
記住我


A total of 78 patients were included in the study. 79% (n = 62) of the patients were male, and the median age was 67 years (range 49–89; Table 1). The etiology of HCC was mainly alcoholic steatohepatitis (ASH) or mixed ASH/metabolic dysfunction-associated steatohepatitis (MASH), 30.8% and 12.8%, respectively). Liver cirrhosis was diagnosed in 83.3% of the patients. BCLC stages A, B, and C were evident in 3.8%, 65.4%, and 30.8% of the patients, respectively. The median MELD score was 8 (6–20), and the median ALBI score was − 2.68 (-3.56- -1.09). 53 (55%) patients were pretreated: 31 with TACE, 1 with TARE, 8 with systemic therapy, 2 with resection, and 1 with radiofrequency ablation.
Table 1 Baseline patients’ characteristicsThe baseline patient characteristics from the SORAMIC trial are presented in Supplementary Table S1. The SORAMIC subgroup included significantly more males (92.8% vs. 79.5%, p = 0.020) and a higher number of patients with BCLC stage C (68.7% vs. 30.8%, p = 1.86 × 10− 6) than our study cohort.
A total of 47 (60%) patients in the study cohort and 73 (88%) patients in the SORAMIC trial died during the observation period (p = 5.95 × 10− 5). The median overall survival times were 36 weeks (4-436) and 44 weeks (7-167), respectively (shown in Supplementary Figure S1). In the study cohort, the overall survival rate after TARE was 5.2 ± 4.9%, 12-week survival rate was 89.5 ± 3.5%, and 24-week survival rate 70.9 ± 5.4%. In the SORAMIC trial, the overall survival rates were 0%, 97.6 ± 1.7% for 12-weeks and 79.5 ± 4.4% for 24 weeks.
Biochemical parameters, liver function scores and cytokine levels before and after TAREIn the total population, there were significant changes in GGT levels (p = 5.44 × 10− 7), bilirubin levels (p = 4.80 × 10− 6), platelet count (p = 0.004), and MCP-1 levels (p = 0.008) between baseline and week 4 after TARE (Table 2). The mean ALBI score was also significantly higher after TARE (p = 1.30 × 10− 6).
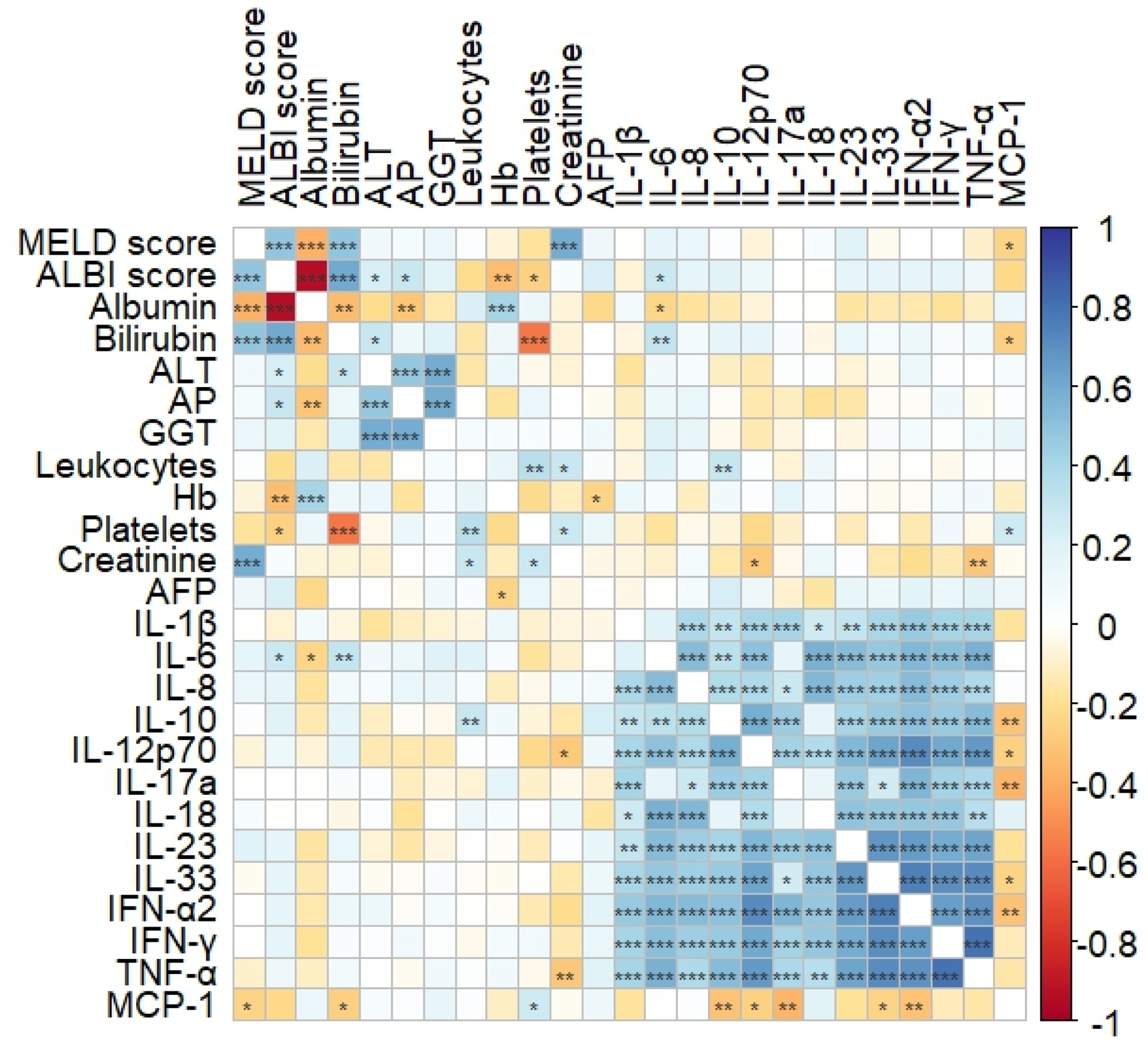
Table 2 Blood parameters and serum cytokine concentrations before and at week 4 after TARE. Values are shown as median and rangeBefore TARE, pro-inflammatory cytokines such as IL-12p70, IL-17a, IL23, and IL-33, as well as the anti-inflammatory cytokine IL-10, showed intermediate to high correlation with the interferons IFN-α2, IFN-γ, and TNF-α, which are known to be associated with apoptosis, cell proliferation, and cell differentiation. There was a weak correlation of IL-6 with ALBI score (r = 0.276, p = 0.016), albumin (r=-0.230, p = 0.045) and bilirubin (r = 0.306, p = 0.007). IL-8 showed an intermediate correlation with IL-6 (p = 0.524, p = 1.21 × 10− 6), IL-1β (r = 0.392, p = 0.0005) and IL-10 (p = 0.379, p = 0.001) (shown in Fig. 1).
Fig. 1
Correlation matrix of biochemical parameters, cytokines and liver function scores in patients with HCC before TARE. The intensity of the colors indicates the Spearman’s correlation coefficient between two parameters. The asterisks display the p-values with * p < 0.05, ** p < 0.01 and *** p < 0.001. Significance was tested using a Pearson correlation test and level of significance was set at p < 0.05. ALBI: albumin-bilirubin, ALT: alanine aminotransferase, GGT: gamma-glutamyl transpeptitase, Hb: hemoglobin, IFN: interferon, IFN-g: interferon gamma, IL: interleukin, MCP-1: monocyte chemoattractant protein-1, MELD: model for end-stage liver disease, TNF: tumor necrosis factor
Association of biochemical parameters, liver function scores and cytokine levels with 12-week and 24-week survival after TAREBaseline IL-8 levels (309.80 vs. 40.50 pg/mL, p = 7.40 × 10− 4 and MELD score (10 vs. 6, p = 0.017) were significantly higher in patients who died 12 weeks after TARE than in those who survived (shown in Supplementary Table S2).
ROC analysis was performed to determine how accurately IL-8 and the liver function scores ALBI and MELD could discriminate between patients with and without survival ≥ 12 weeks after TARE (shown in Fig. 2). The best performance was observed for baseline IL-8, with an area under the receiver operating characteristic curve (AUROC) of 0.861 (p = 0.002), followed by the MELD score with AUROC = 0.799 (p = 0.009) and ALBI score with AUROC = 0.735 (p = 0.041). However, the IL-8 AUROC was not significantly different from the MELD score AUROC (Z = 0.505, p = 0.614) and ALBI score AUROC (Z = 1.499, p = 0.134). The cut-off value for the 12-week survival discrimination for IL-8 was 190 pg/mL, with a sensitivity of 85.7% and specificity of 81.2%. The positive predictive value (PPV) and negative predictive value (NPV) for identifying patients with 12-week survival were 98.2% and 31.6%, respectively.
Fig. 2
Receiver operating characteristics (ROC) curve of the association of IL-8, ALBI and MELD score with 12-week survival after TARE
Median baseline IL-1β levels (5.28 vs. 10.67 pg/mL, p = 0.021) and IL-17a levels (0.54 vs. 2.06, p = 0.031) were significantly lower in patients who died 24 weeks after TARE compared to those who survived (Supplementary Table S3).
Multivariate analysis of factors associated with 12-week and 24-week survival after TAREUnivariate Cox regression analysis showed a significant association between an IL-8 cut-off of 190 pg/mL and 12-week (p = 0.006) and 24-week survival (p = 0.039). The MELD score (p = 0.025) was also associated with 12-week survival. Alterations in the ALBI score, representing liver function, showed no significant impact on 12-week (p = 0.147) and 24-week survival (p = 0.421). In the multivariate Cox regression analysis, the IL-8 cut-off remained independently associated with 12-week and 24-week survival (Table 3).
Table 3 Univariate and multivariate analyses of factors associated with 12-week and 24-week survival after TAREAssociation of the IL-8 cut-off of 190 pg/mL with 12-week and 24-week survival after TARE in the test cohort and in the SORAMIC validation cohortPatients with baseline IL-8 levels above the cut-off of 190 pg/mL had a significantly lower 12-week survival rate after TARE than patients with lower IL-8 levels (66.9 ± 11.1% vs. 98.2%±1.7%, p = 9.27 × 10− 5). Patients’ characteristics of both groups are shown in Supplementary Table S4.
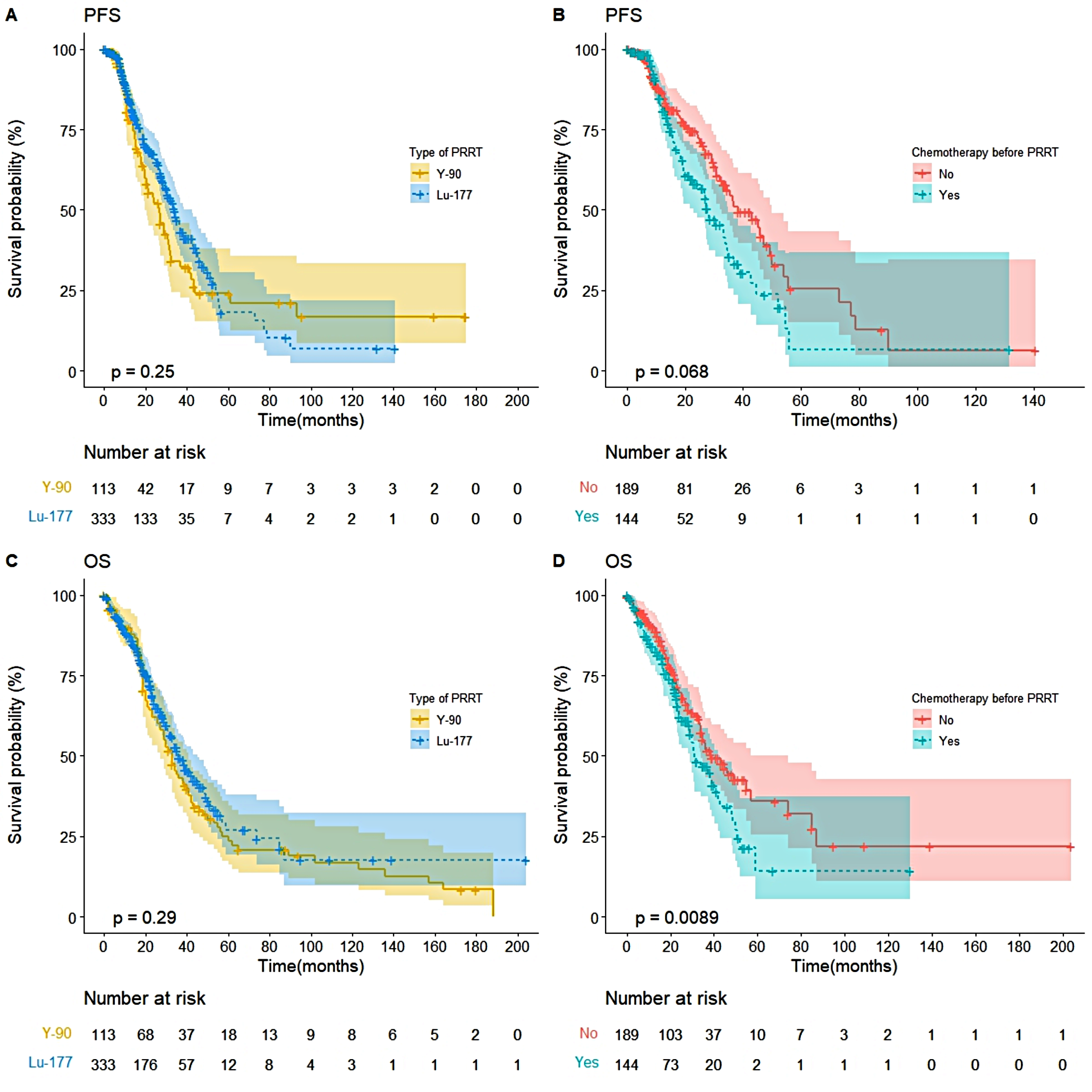
This association was also found for the 24-week survival rates (54.7 ± 11.9% vs. 77.8 ± 5.8%, p = 0.027). Although statistical significance was not achieved, differences in survival rates were observed during the 36-week survival period. Specifically, the survival rate was 54.7 ± 11.9% for individuals with IL-8 > 190 pg/mL, in contrast to 73.0 ± 6.2% for those with IL-8 ≤ 190 pg/mL (p = 0.052) (shown in Fig. 3A-C). Additionally, patients with IL-8 levels > 190 pg/mL before TARE experienced significantly shorter overall survival, with a median survival time of 24 weeks (range: 4-196) compared to 40 weeks (range: 4-436) in patients with IL-8 levels ≤ 190 pg/mL (p = 0.039).
Fig. 3
Kaplan-Meier curves are showing survival of the study cohort at 12 weeks (A), 24 weeks (B) and 36 weeks (C) and of the patients in the SORAMIC trial at 24 weeks (D), 36 weeks (E) and 48 weeks (F) after TARE according to the baseline interleukin (IL)-8 cut-off of 190 pg/mL
In the TARE + sorafenib subgroup of the SORAMIC cohort (n = 83), the IL-8 cut-off of 190 pg/mL was able to distinguish patients at high risk of death from patients at high likelihood of survival at week 36 (41.7%±14.2 vs. 70.4%±5.4%, p = 0.034) and at week 48 (22.2%±12.8 vs. 54.7 ± 5.9%, p = 0.023) after TARE (shown in Fig. 3D-F). Additionally, the median overall survival time significantly differed between patients with IL-8 > 190 pg/mL and patients with IL-8 ≤ 190 pg/mL, with median survival times of 29 weeks (13–114) and 49 weeks (7-167), respectively (p = 0.026).
留言 (0)