
記住我
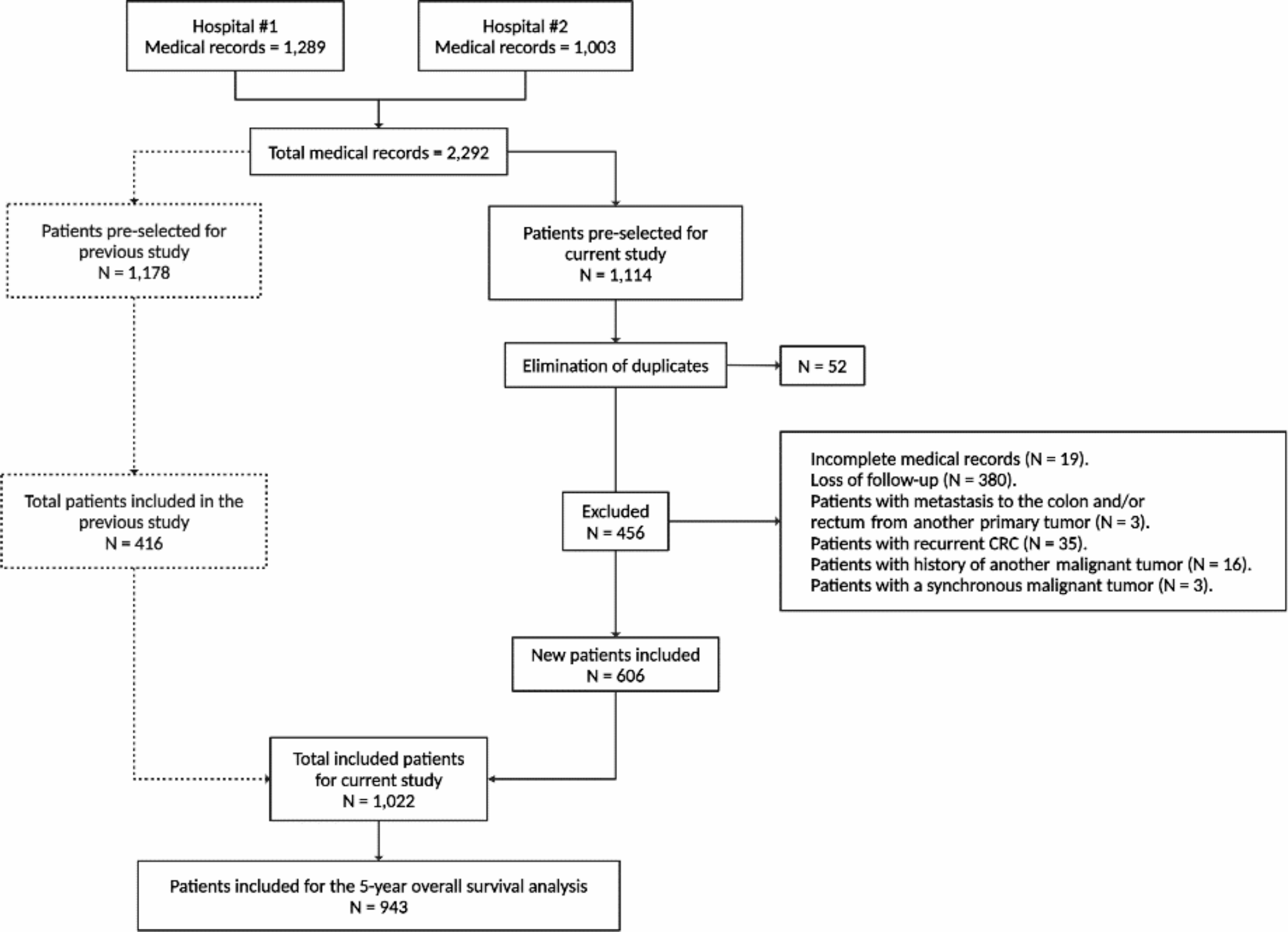
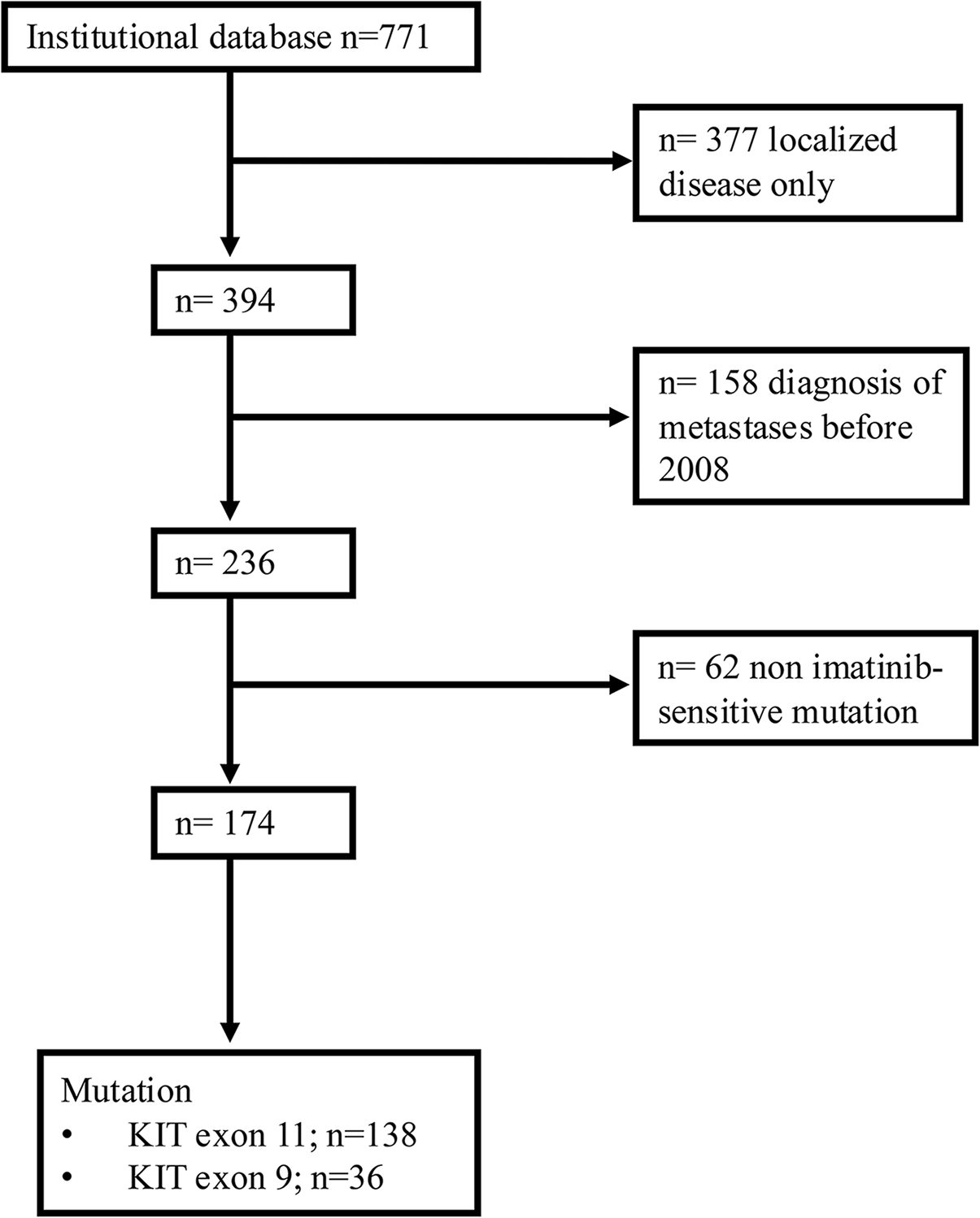

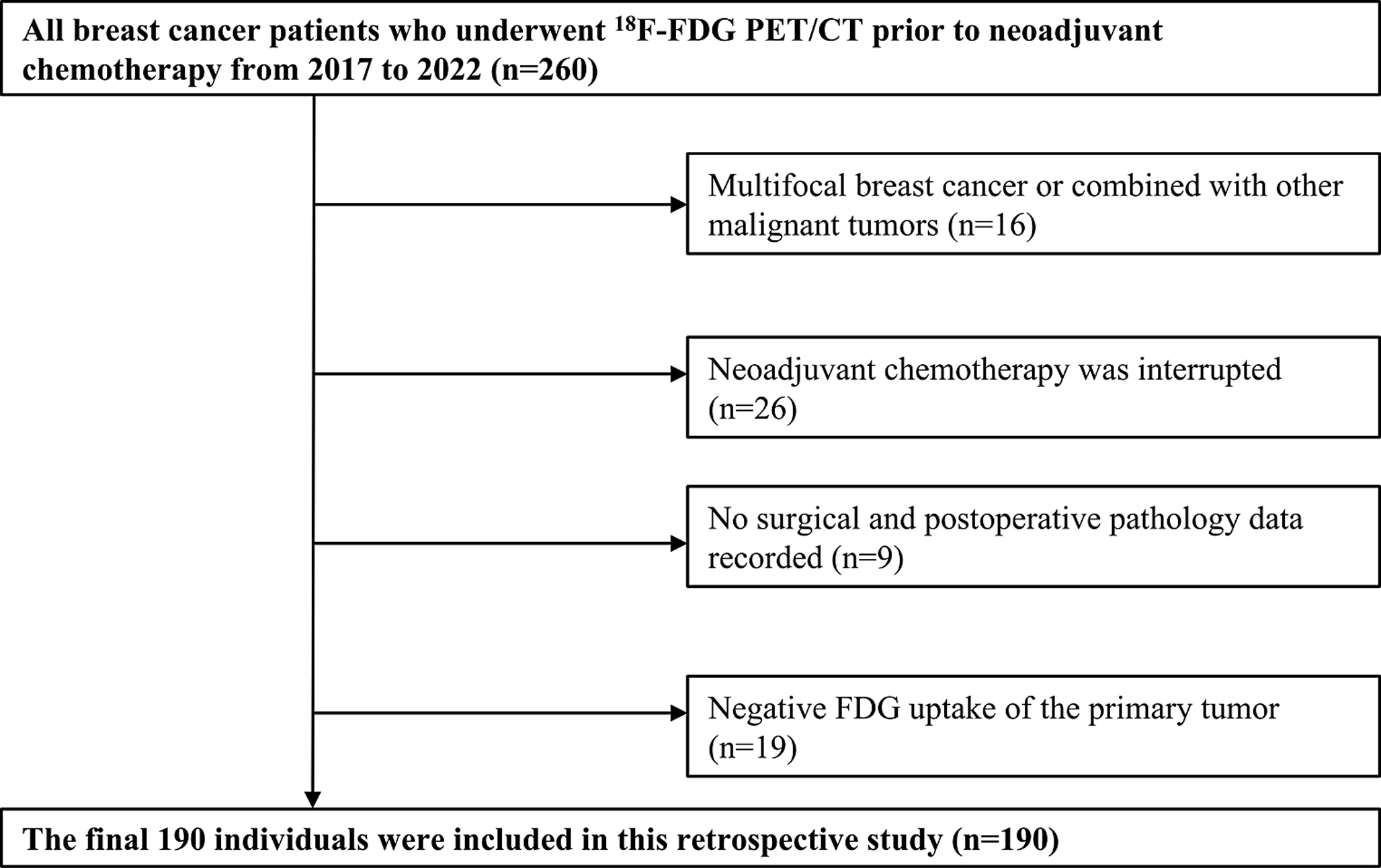

During the study period, a total of 180 adult GBM patients were evaluated. Of these, 51 patients were excluded for the following reasons: poor imaging quality (n = 25), non-adherence to NCCN treatment guidelines (n = 20), and secondary resection (n = 6). Consequently, 129 patients were included in the final analysis, comprising 52 females and 77 males, with ages ranging from 18 to 73 years (mean age: 54 years). Among these patients, 69 experienced recurrence during the study period. The patients were randomly assigned to either a training cohort (n = 90) or a validation cohort (n = 39) at a ratio of 7:3 (Table S2).
Post-operative MRI characteristicsRegarding MRI morphological characteristics, patients in the recurrence group exhibited a significantly greater midline structures displacement (p = 0.017) compared to those in the non-recurrence groups. However, no significant differences were observed between the two groups in terms of tumor location (p = 0.315), corpus callosum involvement (p = 0.817), residual cavity type (p = 1.000), enhanced region (ER) volume (p = 0.175), unenhanced region (NER) volume (p = 0.367), residual cavity morphology (p = 0.204), enhanced pattern (p = 0.689), extent of resection (p = 0.502), and SVZ involvement (p = 0.061). For subregional quantitative mertics, significant differences were noted in ERmean (p = 0.007), ERmedian (p = 0.003), and NERstandard deviation (p = 0.03) between the recurrence and non-recurrence groups (Table 1).
Table 1 Characteristics of patients with GBM in the training and validation cohorts (n = 129 patients)For the evaluation of MRI features, the Kappa values for inter-observer agreement between the two radiologists were as follows: tumor location (0.955), corpus callosum involvement (0.931), midline shift (0.967), MAR (0.934), residual cavity type (0.943), type of residual cavity enhancement (0.921), extent of surgical resection (0.944), and SVZ involvement (0.967).
OutcomeUnivariate analysis in the training cohort identified 12 clinical variables and MRI features as significant factors of recurrence, including SVZ involvement (p = 0.047), corpus callosum involvement (p = 0.001), occipital lobe location (p = 0.001), NERminmum (p = 0.004), NERstandard deviation (p = 0.042), NERmedian (p = 0.01), NERmaximum (p = 0.008), NERmean (p = 0.009), ERmedian (p = 0.004), ERmean (p = 0.008), ERmaximum (p = 0.016), and ER + NER rFLAIR values (p = 0.042). Based on LASSO regression analysis, six potential predictive factors were selected: corpus callosum involvement, SVZ involvement, ERmedian, ER + NERratio, NERstandard deviation, and occipital lobe location (Fig. 3). Ultimately, multivariate analysis identified four significant independent variables: SVZ involvement (p = 0.131), ERmedian (p = 0.02), ER + NERratio (p = 0.08), and corpus callosum involvement (p = 0.001) (Table 2).
Fig. 3
A LASSO feature selection and tuning, where the vertical dashed line indicated the optimal penalty coefficient λ corresponding to the non⁃zero features. B The AUC curve plotted through tenfold cross-validation, with the dashed lines on the left and right representing λ min and λ 1se, respectively. λ min was selected for this study. C The 6 features retained after LASSO filtering and their respective weight coefficients
Table 2 Univariate and multivariate analyses for unfavorable PFS of training cohortNomogram model development and prediction efficiencySignificant variables from the multivariate analysis were incorporated into a nomogram model (Fig. 4A). The C-index was calculated as 0.733 for the training cohort and 0.746 for the validation cohort. The nomogram was compared with various independent variables for predicting recurrence, including corpus callosum involvement, ER + NER rFLAIR values, ERmedian, SVZ involvement, and the nomogram score (Table 3). Two representative GBM patient cases are illustrated in Fig. 5.
Fig. 4
The combined model was constructed and presented as a nomogram. A Decision curve analysis of the nomogram score and each independent predictor predicting PFS in the training (B) and validation (C) cohorts. The y-axis represents net benefit, and the x-axis represents threshold probability. Decision curves show that when the threshold probability is greater than 0.13 (red dotted line), the column-line graph (green line) has more benefit than all patients with a positive clinical outcome (red line) or no positive clinical outcome (brown line). Calibration plots of the nomogram. The diagonal line indicates the ideal value, and the solid line represents the performance of the nomogram; the closer the solid line is to the diagonal dashed line, the better the calibration will be. The calibration curves demonstrated good calibration of the nomogram in the training group (D) and validation group (E). Kaplan–Meier curves based on the Nomo-score (cut-off value of 112.69) for PFS in GBM patients (F, G). PFS, progression-free survival. GBM, glioblastoma. ER, enhancing region outside the residual cavity; NER, non-enhancement region outside the residual cavity
Table 3 The C-index of prognostic factors and nomogram for prediction PFS in the training and validation cohortsFig. 5
Two presented cases of GBM patients who had distinctly different PFS time (2 months vs. 15 months) with similar clinic pathological features showed significantly different nomo-scores (154.54 vs. 115.92; P < 0.001). PFS, progression free survival; OS, overall survival; ER, enhanced regional outside the residual cavity; NER, non-enhancement region outside the residual cavity; SVZ, subventricular zone
The AUCs for predicting recurrence in the training group were as follows: clinical model 0.650, conventional MRI model 0.700, FLAIR value model 0.793, clinical + conventional MRI model 0.743, nomogram model 0.806, and the combined model 0.866. The AUCs in the validation cohort were: clinical model 0.536, conventional MRI model 0.799, FLAIR value model 0.531, clinical + conventional MRI model 0.813, nomogram model 0.818, and combined model 0.732 (Table S3).
Decision curve analysis showed that the nomogram score provided the greatest benefit when the threshold probability was above 0.13, with the highest net gain compared to other predictors. Calibration curves demonstrated good agreement between predicted and actual 1-year recurrence rates in both the training and validation cohorts using the nomogram with quantitative metrics derived from FLAIR hyperintensity subregions (Fig. 4B–E).
Based on a Nomogram cut-off score of 112.69, GBM patients were stratified into high- and low-risk levels. Approximately 50% of patients were classified as high-risk level. Kaplan–Meier curves analysis revealed that patients in the low-risk level had a significantly lower recurrence rate compared to those in the high-risk level (p < 0.001 for the training cohort, p = 0.025 for the validation cohort) (Fig. 4F, G).
留言 (0)