Renal cysts may be incidentally observed in adults as a common finding. The diagnosis of simple cyst, acquired renal cyst, and ADPKD can be made due to the observation of renal cysts on the ultrasound of an asymptomatic adult. A comprehensive history and physical examination appear crucial to establish a definite diagnosis. Additionally, other clinical findings, including hypertension, renal failure, or liver cysts, must be considered.
Differential diagnosis
The prevalence of simple renal cysts escalates in regard to the patient’s age. Computed tomography (CT) or magnetic resonance imaging (MRI) is sensitive imaging methods, commonly used to detect cysts. Approximately, 50% of males (mean age 66 years) and 35% of females (mean age 63 years) are suspected of having benign simple renal cysts. The correlation between simple renal cysts and impaired kidney function is yet to be understood [8]. Approximately, 5% of all renal cysts in the adult population are parapelvic cysts as a subgroup of simple cysts [12]. They can affect the renal parenchyma along with invading the renal sinus.
Approximately, 20% of ESRD patients present acquire renal cystic disease, as well as the patients with elongated renal failure. Research shows the highest frequency of cyst formation among the patients who are on dialysis owing to ESRD [9]. The normal or even small size of the kidneys is approved for the patients in the literature, despite of the bilateral presence of multiple cysts. On the contrary, renal failure is expected in the advanced stages of ADPKD, and enlarged polycystic kidneys that are several times the normal size are common.
Another benign rare condition which is associated by cyst formation is called “Localized renal cystic disease.” It is characterized by hypertension, flank mass, flank pain, and urinary symptoms, such as hematuria. In order to distinguish between localized renal cystic disease and ADPKD, clinical findings seem helpful. Dissimilar to ADPKD, localized renal cystic disease does not occur in a setting of positive family history, extrarenal involvement is not expected, and the patients are not at the risk of progression to chronic renal failure. Moreover, the cysts are usually formed unilaterally, while ADPKD patients have several cysts in both kidneys. The next differential diagnosis with unknown inheritance is medullary sponge kidney. It is typically characterized by the malformation of the distal collecting tubules accompanied by nephrolithiasis, impaired kidney function, tubular acidosis, and recurrent urinary tract infections. Microcystic dilations are expected [10]. Nevertheless, the patients usually do not develop ESRD [11]. There are several syndromic and genetic conditions associated by cyst formation. ADPKD as the most important genetic differential diagnosis in adults is typically presented by enlarged cystic kidneys in patients with a positive family history. On the other hand, cyst formation in the kidneys in the absence of a positive family history of ADPKD seeks a thorough review of the medical history, physical examination, and radiologic and clinical factors to appraise the clinical characteristics of the possible differential diagnoses mimicking the atypical types of ADPKD [7].
In contrast, autosomal recessive polycystic kidney disease is usually expected in infants. The prevalence of ARPKD is explained as 1 in 20,000 births. The condition may consequently result in deaths in 30% of patients in their neonatal period. Patients typically present with enlarged echogenic kidneys consisting of several cortical cysts. As previously explained, this inherited disorder is resulted from a mutation in PKHD1 gene which is located on chromosome 6. Perinatal manifestations, including Potter’s phenotype, portal fibrosis, and pulmonary hypoplasia, are also expected in the patients [13]. Dissimilar to ADPKD, with few macrocysts without liver involvement, Caroli’s disease and congenital hepatic fibrosis may accompany ARPKD.
Tuberous sclerosis complex may be misdiagnosed with ARPKD. The coexistence of angiomyolipoma with renal cysts is a pathognomonic sign of tuberous sclerosis (TSC). Almost 30% of cases are not characterized with the specific symptoms of TSC, who are mistakenly diagnosed with ADPKD.
Von Hippel-Lindau syndrome is another hereditary condition characterized by the formation of tumors and cysts in multiple organs. Moreover, the presence of hemangioblastomas in the central nervous system and retina, pheochromocytoma, and multiple renal cell carcinomas is expected. The patients are at a high risk of developing papillary cystadenomas of the epididymis or multiple cysts in their pancreas.
The presence of renal cysts associated with renal dysfunction in adulthood may lead to the diagnosis of autosomal dominant medullary cystic disease. Interstitial fibrosis is routinely observed in normal- to small-sized kidneys. Additionally, early hyperuricemia and gout are common findings.
Furthermore Bardet–Biedl syndrome is defined as the diagnosis of polycystic kidney disease in addition to the extrarenal defects. For instance, retinal degeneration leading to vision loss, mental retardation, early obesity, polydactyly, and urogenital tract malformation may be observed.
ARPKD is a leading cause of pediatric CKD and end-stage renal disease with considered morbidity and mortality rates. However, the phenotype variability has yet to be understood. Due to the broad spectrum of PKHD1 mutations, most patients are compound heterozygotes, meaning they have two various mutant alleles. However, characterizing the functional effect of any specific mutant allele can be challenging. In 2002, Ward et al. thoroughly evaluated the genetic basis in 14 probands clinically suspected of ARPKD. They detected six truncating and 12 missense mutations in patients with polycystic kidney disease 4 (OMIM# 2632000). Surprisingly, three siblings were identified in a pedigree with compound heterozygosity, affected by ARPKD (OMIM# 606702.0005) initially presented in adulthood. The brother was suffering from Caroli’s disease. The two sisters had congenital hepatic fibrosis, one of whom had a single renal cyst; and the other sister had multiple renal cysts [14]. In our presented case, a homozygous missense mutation in PKHD1 gene was identified in a patient who exhibited disease symptoms for the first time in adulthood. Consistent with this finding, Rossetti et al. reported that the majority of missense mutations lead to milder disease, whereas two truncating mutations often, but not always, result in a severe phenotype [15]. Additionally, substantial phenotypic variability exists among affected siblings, proposing that genetic modifiers influence disease manifestation. For instance, in a study involving 126 unrelated families with more than one affected child, 20 sibships demonstrated widely discordant phenotypes, with one sibling experiencing perinatal lethality and the other surviving into childhood [16]
Basically, parental consanguinity is a predicting factor for the increased prevalence of homozygote mutations in the next generations. However, phenotype variability among family members is considered a challenge regarding genetic consultation.
ARPKD is usually detected in neonates or infants for the first time; however, it is possible to be detected an adults, as we faced in our presented case. Contrary to our presented case, research shows that hepatic symptoms such as hepatomegaly and portal hypertension are more common than renal symptoms in adult-onset ARPKD. In such cases, although the hepatocytes have standard structure and function, the biliary ductal plate has some malformations, including periportal fibrosis and bile duct proliferation. Renal symptoms in older patients include proteinuria, renal insufficiency, renal cysts, and nephrolithiasis. Kidney imaging usually shows nephromegaly, poor differentiation of kidney echo, and medullary kidney cysts. According to the literature, congenital hepatic fibrosis, cholangitis, and portal hypertension are also expected in the patients with renal cysts. In 2024, Loeb et al. evaluated 24 patients with a median age of 51 years, duo to their hepatic complications. Imaging studies along with histologic studies confirmed marked renal cysts suggesting ARPKD in 91.3% of them [17].
Considering the burning ambition to overcome the burden of genetic disorders in the next generation, in addition to achieving a particular diagnosis and selecting the most appropriate treatment strategy, genetic analysis of patients with hereditary disorders seems beneficial. The definite diagnosis of ARPKD is based on the findings of molecular genetic evaluation of the PKHD gene, identifying the pathogenic variants. In this regard, mainstream PCR-based sequencing of the causative exons plays a crucial role. However, the current trend is toward applying WES for ARPKD genetic analysis [18].
Park, Ryu et al. in 2020 [19] conducted a multicenter cohort, aiming to broadly evaluate the clinical and genetic aspects of patients suffering from inherited cystic kidney disease. The prospective study is likely to be accomplished in three years (May 2020–May 2022). According to their published initial proposal, they set out to identify the cases of inherited cystic kidney conditions. As regards, a targeted gene panel of cystogenesis-related genes, WES, and/or family segregation studies were performed.
In 2018, Bullich et al. [20] comprehensively approached the genetic diagnosis regarding cyst formation and glomerular involvement related to hereditary kidney disease in 421 patients. A cost-effective, thorough kidney disease gene panel consisting of 140 genes causative or related to the inherited cystic or glomerular kidney disease was suggested considering their data in order to provide an accurate genetic diagnosis as well as facilitating genetic counseling for the next generation. The advantages and marked sensitivity of the WES method were highlighted by their findings. Nevertheless, WES did not appear to be an accurate diagnostic tool in order to screen of mutations in the main causative gene, PKD1, as almost six pseudogenes were identified for it. In agreement with our data, they reported the superiority of early-onset renal manifestations in ARPKD patients compared to the late-onset phenotype, which is chiefly expected in ADPKD patients.
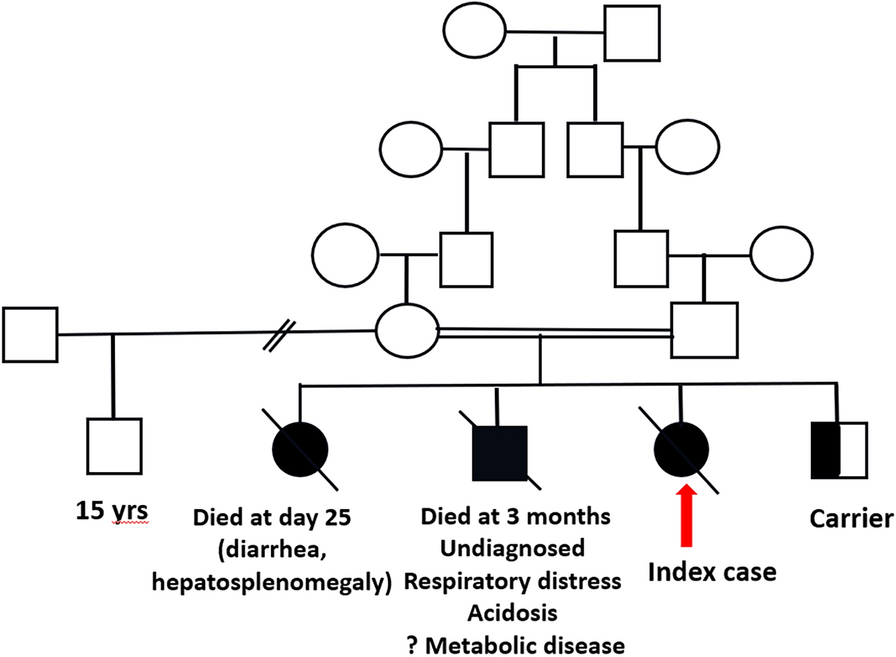
A retrospective study in the USA in 2017 showed that about 21.7% of patients with ARPKD had at least one affected sibling as we saw in our presented case who had a sister with kidney cysts and nephrolithiasis.
The cross-sectional study conducted by Bugmaier et al. [21] in 2019 included a comprehensive assessment of the clinical aspects of ARPKD in young adults. Relatively, ARPKD was diagnosed within the first two years of life or in the prenatal period in three-quarters of their study population. There was only one adult affected patient, diagnosed later at the age of 54 years due to the incidental finding of a renal cyst on ultrasound. The diagnosis was confirmed by genetic studies.
Alawi et al. in 2020 conducted a cohort study in Oman, evaluating the genetic features in 45 clinically suspected ARPKD cases along with their unaffected siblings and parents. Their findings fully endorsed the NGS techniques followed by Sanger sequencing, as though the diagnostic strategies are improved using the methods. Additionally, the early-onset of renal symptoms was demonstrated through their findings. As they reported, five affected individuals out of their study population were diagnosed prenatally, 24 within the first year of their life, and 11 during childhood [4].
A positive aspect of genetic testing in patients diagnosed with ARPKD is that we can approach the other possible diagnoses as well. For instance, in 2017, physicians in Washington conducted a study in order to investigate the kidney disease in 97 individuals with the age of 0.6–36 years old who had been diagnosed with Joubert syndrome. Their analysis showed that the phenotype of ARPKD and Joubert syndrome were overlapped in approximately 35% of cases. However, they did not identify any adult patients diagnosed with ARPKD. In 2020, Molinari et al. [22] reported a 24-year-old female case of polycystic kidney disease with atypical presentations. Similar to our method, a combination of NGS and Sanger sequencing was used to make the final diagnosis of ARPKD. Moreover, two heterozygote changes in the PKHD1 gen were identified. The report highlighted the positive usage of urine-derived renal epithelial cells (URECs) in regard to the RNA and microscopic studies with the goal of making a precise diagnosis.
Unfortunately, limited data are available regarding the prognosis and the management practice of adult-onset ARPKD due to its rarity and broad spectrum of symptoms and comorbidities. Our proband had a normal kidney function according to her calculated GFR. Nevertheless, Reddy et al. revealed a case report, presenting a young male with ARPKD, who was asymptomatic at birth and during the infancy. However, ARPKD was complicated by CKD at the age of 13 in the patient [23].
On the whole, ARPKD is a rare disease leading to the early loss of renal function, and it may cause a lifelong dependency on renal replacement therapy. Hence, prevention must be over-emphasized, and as observed in the presented case, there is no certainty that a patient with adult-onset polycystic kidney disease is never suspicious of ARPKD. As demonstrated by discordant siblings, phenotypes cannot be simply attributed to genotype; instead, they likely involve interactions with other genes and epigenetic factors (e.g., alternative splicing and environmental factors) [16]. A thorough medical history and precise family pedigree seem helpful so as to make the exact diagnosis. However, in terms of adult-onset ARPKD cases, proband’s parents are usually old. Since simple renal cysts are expected to be incidentally and normally discovered in the elderly, imaging and physical examination fail to arm the physician with a definite family history, likewise our presented case. Thus, it is strongly recommended that patients who are diagnosed with adult polycystic kidney disease undergo genetic evaluation and avoid blind genetic consultation, thereby preventing the birth of an infant with ARPKD in the next generation. For better illustration, the discussed studies are summarized in Table 3.
Table 3 A summary of discussed studies





留言 (0)