
記住我
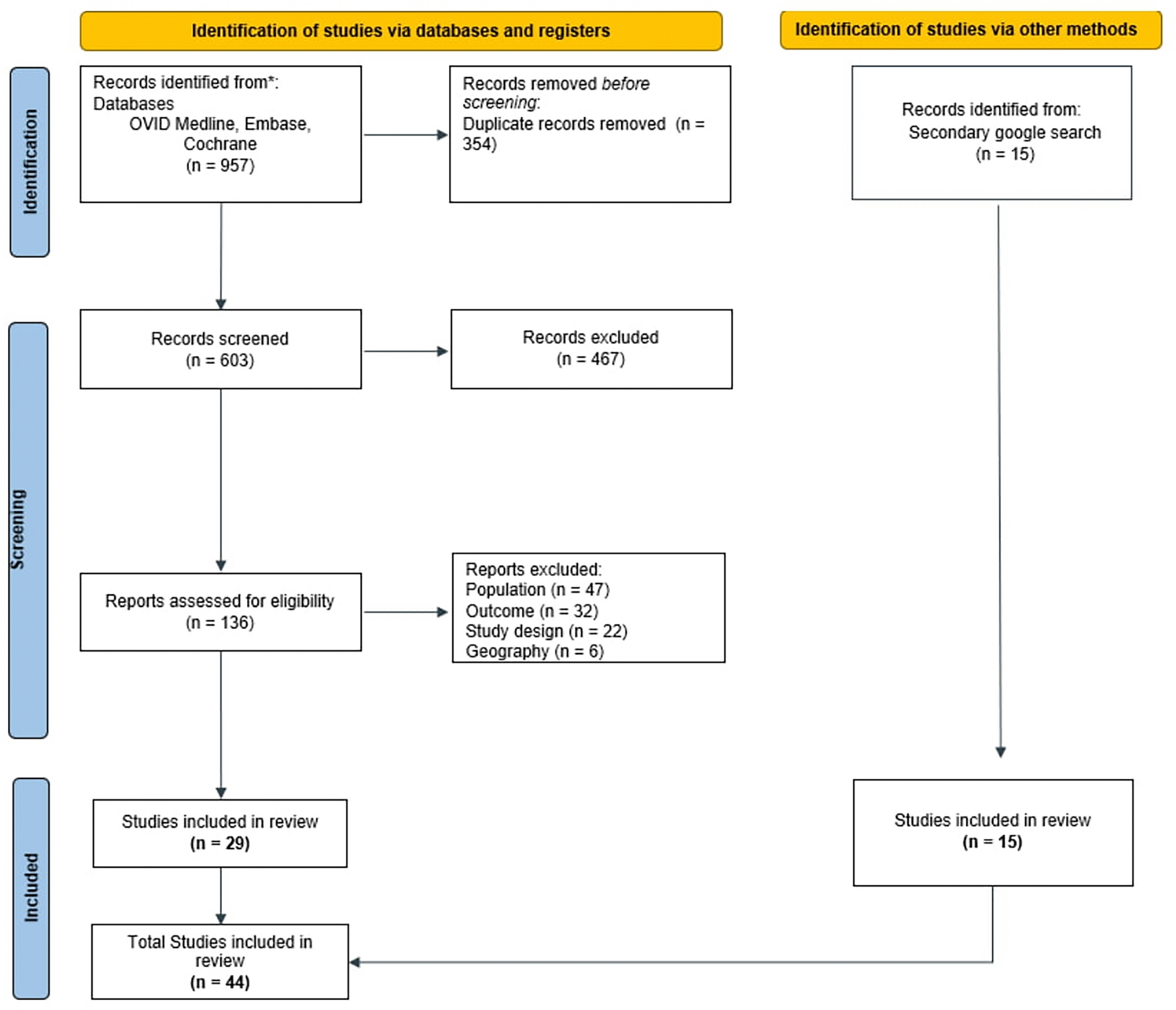

A total of 19,088 prospective participants enrolled in the PSP between March and December 2022 were contacted. There were 2834 completed screenings, resulting in 604 who were eligible to participate (Fig. 1). The most common reason for ineligibility was sustained treatment with galcanezumab for longer than 6 months (n = 1564). Of the 604 prospective participants who met eligibility criteria, 515 provided informed consent, and 500 completed the survey (250 identified as having EM and 250 as having CM); survey completers comprised the analytic sample. Recruitment of participants was stopped after 500 surveys were completed. Missingness for most of the variables ranged from 0 to 2.7% missing, but one variable (the extent to which participants’ source of information agreed with what HCP told them) had 14% missing.
Fig. 1
Patient disposition is presented. *Some respondents were disqualified on more than 1 criterion. **Respondents were only ineligible once the EM quota (n = 250) was reached. CM chronic migraine, EM episodic migraine, PSP Patient Support Program
Participant CharacteristicsOverall, 90% (n/N = 450/500) of participants were women, and 90% (n/N = 448/500) were White, 92% (n/N = 459/500) had at least some college education, and 73% (n/N = 366/500) were employed full time (Table 1). The mean age of participants at the time of the survey was 40.6 (± 12.0) years, and the mean time since the first migraine episode was 18.1 (± 12.7) years. The sociodemographic characteristics of the participants who later were characterized as having EM and CM at the time of the survey were similar (not shown).
Table 1 Participant demographicsThe most common comorbidities reported were anxiety disorder (n/N = 25/500; 45%) and depression (n/N = 218/500; 44%) (Table 2). A migraine family history (immediate family member) was present in 59% (n/N = 295/500) of the participants. Clinical characteristics are summarized in Table 2.
Table 2 Clinical CharacteristicsPrior to DiagnosisOverall, 71% (n/N = 357/500) of participants suspected that they had migraine before diagnosis was made. Among these participants, the most prominent sources that they relied on for information on migraine before diagnosis was advice from friends or family (n/N = 156/357; 47%) and internet search engines (n/N = 101/357; 28%). Other sources reported by participants are shown in Table 3. Participants reported either that they suspected they had migraine, or had a relative or a healthcare professional suggesting they have migraine (Table 3). Others who suggested migraine included a friend, a coworker, and teacher or school staff (Table 3).
Table 3 Path to diagnosisPatient Reluctance to Seek Professional HelpThere were 357 participants who suspected that they had migraine prior to diagnosis, and who were asked whether they were reluctant to seek professional help for migraine attacks. Of these, 109/375 (31%) expressed reluctance. Overall, the most common reasons that participants gave for being reluctant to seek professional help for migraine were that they did not think a physician could do anything more for their migraine attacks (n/N = 35/109; 32%), did not think the physician would take them seriously (n/N = 35/109; 32%), and that they had a previous experience with a physician that was not helpful (n/N = 35/109, 32%) (Table 3). Very few participants (n/N = 4/109; 3.7%) reported that migraines did not interfere with their daily routine.
Of those reluctant to seek professional help, 20 participants (n/N = 20/109; 18%) believed that migraine attacks were due to factors that they could control. The majority of these participants believed that they could control their migraine by changing their diet (n/N = 16/20; 80%), reducing stress levels (n/N = 14/20; 70%), using over-the-counter (OTC) medications (n/N = 13/20; 65%) or by improving their sleep routine (n/N = 13/20; 65%). Participants also felt that they could control migraines using relaxation techniques (n = 6/20; 30%), with supplements (n/N = 5; 25%), or by exercise (n/N = 4/20; 20%) (Table 3).
Seeking Professional Help for MigraineA total of 357 participants described the factors that led them to seek professional help for migraine. The three most prominent factors, selected by > 70% of participants, were increases in headache frequency (n/N = 276/357; 77%), increases in severity (n/N = 263/357; 74%), and migraine attacks interfering with work or school (n/N = 266/357; 75%) (Table 3).
Diagnoses Other Than Migraine and MisinformationFactors during the patient’s journey before later receiving their first CGRP-mAb for migraine prevention included their experiences in healthcare settings, beliefs about how they would be treated, beliefs about migraine triggers, and their ability to control their migraine attacks, as summarized in Table 4. Overall, the mean number of healthcare providers seen since the first migraine episode but prior to a diagnosis of migraine was 4.1 (± 4.3), with a median of 3 and a range of 1–35. Of the 500 participants, 99 (20%) reported that they initially received an alternative diagnosis prior to their migraine diagnosis. Most participants were diagnosed with migraine by a primary care or family practice physician (n/N = 256/500; 51%) or a neurologist (n/N = 178/500; 36%), as described in Table 4. The majority (> 50%) of the 99 participants who initially received an alternative diagnosis did so from a primary care or family practice physician, and 18% (n/N = 18/99) reported a different diagnosis provided by a neurologist. HCPs who provided an alternative diagnosis are shown in Table 4.
Table 4 Migraine DiagnosisThe main sources that participants reported for information on migraine changed once participants received a migraine diagnosis. After diagnosis, most participants reported getting their information from internet search engines (n/N = 208/500; 42%) or specialized or scientific publications, as interpreted by the participant (n/N = 92/500; 18%) (Table 4). Participants reported that their sources of information agreed with what their HCP told them most of the time (n/N = 232/500; 46%) or sometimes (n/N = 136/500; 27%) (Table 4).
Early Migraine EducationThe three most common reasons that participants reported that HCPs had given as causing migraine were stress, anxiety, or depression (42%), hormonal changes (30%), and “don’t know” (29%), where “don’t know” means that the participant did not know the answer to the question. (Table 4).
Forty percent (n/N = 198/500) of participants reported that their HCP informed them that reducing triggers would control migraine attacks and what the participant could expect from treatment (n/N = 190/500; 38%) (Table 4). Only 28% (n/N = 142/500) of participants reported that HCPs informed them OTC pain medications did not treat the disease or prevent future attacks, rather just reduced the intensity of the current attack. They also indicated that the HCPs explained on what basis they diagnosed migraine (n/N = 142/500; 28%), explained the differences between causes and triggers (n/N = 139/500; 28%), explained that overuse of OTC pain medications could make migraine attacks worse over time (n/N = 130/500; 26%), informed them what they felt the cause of migraine could be (n/N = 75/500; 15%), and that migraine had no external cause nor was it a secondary headache (n/N = 50/500; 10%). Most participants reported that the information the HCP provided was in agreement with what they previously thought with regards to how migraine was diagnosed and the evidence leading to the diagnosis (n/N = 112/142; 79%), the difference between causes and triggers (n/N = 108/139; 78%), that reducing triggers would control migraine attacks (n/N = 161/198;81%), what the cause of migraine was (n/N = 57/75; 76%), their treatment expectations (n/N = 135/190; 71%), and that OTC pain medications may treat the attack but not prevent future attacks (n/N = 103/142; 73%). In contrast, 36% (n/N = 18/50) of participants who were told that 'migraine has no cause' reported that this was in line with what they previously thought (Table 5). There were 62 out of 130 (48%) participants who reported that being informed that overuse of OTC pain medications could make migraine attacks worse was consistent with what they previously thought (Table 5).
Table 5 Agreement between what participants previously thought and health-care providers’ explanationsAcute Migraine Treatment Prior to CGRP-Targeted Monoclonal AntibodyOnly eight (1.6%) participants reported never having had a pain prescription for acute treatment of migraine, either presently or in the past. Among the participants, 74% (n/N = 370/500) reported using triptans, 40% anti-nausea medications (n/N = 198/500), 39% oral CGRP antagonists (n/N = 194/500), and 15% reported using opioids (n/N = 73/500), either presently or in the past, for the acute treatment of migraine. Dihydroergotamine (n/N = 11/500; 2.2%) and lasmiditan (n/N = 4/500; 0.8%) were also reportedly used by some participants (Table 6). At the time of the survey, 82% (n/N = 409/500) reported that they were currently being prescribed at least one of these categories of pain medications for the acute treatment of migraine.
Table 6 Treatment for MigraineHalf (n/N = 252/500; 50%) of the participants reported also taking OTC medications to treat migraine. These drugs included non-steroidal anti-inflammatory drugs, acetaminophen (paracetamol), antihistamines, and decongestants.
Participants also reported using several behavioral and other non-pharmacologic methods for symptom relief during migraine attacks. These included avoiding bright lights (n/N = 435/500; 87%), rest (including sleep or relaxation; n/N = 426/500; 85%), avoiding loud noises (n/N = 394/500; 79%), and avoiding being with other people (n/N = 340/500; 68%), drinking water (n/N = 335/500; 67%), applying warm or cold compress (n/N = 287/500; 57%), eating (n/N = 104/500; 21%) (Table 6).
Preventive Migraine Treatment Prior to CGRP-Targeted Monoclonal AntibodyParticipants reported using mainly four different classes of medications to prevent migraine attacks; anticonvulsants (n/N = 307/500; 61%), antidepressants (n/N = 220/500; 44%), blood pressure-lowering medications (n/N = 215/500; 43%), and botulinum toxin A (n/N = 85/500; 17%) (Table 6). The preventive medications were not mutually exclusive, and participants may have been on 2 or more medications to prevent migraine throughout their journey. Among these participants, 15% (n/N = 22/145) of those who started blood pressure lowering medications, 23% (n/N = 30/128) of those on antidepressants, 18% (n/N = 44/239) of those on anticonvulsants, and 12% (n/N = 7/57) on botulinum toxin A reported taking these preventive treatments for two or more years. A sizeable proportion of subjects reported taking anticonvulsants (n/N = 109/239; 46%), blood pressure-lowering medications (n/N = 66/145; 46%), antidepressants (n/N = 46/128; 36%), or botulinum toxin A (n/N = 15/57; 26%) for 6 or fewer months before discontinuing them.
Participants who were taking antidepressants (n/N = 94/128; 73%) or blood pressure-lowering medications (n/N = 100/145; 69%) for the prevention of migraine reported that one of the reasons that they discontinued the treatment was because it was not effective (Table 6). Some participants taking antidepressants (n/N = 57/128; 45%) or blood pressure-lowering medications (n/N = 64/145; 44%) also reported side effects as a reason for discontinuation (Table 6). In contrast, more participants taking anticonvulsants reported side effects (n/N = 168/239; 70%) over treatment not being effective (n/N = 132/239; 55%) as reasons for discontinuation (Table 6). For botulinum toxin A, treatment not being effective (n/N = 27/57; 47%) was followed by expense (n/N = 18/57; 32%) and not covered by insurance (n/N = 10/57; 18%) in order of importance as reasons for discontinuation (Table 6). Reasons participants expressed for discontinuation of a drug class were not mutually exclusive, and they could indicate more than one reason for each drug class.
The participants also reported trying a variety of non-pharmacological methods to prevent their migraine attacks. The most common (> 50%) were changes in nutrition, adjusting fluid intake, and relaxation techniques (Table 6).
留言 (0)