
記住我
The adaptation of the HIRAID® framework for residential aged care will be achieved using a real-time Delphi. This Delphi technique will allow experts to view panel responses and feedback in real-time and change their own responses within a set timeframe [14, 15].
ParticipantsThe panel will purposively recruit experts from two populations:
Academic experts in the fields of aged care, nursing pedagogy, education, and training, including researchers involved in the development and implementation of the original HIRAID® framework in the ED context
Clinical and management experts in aged care, including registered nurses, nurse educators, and facility managers, from six residential aged care organisations
Given the focused aim of the Delphi and the homogeneity of the expert population, this study will recruit 12 participants to the panel.
Data collectionPrior to commencing the Delphi, a semi-structured facilitated discussion with HIRAID® and aged care experts will be conducted to identify key questions and items for the survey. The session will occur in tandem with an onsite demonstration of HIRAID® at an ED framework where the framework is active to enable aged care experts to understand how HIRAID® operates in established practice. The discussion session will include members of the expert panel for the Delphi study as well as non-panel members and stakeholders. No members of the panel will be individually identified during the session.
The Delphi will combine the functionality of real-time consensus with iterative survey rounds and will be hosted on Calibrum (Calibrum International, USA, calibrum.com). The first round of survey items will be developed using feedback generated from the facilitated discussion. The survey will contain a combination of open-ended questions and Likert scale items. The level of consensus for each item will be calculated by the proportion of experts who gave a rating of the same valency, that is, if more than 80% of experts responded ‘somewhat agree’, ‘agree’, or ‘strongly agree’ on a 7-point Likert scale, an agreement consensus is reached for that item. The same 80% threshold applies for disagree responses to reject an item.
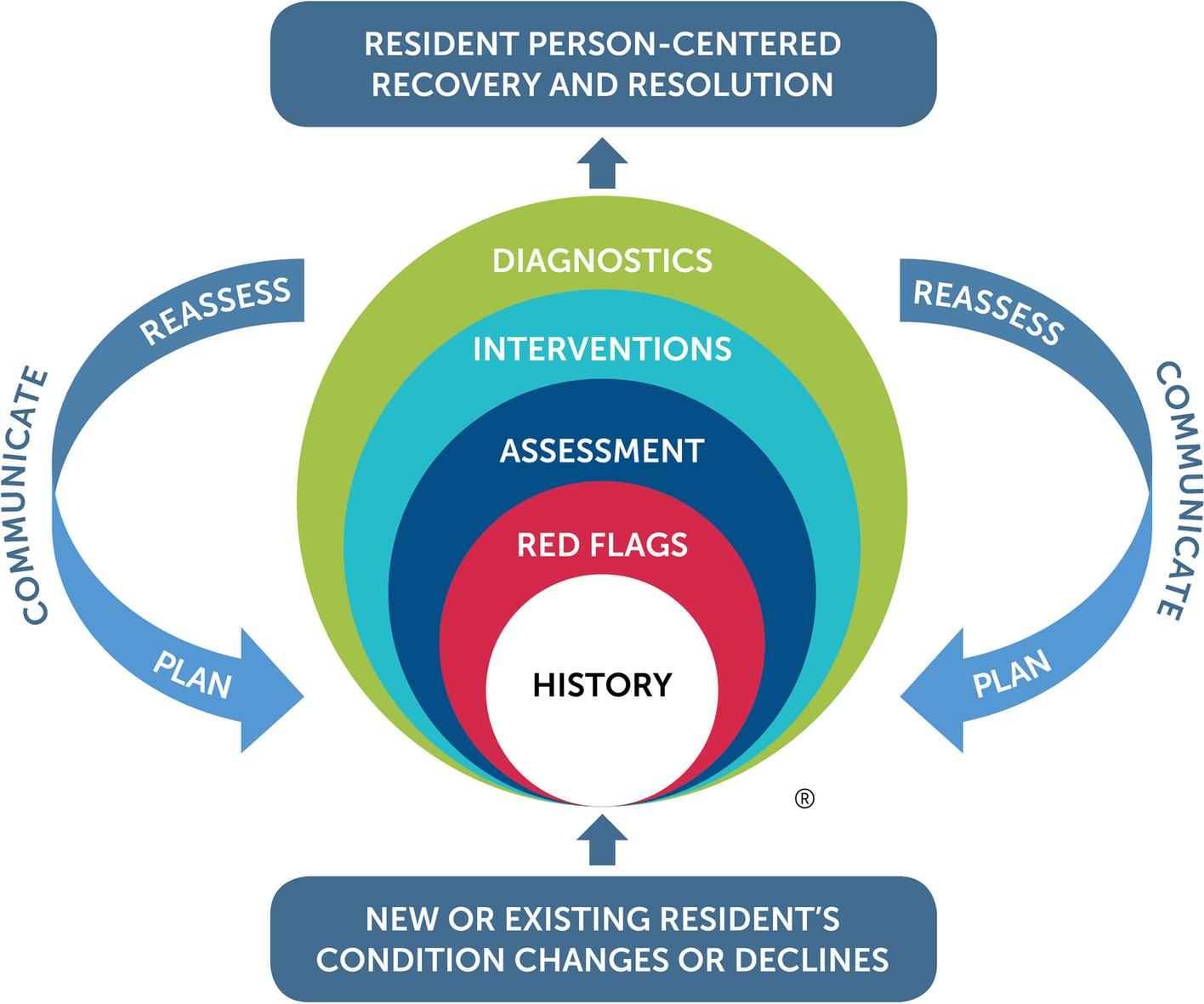
The survey will comprise nine sections, including a short demographic questionnaire and then one for each of the eight elements of the original HIRAID® framework (Fig. 1). During each survey round, panel members will be able to review anonymised responses in real-time. This information will include the distribution of panel members’ votes, comments, and responses to open-ended questions. Each round of the survey will be distributed to panel members via email and open for 2 weeks. Experts will be able to begin the survey and revise their responses at any time during this period.
Data analysis and outcomesSummative responses from round 1 will be provided to panel members and used to inform the items in the subsequent round. Data will be exported from Calibrum into IBM SPSS Statistics V28 (IBM Corp., Armonk, NY, USA) for descriptive analysis [16]. Qualitative data will be exported to NVivo 14 (Lumivero, Denver, CO, USA) for content analysis, where responses will be coded by two members of the research team [17]. Qualitative outcomes will inform the questions in the subsequent survey round, including how items that do not reach consensus are modified and whether new items are added. Only items that reach 80% consensus with a positive valency will be included in the HIRAID® Aged Care framework. Items that do not reach consensus after two rounds will be rejected. The Delphi will terminate once no items remain for review. The final HIRAID® Aged Care framework and implementation package will be co-designed by the research team and aged care partners based on the outcomes of the Delphi.
Stage 2: Implementation and evaluation of HIRAID® Aged CareStudy designIn stage 2, the HIRAID® Aged Care framework will be implemented using a modified SW-cRCT design, where each cluster undergoes 6 months of baseline observations, followed by a 6-month intervention transition period and then 12 months of post-intervention data collection [18]. A SW-cRCT design was selected as it is advantageous for implementing and evaluating health service interventions where participants belong to pre-determined groups (i.e. homes) and cannot be randomly assigned. Furthermore, the design has the ethical benefit of allowing all participants to receive the intervention, ensuring that potentially beneficial treatments are not withheld from control participants. The design also provides important logistical advantages, including optimising implementation and data collection resources, and accommodating for temporal issues, such as delays in implementation [19]. HIRAID® Aged Care implementation will be evaluated using a type 1 effective-implementation hybrid design to simultaneously assess the effectiveness of the implementation strategies in supporting HIRAID® Aged Care uptake, sustainability and impact [20].
The sequence of treatments will be identical for all clusters and will comprise three consecutive phases (Fig. 2): a baseline phase where usual care is provided (B-BD), an intervention transition phase when the intervention is provided (I-T), and a post-intervention data collection phase (I-D). The commencement of the sequence at each cluster will be staggered at 3-month intervals. Each cluster will be randomly allocated to a sequence by the study statistician. Each sequence is expected to be completed within 24 months and the whole trial within 33 months.
Fig. 2
The modified stepped-wedge cluster randomised controlled trial design for the implementation of HIRAID® Aged Care across four clusters. Each sequence comprises a 6-month baseline control condition, a 6-month intervention transition period, and a 12-month intervention exposure condition
The interventionHIRAID® Aged Care is an eight-element framework (History including Infection risk, Red Flags, Assessment, Interventions, Diagnostics, reassessment, communication, plan) that will provide RNs with an evidence-based, systematised approach to completing and documenting point-of-care assessments and decisions in residential aged care. The delivery of the intervention will be multi-pronged and supported by strategies informed by behaviour change and implementation science, including the assessment of enablers and barriers to HIRAID® Aged Care implementation, a co-designed and scaffolded education program, and integration of HIRAID® Aged Care into homes’ documentation systems. The evaluation of the intervention will test six primary hypotheses listed in Table 1.
Table 1 List of the six primary hypotheses to be tested through the implementation and evaluation of HIRAID® Aged CareStudy settingThe study will be conducted in 23 homes located across Sydney, Australia. To be eligible, all homes must be located within the greater Sydney area, have permanently employed RNs, and must belong to one of six organisations: Southern Cross Care, Hardi Aged Care, United Protestant Association of NSW Ltd., Opal Health Care, Minchinbury Manor, and Gallipoli Home. Participating homes were selected by executives from each organisation based on their suitability and readiness to adopt the intervention. Selected homes vary in size and total bed numbers (ranging from 25 to 149, Table 2) and include a mix of not-for-profit, for-profit, faith-based, and non-faith-based organisations.
Table 2 Profiles of the six participating aged care organisations, including the number of participating homes, number of homes with > 100 beds, total beds across homes, and approximate number of RNs employed across all homesParticipants and eligibility criteria Nursing staffAll RNs, ENs, and NPs employed by partnering aged care organisations will be enrolled to complete the HIRAID® Aged Care training to implement the framework in routine practice. Furthermore, nursing staff will also be invited to participate in the evaluation of the intervention (i.e. surveys, interviews to assess the effectiveness of HIRAID® Aged Care against the outcomes of interest and the success of the implementation process). To be eligible, nursing staff must be employed by a participating aged care organisation during the study period and have received the HIRAID® Aged Care training. Sampling will be stratified based on the bed numbers of each home.
Medical staffMedical and allied healthcare staff employed or contracted by partnering organisations will be eligible to participate in the evaluation of the intervention with no exclusions. Participation will include the completion of surveys and interviews to understand how the intervention has changed their working relationship and communication with aged care nursing staff.
ResidentsAll persons who reside or come to reside in participating homes during the study period will be included for the evaluation of the intervention. A waiver of consent has been approved for the collection of de-identified resident data, which will include medical records, care plans, charts, progress notes, and all associated documentation pertaining to clinical deterioration, incidents, and hospital transfers. Residents will also be able to participate in surveys and interviews to see if the intervention has changed their satisfaction with care.
Family of residentsFamily members and/or guardians of residents will be invited to participate in the evaluation of the intervention via surveys and interviews, as described above. To be eligible, they must be over 18 years of age and visit the resident at least once during the study period.
Research implementation officersAll research implementation officers employed by the study will be included to evaluate implementation fidelity, as they will be responsible for the implementation of HIRAID® Aged Care.
RandomisationA restricted randomisation process will be employed to allocate participating homes into four clusters. The allocation will balance for home size and ensure an even distribution of bed numbers across clusters. A geographical restriction will also be applied to minimise large distances between homes within the same cluster for practicality. Each cluster will then be randomly allocated to one of four starting dates. Randomisation will be completed by the study statistician using computer-generated numbers. No participating homes will be able to influence their allocation before the randomisation occurs, meaning that the allocation sequence will be concealed until participating homes are assigned. To minimise the risk of bias, there will be no changes to clusters after allocation.
BlindingGiven the nature of the intervention, it is impractical to blind investigators and staff delivering the intervention to the cluster allocation after it has been randomly assigned. However, the researchers recording and evaluating outcomes for nurse-associated clinical deterioration events, inappropriate hospital transfers, and nursing documentation will be blinded to the cluster and intervention sequencing. Specific participants population who are not directly involved in the delivering or receiving the intervention (i.e. residents, family of residents) will also be blinded to their cluster allocation.
Study plan Tailoring the implementation strategiesSite-specific implementation strategies will be guided by the integrated Promoting Action on Research Implementation in Health Services (i-PARIHS) framework and behaviour change wheel (BCW) [21, 22]. Behavioural diagnostics will be undertaken during baseline data collection to identify enablers and barriers to implementation. This will be measured using the Practice Environment Scale of the Nursing Work Index (PES-NWI) [23], which will assess nurses’ perception of the practice environment and identify organisational and external factors that influence nurses’ ability to practice skilfully and deliver high-quality care. Nursing staff will also complete a short survey that will be co-designed using the i-PARIHS Framework [21, 24] to identify local enablers and barriers to implementing HIRAID® Aged Care.
The outcomes from both instruments will be reviewed to identify the primary facilitators and barriers to the implementation of HIRAID® Aged Care and will inform the development, adaptation, and preparation of site-specific implementation strategies. The BCW will be used to map facilitators and barriers to specific intervention functions and techniques for sustained behaviour change. The final implementation strategy will be refined using mechanisms from the behaviour change techniques taxonomy and the APEASE criteria [22]. This approach has previously been used to inform the implementation strategies for HIRAID® in the ED [25].
Education and training of nursing staffAll nursing staff will receive pedagogically informed education regarding the theory and practice of HIRAID® Aged Care. The education approach will be co-designed with experts from the six participating organisations and will be grounded in principles of constructive alignment [26,27,28], backwards design [29], and scaffolded learning [30]. HIRAID® Aged Care training will first be delivered to all NPs and senior RNs employed at each site, and then in a separate session, to the remainder of the RN and EN workforce. In addition to HIRAID® Aged Care training, NPs and senior RNs will also complete HIRAID® Aged Care instructor training. This component will prepare staff to independently deliver HIRAID® Aged Care training to ensure sustainability. Completion of HIRAID® Aged Care training will be mandatory for all incoming nursing staff and having an instructor base will enable integration into orientation and onboarding programs.
Integration of framework into documentation systemsHIRAID® Aged Care documentation templates will be integrated into local electronic and paper documentation systems. A standard documentation template will be created for HIRAID® Aged Care that contains fields and prompts for each of its elements. Integration of documentation templates will be adapted based on local factors, such as use of electronic or paper-based documentation, and in the case of electronic documentation, the product(s) used (e.g. AutumnCare [31], ManAd [32]), automation capabilities, and capacity to communicate with existing assessment tools. The documentation templates will be tailored to maximise the efficiency of documentation of assessments whilst reducing duplication, administrative burdens, and redundancies for nurses.
Supporting materialsSeveral strategies tailored to local facilitators and barriers will be deployed to support implementation. These include co-designed educational materials that provide easy access to learning and support. Environmental cues such as posters and reference cards will act as immediate reminders of the structure of HIRAID® Aged Care. Uptake of HIRAID® Aged Care will also be positively reinforced by implementation officers and nurse champions seconded from the existing nursing workforce. Research implementation officers will perform fortnightly audits of nursing documentation to ascertain uptake, maintain a record of implementation strategies executed within their allocated sites, and regularly correspond with the research team to provide updates, identify teaching opportunities, and address implementation issues.
The general phases of the study are summarised in Fig. 3.
Fig. 3
Overall process for the implementation and outcome measurement of the HIRAID® Aged Care intervention
Outcomes Nurse-associated clinical deteriorationThe outcome will measure the mean difference in the rate of nurse-associated resident clinical deterioration events between baseline and post-intervention. Clinical deterioration is broadly described as the worsening of an individual’s clinical state, putting them at increased risk of greater morbidity and mortality, with nurse-associated clinical deterioration pertaining to deterioration events that are directly influenced by a nurse’s involvement, such as their capacity to recognise, react, or respond to events [33,34,35]. In this study, a clinical deterioration event will be defined by the activation of local clinical deterioration pathways, which will be identified through the review of residents’ medical records and progress notes. All participating homes maintain policies and systems for identifying and responding to clinical deterioration. These pathways typically require the initiation of ongoing vital sign monitoring, escalation for medical officer review, progress note documentation and, if required, hospital transfer.
For all identified clinical deterioration events, the associated medical records, clinical data, forms, and documents will be reviewed by a panel of experienced aged care clinicians to identify the prime causal factors. The Human Factors Classification Framework [36] for patient safety will be used to assess the degree of nurse involvement as a causal factor for the event. The framework distinguishes several factors that may have directly led to or increased the likelihood of a clinical deterioration event, including those relating to staff action. All reviewers will complete an initial review of 10 duplicate records to ensure consistent scoring. Inter-rater reliability will be examined for all items using Cohen’s kappa. Major discrepancies in scores between reviewers will be re-evaluated and resolved by an additional independent reviewer. All reviewers will be blinded to whether the record was created during baseline or post-intervention and to the identity of the nurses. This framework has been previously described to evaluate the effect of HIRAID® on nurse-associated clinical deterioration in the ED [11].
Inappropriate hospital transferThis outcome will measure the mean difference in the rate of inappropriate transfer to the hospital or ED between baseline and post-intervention. The rate and outcomes of ED transfer will be extracted from data that is routinely collected and reported as part of residential aged care services. To identify the proportion of inappropriate transfers, a panel of experienced aged care clinicians will review data from the ED medical charts, transfer and discharge forms of discharged residents. The inappropriateness of the transfer will be assessed against an adapted version of Codde et al.’s (2010) criteria that is co-designed with aged care partners to take into consideration local policies and procedures [37, 38].
Aged care quality indicatorsThis outcome will measure the mean difference in the performance on quality indicators reported between baseline and post-intervention [39]. The National Aged Care Mandatory Quality Indicators Program (QI Program) defines 11 quality indicators relevant to resident care and wellbeing, which aged care organisations are required to report for each home quarterly. Performance on each indicator is measured as the percentage of residents that meet a specified criteria for that indicator (Table 3).
Table 3 The 11 quality indicators reported to the National Aged Care Mandatory Quality Indicators Program for homes every 3 months Resident and family carer satisfactionResident and family carer satisfaction with care and perception of the person-centredness of care will be compared at baseline and post-intervention. Satisfaction with care will be determined by mean scores on Schmidt’s Perceptions of Nursing Care Survey (SPNCS), which comprises 15 items on a 5-point Likert scale [40]. Perception of person centredness of care will be determined by mean scores on the Person-Centred Practice Inventory-Care (PCPI-C) [41].
Staff satisfaction with communicationSatisfaction with communication amongst nursing and medical staff will be compared at baseline and post-intervention. Satisfaction will be measured using a previously validated instrument that asks staff to rate 8 items on a 11-point Likert scale, 5 yes/no questions, and one free-response question [42]. The instrument assesses overall satisfaction with nurse communication and the quality of information received during handover.
Nursing staff capabilityNursing staff capability will be compared at baseline and post-intervention across three self-reported domains: self-efficacy, anxiety, and perception of person-centredness of care provided. Nurse self-efficacy will be measured using the Self-Efficacy in Clinical Performance Scale, where nurses rate their level of confidence for 14 items on an 11-point Likert scale [13]. Anxiety will be measured using the State-Trait Anxiety Inventory, where nurses rate the relatability of 20 statements on a 4-point Likert scale [43]. Finally, nurses’ perception of the person-centredness of care will be measured using the Person-Centred Practice Inventory-Staff (PCPI-S), which consists of 59 items for which nurses indicate their agreement on a 5-point Likert scale [44, 45].
Quality and quantity of nursing documentationThe quality (accuracy) and quantity (completeness) of nursing documentation will be assessed by two experienced nurse clinicians through the review of resident electronic and paper medical records using the modified D-Catch tool [12, 46]. Average ranks and distribution of ranks in documentation quantity and quality will be compared at baseline and post-intervention. Inter-rater reliability will be examined for all items using Cohen’s kappa, and major discrepancies in scores between reviewers will be re-evaluated and resolved by an additional independent reviewer.
Implementation fidelityDifferences in the delivery of the intervention between sites may impact the outcomes of the intervention at those sites [47]. Implementation will be assessed throughout the intervention transition and post-intervention periods by research implementation officers, who will score implementation strategies against two criteria: whether the intervention was implemented (from 0 = not implemented, to 2 = fully implemented) and how much the intervention deviated from the plan (from 1 = just as planned to 4 = many changes). Implementation fidelity scores will be considered when evaluating the effect of the HIRAID® Aged Care intervention across different sites.
Finally, nurses’ overall perceptions and experiences of HIRAID® Aged Care and its implementation will be collected through a formal feedback survey and online interviews. The survey will comprise a selection of Likert scale and free responses questions where nurses rate the utility and useability of HIRAID® Aged Care from an end-user perspective. Nurses who complete the survey will also be invited to participate in a semi-structured interview with a member of the research team. Outcomes from the survey and interviews will inform improvements to both the HIRAID® Aged Care framework and future implementation strategies.
All outcome measures are summarised in Table 4.
Table 4 Summary of HIRAID® Aged Care outcome measures and associated measurement instruments, data collection methods, and measurement timepoints (by 3-month intervals)Sample sizeSample sizes were calculated for each of the six hypotheses (Table 5) and assumed an intracluster correlation coefficient of 3%, 5% significance (two-tailed) and 80% power. Baseline and attrition values are estimates based on existing literature scans and values derived from participating aged care organisations as well as similar projects previously completed by the research team.
Table 5 Sample size calculations for six hypotheses showing the target total and per arm sample sizesData collection Resident health records and nursing documentationResident medical records, charts, progress notes, and associated documentation will be extracted from each home’s electronic databases monthly. Quality indicator data are routinely collected by aged care organisations to meet mandatory reporting requirements and will also be obtained quarterly from databases. If a site uses mixed documentation methods, both electronic and paper documents will be obtained and paper documents will be scanned and stored electronically.
Resident and family-of-resident surveysResidents will be approached and invited to complete the surveys onsite. Residents who have cognitive or communication issues will be invited following consultation with their guardians and/or treating clinician and may have a family member complete the survey on their behalf. Family-of-residents will be invited to complete the surveys during their visitations and will be given the option to complete the survey on paper, online, or over-the-phone. Participants opting to complete the survey online will receive a link to the REDCap™ survey via their provided email address. Gift vouchers (AU$10) will be offered to both residents and family-of-residents to incentivise participation. Baseline surveys will be administered three months prior to commencement of the intervention-transition period, and post-intervention surveys will be administered three months after the intervention-transition period is completed.
Medical and nursing staff surveysAll nursing and medical staff surveys will be hosted on REDCap™ and will be distributed electronically to staff emails via the office of the aged care organisation. Baseline surveys for both medical and nursing staff will be distributed 3 months prior to commencement of the intervention. Post-intervention surveys will be distributed three months after the intervention-transition period has concluded. Gift vouchers (AU$10–$20) will be offered to nursing and medical staff to incentivise survey participation.
Nursing interviewsAll nursing staff completing the post-intervention survey will be invited to participate in an interview, which will supplement data collected from the post-intervention feedback surveys. Interviews will follow a semi-structured interview guide and may be completed in-person, over the phone, or via teleconferencing software. The interview will be audio recorded and then transcribed verbatim for data analysis. Interviews participants will be offered an AU$20 gift voucher.
Implementation auditsImplementation fidelity data will be collected by research implementation officers through regular audits during the intervention transition and post-intervention periods. Data will be entered for each site into standardised implementation logs and a fidelity scoring framework hosted on REDCap™.
Statistical methods Quantitative dataData will be analysed using SPSS V28[16] and by intention-to-treat. The demographic and clinical characteristics of residents will be summarised descriptively using mean and standard deviation for numeric data and frequency and percentage for categorical data. Bivariate analyses between all study and the outcome variables will be applied using Student T-test or ANOVA for continuous variables and chi-squared test or Fisher exact test for categorical variables. Logistic regression analyses will be employed for investigating the effect of the intervention on the outcome measures with adjustment for potential confounding variables identified in the bivariate analyses, such as seasonal variations, cluster start date, and the introduction of independent practice initiatives running in parallel.
Qualitative dataQualitative data will be analysed thematically using an inductive approach by two independent researchers. This approach was selected as the qualitative aspect of the study is exploratory and will serve to provide more information about different staff, resident, and family experiences of care and how they change throughout the intervention. Responses will be coded line by line, and content analysis will be used to develop the thematic organisation of responses [48]. The software program NVivo 14 [17] will be used to facilitate coding of all qualitative data.
Process evaluationFor behavioural diagnostic data, quantitative items will be determined to be facilitators if they are a positive valence and reach greater or equal to 70% agreement [49, 50]. The same threshold applies to barriers and negative valence items. A sentiment analysis will be performed on qualitative data to identify additional facilitators or barriers based on positively or negatively worded statements [51, 52]. Sub-analyses will be conducted to identify specific barriers or facilitators by location to tailor implementation. Post-intervention measures of implementation fidelity and intervention feedback will be collated and analysed for each site. Categorical fidelity measures will be incorporated and adjusted for within the logistic regression analyses.
Economic evaluationAn economic evaluation will be conducted to measure potential reductions in treatment costs associated with fewer adverse resident events and hospitalisations associated with the intervention. Discrete event simulation extrapolation modelling will be performed to estimate local and other system-wide implications of the implementation of HIRAID® Aged Care (versus non-adoption) over 5 and 10 years using trial data and published literature to inform assumptions [53,54,55].
Data management Data storage and accessData will be managed in accordance with the University of Sydney’s Research Data Management Policy and Procedures. Paper records will be scanned and stored electronically on the University of Sydney Research Data Store (RDS) and destroyed securely, as recommended by the policy. Where relevant, the contents of paper records (e.g. surveys) will be digitally transcribed into a standardised form on REDCap™. Paper records that cannot be digitised immediately following collection will be stored at a secure location. All data will be kept for a minimum of 15 years [56].
Data de-identification and linkageTo maintain privacy and confidentiality, all resident data will be de-identified by the project statistician prior to linkage and analysis. A unique record identifier (ID) will be assigned to each record when a dataset is received. The full dataset will be split into two sets after the assignment of record IDs: [1] one with research and clinical information and [2] one with personal identifiable information. Data analysis will be conducted using dataset 1. In situations when data from different sources need to be linked, dataset 2 will be used. All data containing identifying details will be stored separately and encrypted with a linkage or study ID key. These data will only be accessible to the statistician, the chief investigator, and designated members of the research team. Identifiable information collected during interviews will be removed at transcription or replaced with broader, non-specific terms (e.g. names of specific facilities replaced with jurisdictional descriptors).
Ethics and dissemination Data monitoringGiven the low-risk nature of the intervention and the absence of significant blinding, a data monitoring committee will not be necessary for this trial. Data will be monitored on an ongoing basis by the project statistician to ensure consistency. Data entered by research officers into REDCap™ will undergo automated plausibility checks (i.e. acceptable value range, detection of invalid characters) and regular audits.
HarmsAll adverse events will be recorded and maintained by the chief investigator and will be reported in accordance with the NHMRC Guidance Safety Monitoring and Reporting guidelines and the University of Sydney’s Safety Reporting Guidelines 2021. All serious adverse events will be reported to the University of Sydney Clinical Trial Support Office and to
留言 (0)