
記住我


Primary treatment was surgery in 39 patients (Table 1) and the vast majority received surgery outside of experienced centers (33/39, 84.6%). 69.2% of all patients with resection revealed no distant metastasis at diagnosis (N0M0, n = 26; N1M0, n = 8) and all patients with N0M0 status received a tumor excision. First surgery resulted in positive margins in 25/39 (64.1%) patients. However, in those patients with resection biopsy (n = 31, 79.5%), residual tumor was found in 25 of 31 patients (81%) (R1: 20, R2: 5). Of note, the median tumor size was 3.3 cm in patients with resection biopsy.
A biopsy was performed in 12 patients (median size at biopsy: 6 cm, all but one > 3 cm). In eight patients CCS was resected after biopsy, all with R0 status, except one with R1. In three cases resection was not performed due to multifocal progression at distant sites (M + :3) and in one case the resection status was unknown due to short follow-up (< 1mos, N + :1).
Sixteen patients with incomplete resection of local disease (of n = 26 in total N0M0 cohort, Table 1) were converted into R0 resections with 71.8% (n = 28) of all patients finally receiving R0 resections (Table 1). Two patients received an amputation of their lower leg, and one patient underwent exarticulation of the proximal phalanx. Additional local treatment to primary tumor resection was performed in 51% (n = 22).
Lymphadenectomy and sentinel biopsyLymphadenectomy (8 of 11 positives for CCS) was typically performed in patients with visible lymph nodes in pre-surgical imaging studies of the adjacent region. A sentinel biopsy was done in five cases with two samples positive for CCS in immuno-histopathology. These two patients underwent subsequent lymphadenectomy with no evidence of further lymph node metastases in respective surgical specimen.
Isolated limb perfusionTwelve patients underwent isolated limb perfusion with TNF-α and melphalan, of which three cases were treated pre-operatively (all final R0) at small tumor sizes T1-T2 (N0M0 = 2: both with lymph node recurrence after 1.9 years and 6.5 years; time from diagnosis to progression 3.1 and 7 years), and in five cases as additive treatment following R + resection without an option for additional, limb-salvaging surgery (time to recurrence 0.4–1.1 years/ time to progression 0.5–2.5 years). Four other cases received ILP following local, symptomatic tumor recurrence. In all patients, radiologic, metabolic (FDG-PET) and clinical response was observed. However, all patients experienced tumor progression outside the treated region after 0.9–11.8 months). ILP was part of a multimodal treatment strategy including postinterventional resection, whenever possible.
RadiotherapyThirteen patients were identified to have received local radiotherapy as initial therapy. Four of these were treated in a neoadjuvant (one at difficult anatomical location; two with lager tumor size to ensure limb salvage; one patient within palliative context: N1M1; all were followed by R0 resection) and two in an adjuvant setting after R0 resection with close surgical margins (up to 0.1 mm), six cases following positive microscopic margins (all R1) and one as single therapy without resection. The median radiation dose (incl. boost therapy) was 63.2 Gy (range: 50–70 Gy). Boost therapy ranged from 10 to 26 Gy. One patient with N1M0 at diagnosis received radiotherapy of the affected lymph pathways.
Systemic therapyEleven patients were treated with chemotherapy as initial treatment. Six patients with localized disease (n = 1) or locoregional spread (N1: n = 5) received chemotherapy doxorubicin + ifosfamide, dacarbazine + ifosfamide or temozolomide. Two patients received neoadjuvant chemotherapy, one patient due to a large tumor size with 11.1 cm (one cycle of doxorubicin + ifosfamide) followed by tumor resection and the other patient in a palliative setting (with M1 at diagnosis).
Patterns of recurrenceIn 18 of 24 patients with no distant metastases (N all, M0) at diagnosis, CCS recurred (at local site or distant) after a median time of 1.2 years – relapses did not occur beyond three years from time of primary resection with R0 resection status (Fig. 1a, b).
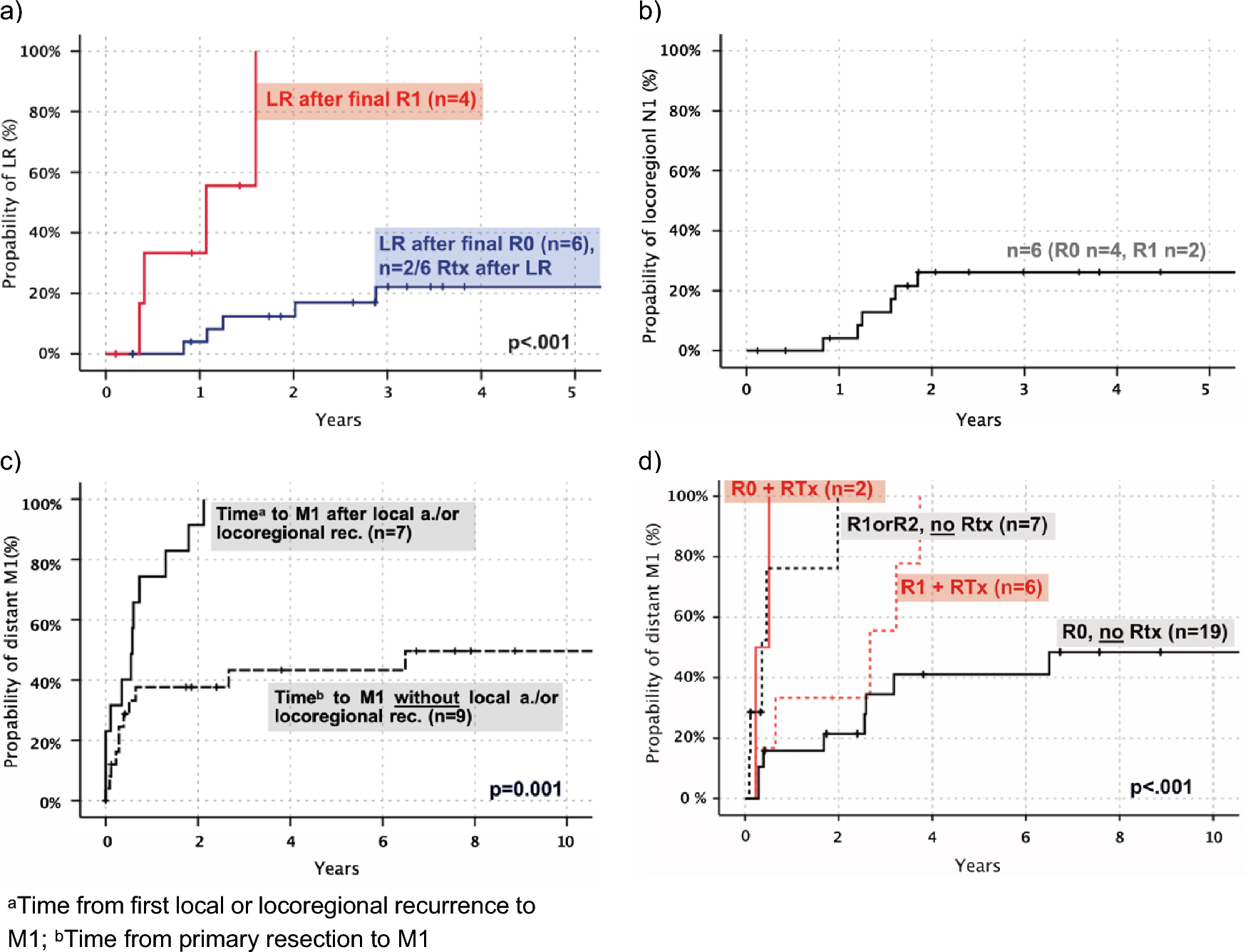
Fig. 1
Patterns of local, locoregional (N1) and distant recurrence (M1) in CCS. a Local recurrence (LR, n = 10, only primary tumor location) in patients with final R0 vs final R1, including two patients with RTx in R0 cohort (time primary resection—recurrence, in years). b Locoregional (N1) recurrence after resection in patients with local disease, N0M0 (time primary resection—recurrence, in years). c Time to distant metastasis after local treatment (R0) for regional relapse (local or N1) compared to patients without regional relapse (time from resection to distant metastasis, in years). d Distant metastasis-free survival for patients with complete (R0) vs incomplete resection (R1 or R2) and postoperative radiotherapy (time primary resection—distant metastasis, in years)
Five-year local recurrence-free survival for all patients was 59%. Patients with R0 resections presented a probability of 22% LR (local relapse) in three years (Fig. 1a). All locoregional lymph node recurrences developed in the first two years with a rate of 26% (R all, initial N0M0) (Fig. 1b). In patients with complete final resection, median time to local recurrence was 1.6 years (n = 6; range, 0.8–12.5yrs), compared to 0.7 years (n = 4; range, 0.4–1.6yrs) in patients with incomplete microscopic resection (only those with R1). Within two years local recurrence occurred in all patients with R1 but only 13% of patients with R0 resection (negative margins) (Fig. 1a).
In total, 19/28 (68%) of patients with complete resection (R0) showed distant metastasis after five years in Kaplan–Meier estimation. Patients with local recurrence were at a much higher risk of developing distant metastasis (all of them show M1 after two years, Fig. 1 c) with a median time to distant metastasis of 0.6 years vs 15.2 years. M1 occurred always after local or locoregional (N1) tumor re-appearance (only one patient with M1 before locoregional N + , ∆ 6.6mos). The primary tumor size did not correlate with distant metastasis (p = 0.475).
Patients with postoperative radiotherapy after R0 resection (n = 2, both at close primary resection) presented with distant metastasis in the first year after resection and patients with R0 and no radiotherapy (n = 19) presented with a median survival of 15.2 years (Fig. 1d). All patients with R1 and radiotherapy showed a metastatic-free survival of 66% vs 40% in the R1 group without radiotherapy at two years (and 0% with R2 included, Fig. 1d). In-field recurrence at local site after primary resection in patients with N0M0 (n = 8) was seen in 37.5% (n = 3) of patients, which included two with R0 (25% in-field) and one with R1 status (follow-up in-field recurrence, range: 0.2–2.7yrs).
In all patients the median time to distant metastasis was 1.1 years. 26% (n = 5) with CCS reappearance developed distant metastatic spread as their first tumor recurrence (median 2.7yrs). At first observation, 14 tumors had spread in only one remote organ: lung n = 5, bone n = 3, soft tissue n = 2, liver n = 1, indefinable n = 1 and in 14 patients, multiple organs were infiltrated. 65.5% of all metastases (n = 29) were thoracic (mostly pulmonary: n = 17, 58.6%), 44.8% (n = 13) were found in the abdominal cavity (mostly hepatic: 13.8%) and 20.7% (n = 6) showed involvement of the spinal system. Half of all pulmonary metastases were observed within the first year of diagnosis (median, 0.96yrs). Both the chest as well as abdominal cavity were infiltrated after 1.4 years in median. CCS progressed four months (in median) after tumor recurrence or five months after initial stage IV (N + and/or M + : 8th edition AJCC staging). 80% of patients with progressive disease died during follow-up. Time from disease progression to death was about half a year (median 6.4mos).
Treatment of local (LR), locoregional recurrence (N1) and distant metastasisAll patients with local recurrence (in total n = 10 with LR) were successfully treated with surgery. In patients with LR two received radiotherapy. Notably, tumor recurrence after surgery emerged in locoregional lymph nodes in seven patients which were clinically diagnosed by ultrasound. All of them underwent lymph node dissection which revealed CCS-positive lymph nodes. Additionally, six patients with positive lymph node removals received radiotherapy of the corresponding region.
Distant metastases were treated with surgery in eight patients, and 21 patients with metastatic disease received chemotherapy in a palliative intention. Only one of those patients experienced tumor regression with doxorubicin + ifosfamide in combination with hyperthermia. Further treatments of metastatic CCS included checkpoint inhibitors such as ipilimumab, nivolumab and pembrolizumab, the kinase inhibitors crizotinib, pazopanib and sunitinib, as well as experimental treatments with treatment durations ranging from less than a month up to one year.
Overall survivalOS for all patients was 3.6 years in median with a 5-year survival rate of 42% (10-year survival 38%) (Fig. 2) and 52% for initially localized CCS (10-year survival 44%). All patients died of CCS or GINET. Only five patients with distant metastasis (n = 28) were alive at follow-up (median follow-up to survival 3.8yrs). Four patients survived more than ten years (follow-up: 12.5—26.9yrs). One of four patients was disease-free until distant M + showed up after 15 years (follow-up other three patients 12.5—26.9yrs). All of them were primarily localized and underwent complete resection (R0) as single therapy; only one received adjuvant ILP and CTx (regimens: ifosfamide, dacarbazine).
Fig. 2
Overall survival (OS) depending on tumor size, staging at diagnosis and final R status in Kaplan–Meier estimation. a OS for all patients (time: diagnosis CCS—death, in years). b OS for all tumor sizes (T) only in patients with local disease (N0M0) and with final R0 (time: diagnosis CCS—death, in years). c OS depending on initial staging: local disease vs locoregional spread vs distant metastasis for all patients (time: diagnosis CCS—death, in years). d OS for final R0 vs final R + (R1 or R2) with localized disease at diagnosis in Kaplan-Meier estimation (N0M0) (time: diagnosis CCS – death, in years)
留言 (0)