
記住我



In this multi-cohort study, we employed a systematic approach to identify and validate a gene signature predictive of ICI response in NSCLC (Supplementary Figure S1). The study design encompassed retrospective discovery in two cohorts (PMBCR and BC) and prospective validation in an independent cohort (PBMCP). A total of 145 NSCLC patients were included in this study, with 59 in the PMBCR (WHTJ) cohort, 44 in the BC (RUMC) cohort, and 42 in the PBMCP (WHTJ) cohort. All patients received treatment with pembrolizumab, carboplatin, and pemetrexed. The median age was 62, 68, and 62 years in the PMBCR, BC, and PBMCP cohorts, respectively. The majority of patients were male (77.9% in PMBCR, 68.2% in BC, and 71.4% in PBMCP). The median progression-free survival (PFS) time was 190, 213, and 260.5 days, and the median follow-up time was 478, 520.5, and 535.5 days in the PMBCR, BC, and PBMCP cohorts, respectively. Smoking history was present in 55.9%, 95.5%, and 54.8% of patients in the PMBCR, BC, and PBMCP cohorts, respectively. Adenocarcinoma was the predominant pathological type across all cohorts. Most patients had stage IV disease (52.5% in PMBCR, 100% in BC, and 73.8% in PBMCP). The response rates were 47.5%, 22.7%, and 54.8% in the PMBCR, BC, and PBMCP cohorts, respectively (Supplementary Table 1).
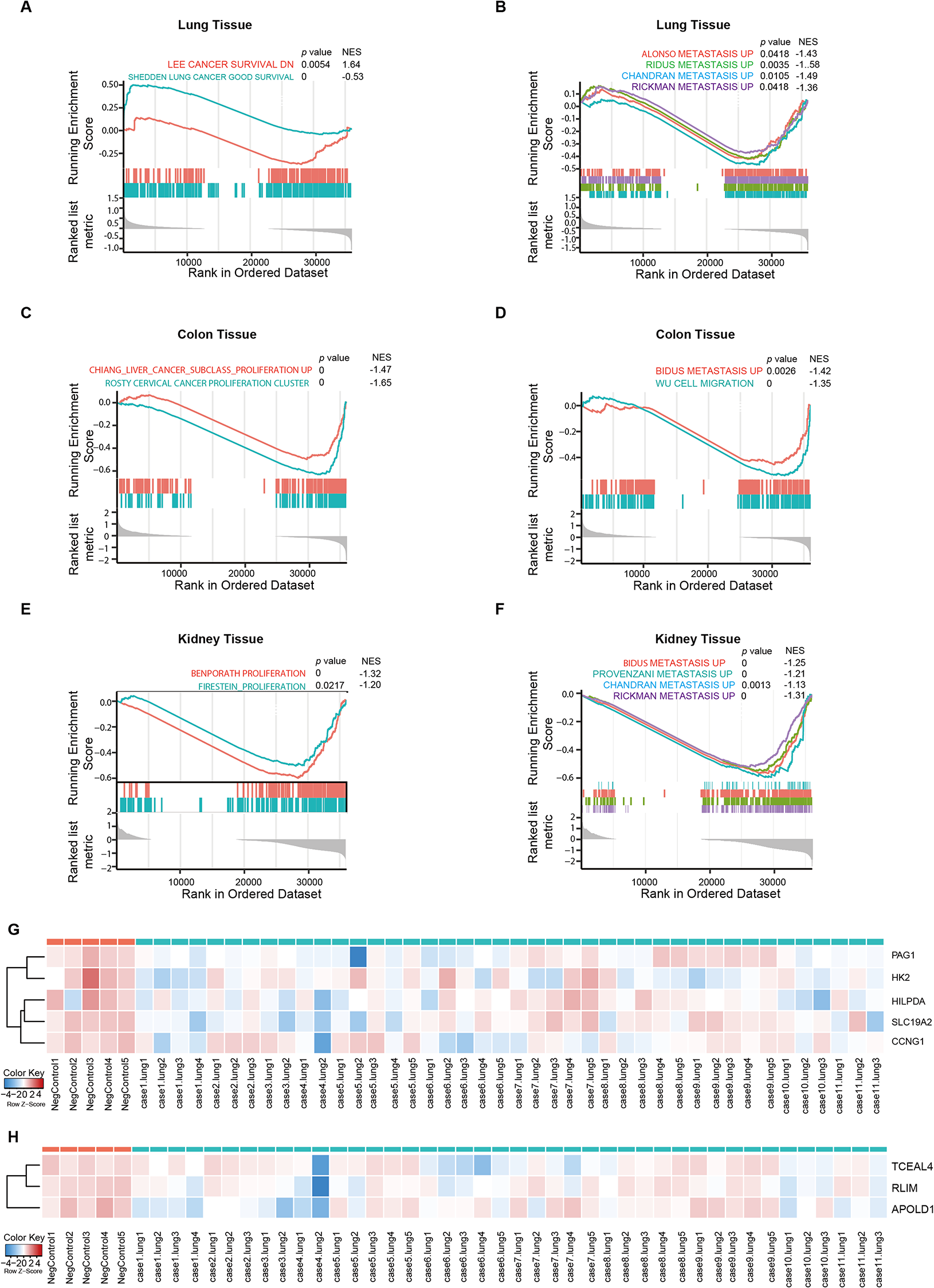
A novel 5-gene signature emerges as a robust predictor of ICI response in NSCLCThrough retrospective analysis of the PMBCR and BC cohorts, we identified 5 genes (UQCRB, NDUFA3, CDKN2D, FMNL1-DT, and APOL3) that contributed the most to differentiating responders from non-responders in both datasets (Supplementary Figure S2 and Supplementary Table 5). Based on these 5 genes, we established a 5-gene signature and calculated a meta-score for each patient. The distribution of meta-scores for responders and non-responders in the PMBCR and BC cohorts is shown in Fig. 1A and B, respectively.
Fig. 1
Transcriptomic Analysis Outcomes. A: Meta-score distribution of the 5-gene signature inresponders and non-responders of the PMBCR (WHTJ) training cohort. B: Meta-score distribution of the 5-genesignature in responders and non-responders of the BC(RUMC)validation cohort. C Meta-score distribution of the 5-gene signature in responders and non-responders of the PBMCP (WHTJ) prospective validation cohort. D: ROCcurve analysis demonstrating the predictive performance of the 5-gene signature in the PMBCR cohort (AUC=0.90,95% CI: 0.82-0.99). E: ROC curve analysis confirming the predictive value of the 5-gene signature in the BC(RUMC) validation cohort (AUC=0.89, 95% CI: 0.75-1.00). F: ROC curve analysis validating the predictive accuracyof the 5-gene signature in the prospective PBMCP cohort (AUC=0.89, 95% CI: 0.80-0.99)
Retrospective cohorts validate the strong predictive power of the 5-gene signatureTo validate the predictive performance of the 5-gene signature, we performed ROC curve analysis in both cohorts. The signature achieved an AUC of 0.90 (95% CI: 0.82–0.99) in the PMBCR cohort (Fig. 1D) and an AUC of 0.89 (95% CI: 0.75-1.00) in the BC cohort (Fig. 1E), demonstrating its robust ability to distinguish responders from non-responders.We further compared the 5-gene signature with other published gene markers (Supplementary Tables 2 & 3). The results showed that the 5-gene signature exhibited the highest stability and predictive accuracy among all the compared markers.
Examining the 5-gene signature in other cancer typesTo evaluate whether the 5-gene signature is specific to NSCLC, we analyzed its predictive performance in other cancer types. We collected Whole-blood RNA transcriptome sequencing data from Renal Cell Carcinoma patients and applied our 5-gene predictive model [6]. The results indicated a poor predictive performance, with an AUC of 0.42 (95% CI: 0.22 − 0.62), as shown in Supplementary Figure S3. Furthermore, we compared our 5-gene signature with predictive models used in melanoma and bladder cancer and found no overlap between the genes involved [7; 8]. This suggests that our 5-gene signature demonstrates strong specificity to NSCLC, and may not be broadly applicable across other cancer types.
Prospective validation solidifies the clinical utility of the 5-gene signature in guiding ICI treatment decisionsTo assess the clinical utility of the 5-gene signature, we conducted a prospective study in the PBMCP cohort. The meta-scores for responders and non-responders in the PBMCP cohort were calculated (Fig. 1C), and ROC curve analysis revealed an AUC of 0.89 (95% CI: 0.80–0.99) (Fig. 1F), confirming the signature’s predictive value in a prospective setting.
5-Gene signature serves as a reliable prognostic marker for survival outcomes in NSCLC patients receiving ICI therapyWe performed survival analysis based on the predicted response status determined by the 5-gene signature. In the PMBCR cohort, patients predicted as responders had significantly longer progression-free survival (PFS) compared to those predicted as non-responders (P < 0.001) (Fig. 2A). Similarly, in the BC cohort, both PFS and overall survival (OS) were significantly longer in the predicted responder group compared to the predicted non-responder group (P < 0.001) (Fig. 2C and D). The prospective PBMCP cohort also demonstrated significantly improved PFS in the predicted responder group (P < 0.001) (Fig. 2B), further validating the prognostic value of the 5-gene signature.
Fig. 2
Survival Analysis Demonstrating the Prognostic Value of the 5-Gene Signature. A: Kaplan-Meiercurves for progression-free survival (PFS) in the PMBCR cohort, revealing a significant survival benefit for patientspredicted as responders by the 5-gene signature compared to predicted non-responders (P < 0.001). B: Kaplan-Meier curves for PFS in the prospective PBMCP cohort, confirming the prognostic value of the 5-gene signature,with predicted responders exhibiting significantly longer PFS than predicted non-responders (P < 0.001). C: Kaplan-Meier curves for PFS in the BC cohort, demonstrating a significant survival advantage for predicted respondersover predicted non-responders based on the 5-gene signature (P < 0.001). D: Kaplan-Meier curves for overallsurvival (OS) in the BC cohort, showing a significant survival benefit for patients predicted as responders by the 5-gene signature compared to predicted non-responders (P < 0.001)
5-gene signature proves superior to clinical factors in predicting ICI response, highlighting its independent predictive valueTo investigate the relationship between clinical factors and the 5-gene signature, we performed multivariate logistic regression analysis. The results showed that the 5-gene signature was the most significant predictor of ICI response among all clinical factors (P < 0.001). Smoking history was also found to be significantly associated with ICI response (P < 0.05) (Supplementary Table 4).
留言 (0)