Wolman disease is a rare autosomal recessive lysosomal storage disorder that presents early in life. It is caused by a deficiency of LAL that metabolizes triglycerides and cholesterol esters, thus patients had elevated levels of triglycerides and cholesterol, resulting in deposition of lipid esters with excessive amounts in most tissues particularly the liver, intestine, lymph nodes, adrenal glands, and spleen [3].
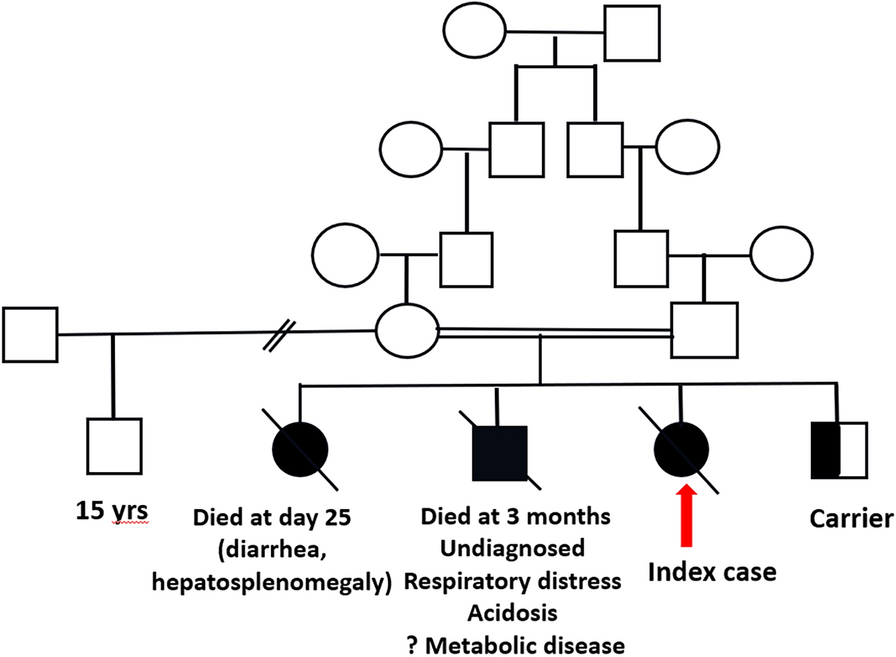
The diagnosis of WD in the reported case was complicated first by the presence of diagnostic criteria of HLH (5/8 criteria): bicytopenia, hemophagocytosis, hypertriglyceridemia, high ferritin, and high soluble CD25. Some features of WD were overlapping with HLH; hepatomegaly, hypertriglyceridemia, and abnormal liver function tests. Secondary HLH to WD has been anecdotally described in 14 reports (19 patients) (Table 2). Except for two patients, who were diagnosed early and received ERT followed in one of them by HSCT, all the other patients died in less than 2 months after their admission whether with or without HLH treatment which was considered inefficient in these cases. The patients aged from 26 to 180 days (median 90 days) and are mostly from consanguineous families [1, 2].
Table 2 Summary of reported cases of WD with HLHIn the current study, the confirmation of diagnosis was reached by NGS which revealed a previously reported pathogenic homozygous missense variant c.398del; p. (Ser133Ter) which interrupts the reading frame by a premature stop codon wielding a truncated protein. This variant has been reported in Clinvar (RCV000801965.11).
The patient deletion mutation is in line with previous reports that indicate that CESD patients typically had missense mutations, with some residual enzyme activity (3–8%) [4] while WD had very low or absent LAL activity and could be due to several dozens of mutations in the LIPA gene; that is, deletions, insertions, and nonsense mutations [21].
The accumulation of cholesterol ester may play a role in inducing inflammasome activation in macrophages, leading to secondary HLH [11]. In all previous reports of WD with HLH, the patients were treated for HLH, and the diagnosis of LAL was reached later either through detecting a calcified adrenal or due to low LAL activity or due to the presence of mutation on performing genetic analysis [2].
A previous report from Egypt by Elaraby et al. [22] has reported three mutations (p.Gly87Val, p. Asp352del, and p. His374Gln) in seven patients from five unrelated families; however, none of them presented with HLH. Meanwhile, the study by Elsayed et al., 2016, confirmed WD diagnosis in three Egyptian patients presenting with HLH and had no mutations in hereditary familial hemophagocytic lymphohistiocytosis genes but had LIPA gene variants p.W130X, p.S112X, and p.W289X [14].
Treatment of HLH is critical and should begin as early as possible to prevent irreversible organ damage. The conventional treatment consists of a potent immunosuppressant, chemotherapy, a standard of care, and the only curative treatment after remission is allogeneic HSCT which improves overall patient survival [17]. Untreated WD patients are poor candidates for HSCT as they are severely malnourished, with an ongoing inflammatory process, and have significant, rapidly progressive liver disease [18]. The chemotherapeutics used during the conditioning cause liver toxicity and the long turnover time of tissue macrophages (liver macrophages survive > 1 year) may cause unfavorable outcomes [23]. Data on HSCT are debatable as there is only a short-term survival benefit [24]. Thus, HSCT in WD has a prohibitively high treatment-related mortality and poor outcome [18, 20]. Similar to other cases that reported WD and secondary HLH, the patients usually showed refractory responses to multiple therapies [17]. Recently, Emapalumab (a monoclonal antibody directed against interferon-gamma) has been shown to be safe and effective in treating recurrent, progressive, or refractory primary HLH or cases who are intolerant to conventional treatment. There are currently ongoing clinical trials to study the efficacy of Emapalumab in treating secondary HLH. This can be a key factor for managing patients with WD and HLH [17].
As early treatment is mandatory for favorable outcomes, early patient diagnosis is required. Fateen et al. [25] diagnosed a patient with LAL deficiency using a dried blood spot (DBS) after screening 53 patients with hepatosplenomegaly, anemia, and failure to thrive to assess enzyme activity. Their study proved DBS to be an accurate and efficient method for diagnosis of WD especially in suspected cases with overlapping phenotype.





留言 (0)