
記住我



A total of 78 cases who underwent lower gastrointestinal endoscopy were enrolled for this study: 17 healthy controls, 6 with conventional colorectal adenomas, 41 with Tis–T1 CRC, and 14 with T2–4 CRC. According to the AJCC and UICC TNM classifications, which are identical to the T classification, CRC patients were categorized into Tis–T1 and T2–4 stage groups. Patient characteristics are shown in Supplementary Tables S1-S3.
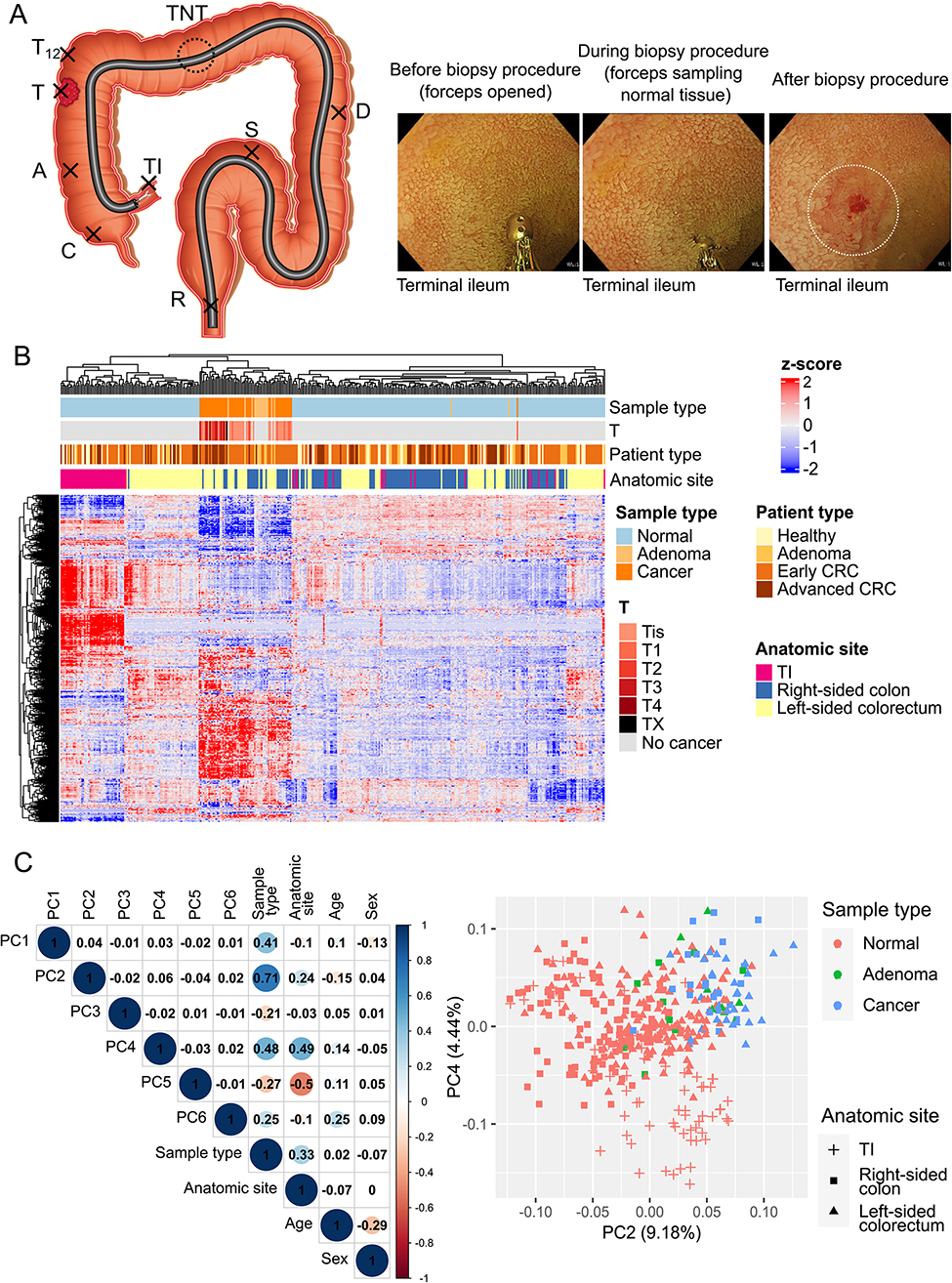
Biopsies were taken from various sections of the intestinal mucosa in the participants, such as the terminal ileum, right-sided colon, left-sided colorectum, CRC, adenoma, and adjacent normal mucosa 1–2 cm away from CRC or adenoma (Fig. 1A). We termed this procedure of collecting untargeted step biopsies of the intestinal mucosa from multiple locations in addition to biopsies from the targeted lesion(s) in the same individual “Endoscopic intestinal step biopsy.”
Fig. 1
Overview of the endoscopic intestinal step biopsy procedure. (A) Endoscopic biopsies of normal appearing mucosa of the terminal ileum and colorectum were performed for all individuals. Tumor samples and 1–2 cm of surrounding normal mucosa (T12) were also obtained where present. Biopsies from the transverse colon were only taken in a few cases because of the higher perforation risk than in other locations. The endoscopic images on the right show a biopsy procedure of the terminal ileum. The white dotted circle indicates the site after the biopsy. A, ascending colon; C, cecum; D, descending colon; R, rectum; S, sigmoid colon; T, tumor; TI, terminal ileum; TNT, transverse colon; T12, normal mucosa 1–2 cm away from the tumor. (B) Heatmap of all 388 samples using unsupervised clustering (top 2,500 genes). Colorectal cancer (CRC) and conventional adenoma cases belonged to the same cluster. (C) Principal component analysis (PCA) of 388 samples. PC2 strongly correlated with sample type, and PC4 with sample type and anatomic site (left panel). In PCA plots using PC2 and PC4, the terminal ileum samples are generally plotted separately from colorectal tumor samples. Colors (pink, green, blue) indicate “Sample type”, and shapes (+, ■, ▲) “Anatomic site”
A heatmap of all samples using the top 2,500 genes with high variability showed that CRC and conventional adenoma samples belonged to the same cluster (Fig. 1B). PCA revealed that PC2 and PC4 correlated strongly with sample type (CRC, conventional adenoma, or normal mucosa) and anatomic site (terminal ileum, right-sided colon, or left-sided colorectum) (Fig. 1C left). In contrast, age or sex did not exhibit any correlation with any axis. The terminal ileum tissues were distinct from both colonic tissue (tumor and non-tumor areas) when visualized using PC2 and PC4 (Fig. 1C right).
Gene expression in the intestinal mucosa of healthy individuals varies with the anatomic siteDEG analysis was performed to examine anatomic site-specific differences in gene expression in the intestine. Each anatomic site is shown in Fig. 2A. Unsupervised clustering of the top 500 variable genes showed that the terminal ileum, right-sided colon (cecum, ascending colon, transverse colon), and left-sided colorectum (descending colon, sigmoid colon, rectum) belonged to different clusters (Fig. 2B), indicating differences in embryological origin. The data obtained from PCA analysis did not indicate any discernible distinctions between the two hospitals (Supplementary Figure S1B). Age showed no correlation with the primary axis in the PCA analysis (Supplementary Figure S1C). However, considering the influence of age on transcriptome analysis data, we excluded DEGs that, based on regression analysis, appeared to have a potential association with age.
Fig. 2
Anatomic site-specific differences in the normal mucosa of healthy individuals. (A) Schema showing the anatomic sites of the terminal ileum (TI), right-sided colon, and left-sided colorectum. The superior mesenteric artery (SMA) dominates the terminal ileum and right-sided colon, embryologically derived from the midgut. The inferior mesenteric artery (IMA) dominates the left-sided colorectum, embryologically derived from the hindgut. (B) Heatmap for 61 normal mucosa samples from 17 healthy individuals using unsupervised clustering (top 500 genes). Note: separate clustering of terminal ileum (TI), right-sided colon, and left-sided colorectum. (C, D) Discrepancies in gene expression between the terminal ileum and the colorectum (C) and between the right-sided colon and left-sided colorectum (D) in healthy individuals. Volcano plots (left panels) show differences in gene expression in normal mucosa of different anatomic sites, with gene ontology (GO) enrichment analysis results in the right panels. An absolute value of log2 fold change (|log2FC|) > 1.5 and a false discovery rate (FDR) < 0.001 were used as cut-offs for expression variation genes
In the comparison between the colorectum and the terminal ileum, there were 877 DEGs up-regulated in the terminal ileum and 338 in the colorectum (Fig. 2C). In the terminal ileum, there was a significant enrichment of GO terms related to immune cell proliferation and activity. The expression of CCL25, a chemokine produced by the small intestinal epithelium and involved in lymphocyte homing, significantly differed between the terminal ileum and colorectum. Although not detected as a GO term, genes related to lipid transport, such as APOA, FABP6, and MTTP, were more highly expressed in the terminal ileum. In the colorectum, GO terms related to substance transport were enriched (Fig. 2C).
The comparison between the left-sided colorectum and the right-sided colon revealed an up-regulation of 210 DEGs in the left-sided colorectum and 122 DEGs in the right-sided colon (Fig. 2D). In the left-sided colorectum, GO terms associated with extracellular matrix organization and cell adhesion were highly enriched. The left-sided colorectum exhibited high expression levels of PRAC1 and PRAC2, which are specifically expressed in the human prostate and distal colorectum [15]. Homeobox genes, specifically HOXB13, HOXD11, HOXD12, and HOXD13 were upregulated in the left-sided colon. In the right-sided colon, GO terms related to response to xenobiotic stimulus and antimicrobial peptide were enriched (Fig. 2D). The REG (regenerating gene) family with various physiological activities in the intestinal tract, including antibacterial, anti-inflammatory, and antiapoptotic potential [16], exhibited significantly higher expression in the right-sided colon. Lists of DEGs are shown in Supplementary Tables S4 and S5.
Immune profiles of intestinal mucosa of healthy individuals differ by anatomic siteTo investigate how immune cells differ by anatomic site, we compared the immune profiles of the terminal ileum, right-sided colon, and left-sided colorectum of the normal mucosa of healthy individuals using CIBERSORTx. Unsupervised clustering showed that the terminal ileum samples were predominantly characterized by high B cell immunity (Fig. 3A). Among the immune cells, lymphocytes, followed by macrophages, accounted for a large proportion. M2 macrophages were found to be the prevailing type among macrophages in the terminal ileum, right-sided colon, and left-sided colorectum (Fig. 3A). In contrast, γδT cells, eosinophils, and neutrophils were observed in only a few samples.
Fig. 3
Differences in immune cell profiles of healthy individuals by anatomic site. (A) Bar plot (left panel) showing the results of unsupervised clustering of immune profiles of intestinal mucosa in healthy individuals calculated with CIBERSORTx. Bar plot (right panel) showing the mean values for the terminal ileum (TI), right-sided colon (Right), and left-sided colorectum (Left). (B, C) Depending on the anatomic site, immune cells were found in differing amounts (Mann-Whitney U test). The Y-axis indicates absolute abundance. TI, terminal ileum; Right, right-sided colon; Left, left-sided colorectum
The terminal ileum exhibited significantly more immune cells than the colorectum (P = 0.0039, Mann-Whitney U test) (Fig. 3A, Supplementary Figure S2A), with more B cells than the colorectum and more CD8+ T cells, follicular helper T cells, regulatory T cells, and M0 macrophages. There were fewer resting dendritic cells and more active ones (Fig. 3B). The abundance of B cells, active dendritic cells, and follicular helper T cells in the terminal ileum presumably reflects abundant Peyer’s patches and active antigen presentation. Data on the abundance of cell types are provided in Supplementary Figure S2B.
A site-specific comparison showed that the left-sided colorectum displayed a significantly elevated presence of immune cells compared to the right-sided colon (P = 0.022, Mann-Whitney U test) (Fig. 3C, Supplementary Figure S3A). The left-sided colorectum exhibited a higher presence of plasma cells, CD8+ T cells, resting memory CD4+ T cells, resting NK cells, and macrophage M2. The data regarding the abundance of cell types is presented in Supplementary Figure S3B. We also examined the disparity in gene expression between rectal and colonic tissue in healthy individuals. The rectum exhibited a higher count of immune cells, denoted as Absolute score, compared to the colon (Supplementary Figure S4A). In the rectum, B cell memory, T cell CD4 memory resting, macrophage M2, and resting mast cells were more prevalent, whereas activated T cell CD4 memory was more prevalent in the colon (Supplementary Figure S4B).
Normal-appearing intestinal mucosa of CRC patients exhibits different gene expression from healthy individualsA DEG analysis was conducted in order to examine potential differences in gene expression between the normal intestinal mucosa of CRC patients and healthy individuals. Due to the significant variation in gene expression across different anatomic sites in the intestinal tract, a differential expression analysis was performed for each site. The DEG analysis did not factor in the distance from the CRC, as PCA did not establish a distinction between normal colonic mucosa close to or distant from the CRC (Supplementary FigureS5). In order to take account of the age and sex disparities among healthy individuals, Tis–T1 CRC patients, and T2–4 CRC patients, regression analysis was conducted to eliminate any DEGs that could be attributed to age or sex. When comparing T2–4 CRC patients with healthy individuals, more DEGs were observed across all anatomical sites, in contrast to the comparison between Tis–T1 CRC patients and healthy individuals. In the left-sided colorectum, right-sided colon, and terminal ileum, 259, 316, and 71 DEGs were detected in T2–4 CRC patients, respectively (Fig. 4A and B). Notably, many DEGs were also identified in the terminal ileum of T2–4 CRC patients, even when the terminal ileum was distant from the CRC anatomically. A detailed compilation of the DEGs is presented in Supplementary Tables S6-S10.
Fig. 4
Differences in gene expression between normal mucosa of CRC patients and healthy individuals. (A, B) Volcano plots show gene expression differences between normal mucosa of CRC patients and healthy controls (HC). The comparison for T2–4 CRC patients is provided in A, and for Tis–T1 CRC patients (Tis and T1), in B. Left-sided colorectum (Left), right-sided colon (Right), and terminal ileum (TI) are shown in order from left to right. After conducting a multiple regression analysis that accounted for age and sex, the differential expression analysis omitted genes suspected of introducing confounding variables. These genes are visually represented as gray dots in the figure. (C) Results of gene ontology (GO) enrichment analysis of expression variation genes in normal mucosa of T2–4 CRC patients and normal mucosa of healthy controls. FDR, false discovery rate; Left, left-sided colorectum; logFC, log2 fold change; Right, right-sided colon; TI, terminal ileum. (D) Volcano plot showing gene expression differences between two groups of cases: those with lymph node metastasis (n = 11) and those without (n = 11). The thresholds were set at log2FC absolute value > 0.8 and FDR < 0.01. Regression analysis was performed to examine the correlation with age, sex, and T stage for each DEG, and genes correlated with them were excluded from the DEG
GO analysis was performed on the DEGs of T2–4 CRC patients’ normal mucosa compared to healthy individuals’ normal mucosa (Fig. 4C). The down-regulation of transcription and translation-related GO terms, which indicate the involvement of ribosome-related genes (e.g., RPS18, RPS17, RPL24), was observed in patients with T2–4 CRC across all anatomic sites.
Furthermore, we analyzed the disparities in gene expression in the terminal ileum between two groups of cases: those with lymph node metastasis (n = 11) and those without (n = 11), among T1 to T4 cases (total of 22 cases) (Fig. 4D). In cases with lymph node metastasis, the terminal ileum exhibited high expression levels of genes encoding glycosyltransferases involved in the metabolism and excretion of both endogenous and exogenous toxic compounds (e.g., UGT2B17, UGT2B15). On the contrary, the expression of immune-related genes, specifically CXCL3 and CD59, was decreased in these patients.
Differences in mutations between Tis–T1 and T2–4 CRCs on whole-exome sequencing (WES) analysisTumor samples from 47 CRC patients were subjected to WES, with 23 patients classified as having Tis–T1 CRCs, 24 with T2–4 CRCs, and 7 with concomitant conventional adenomas. Note: three Tis–T1 CRC patients and ten T2–4 CRC patients were not included in this RNA-seq analysis.
Figure 5A illustrates an oncoplot of somatic mutations of known driver genes in CRCs. Somatic mutations of TP53 were detected in T2–4 CRCs more frequently than in Tis–T1 CRCs (P = 0.0010, Fisher’s exact test). Interestingly, there was a mutual exclusivity observed between somatic mutations in TP53 and KRAS in all CRCs (P = 0.020, Fisher’s exact test), as well as in CRCs at the Tis–T1 stage (P = 0.021, Fisher’s exact test). This is likely since the study specifically concentrated on early-stage CRC. The typical progression of abnormalities in CRC involves the sequential accumulation of APC, KRAS, and TP53 mutation [14, 17]. The presence of TP53 mutations in colorectal tumors with APC abnormalities may obviate the need for KRAS mutations in early-stage CRC [18]. BRAF mutations were observed in only two cases [19]. In addition, three cases were found to have a hyper-mutated phenotype.
Fig. 5
Mutations revealed by whole-exome analysis and their association with the transcriptome. (A) Oncoplot of mutations revealed by whole-exome sequencing analysis of Tis–T1 and T2–4 CRC and adenomas. Note: the inclusion of somatic mutations in known driver genes. The upper panel shows the number of somatic mutations. The most advanced lesion is classified as Patient type. (B) Heatmap for normal mucosa samples of 55 CRC patients using unsupervised clustering (top 1,000 genes). No obvious associations were identified between major CRC mutation (i.e., APC, TP53, and KRAS) and gene expression. (C) Volcano plots show differences in gene expression between normal mucosa of CRC patients with KRAS mutation and that of CRC patients with KRAS wild-type. The analysis of the left-sided colorectum is shown in the left panel, the right-sided colon in the center, and terminal ileum on the right. After conducting a multiple regression analysis that accounted for age and sex, the differential expression analysis omitted genes suspected of introducing confounding variables. These genes are visually represented as gray dots in the figure. logFC, log2 fold change; NA, not available; TI, terminal ileum
The inclusion of CRCs through the serrated pathway was restricted in this biopsy study due to the potential hindrance of pathological diagnosis by biopsies in cases of CRCs displaying flat appearance through the serrated pathway. APC mutations were identified in 21 out of 25 CRCs, suggesting that these tumors likely progressed through the adenoma-carcinoma sequence, a well-established conventional pathway. In the subset of Tis (advanced adenoma)–T1 CRC and adenoma cases (Fig. 5A), APC mutations were observed in 21 of 30 tumors, further supporting their classification as conventional tumors. A histological analysis of the endoscopically resected tumors was conducted for the remaining nine cases without APC mutations to explore the potential involvement of alternative pathways, such as the serrated pathway. These cases also revealed the presence of conventional adenoma components. Thus, the focus of the present study is on tumors that follow the conventional adenoma-carcinoma progression pathway.
Examination of the relationship between tumor mutations and gene expressionAn assessment was performed to examine the relationship between tumor mutations and gene expression in normal mucosa. The heatmap generated using normal mucosa samples from CRC patients, focusing on the top 1,000 variable genes, revealed no discernible correlation between major three CRC mutations (i.e., APC, TP53, and KRAS) and gene expression (Fig. 5B).
Subsequently, DEG analysis was conducted in order to evaluate potential disparities between normal mucosa of CRC patients with significant mutations and that of CRC patients without mutations. Due to the high prevalence of APC mutations in CRC patients and the need to consider genetic abnormalities such as LOH (loss of heterozygosity) in the case of the TP53 gene, DEG analysis was restricted to the presence or absence of KRAS gene mutations. DEG analysis was conducted for each anatomic site, comparing the normal appearing mucosa of CRC patients with KRAS mutations and the KRAS wild-type. The study revealed the presence of 404 DEGs in the left-sided colorectum, 71 DEGs in the right-sided colon, and no DEGs in the terminal ileum (Fig. 5C). The Consensus Molecular Subtypes (CMS) framework is being developed as a tool for classifying CRC [20]. CMS1, characterized by hypermutation, microsatellite instability, and pronounced immune activation, is frequently associated with BRAF mutations, whereas CMS3, distinguished by epithelial features and marked metabolic dysregulation, often harbors KRAS mutations. The findings of this study indicate that the gene expression profiles of normal tissues vary depending on the presence or absence of KRAS mutations, suggesting that distinct predisposition states might exist prior to tumor development, as classified by the CMS framework.
留言 (0)