
記住我
The study aims to evaluate if the proposed SKOPE intervention strategies are better than existing usual care for patients with CKD. The usual care will serve as the comparator for evaluating the effectiveness and cost-efficiency of the SKOPE interventions while ensuring patient safety and ethical standards, thereby providing insight as to whether the SKOPE interventions can be adopted into clinical practice for patients with CKD.
Intervention descriptionThe intervention is a structured multicomponent intervention (MCI) comprising:
1.Training nurses or service coordinators as health coaches and hybrid follow-up approach of in-person, telephone, and secure video sessions
At least two nurses or service coordinators (preferably bilingual- Chinese, Malay, Tamil in addition to English speaking) at each of the 5 polyclinics will be trained over the Zoom platform in motivational conversation (MC), and nutritional assessment, lifestyle counseling and self-care for prevention of CKD and CVD. Training on MC will be provided over 4 h/half day by a psychologist, and nutritional assessment and lifestyle counseling will be given by a registered dietician in 4 sessions over 2 weeks, followed by a post-test. Refresher training sessions will also be conducted annually until the trial’s end. Additionally, a refresher training of 1 session will be conducted at 3 months from baseline. The MC curriculum developed for the SingHypertension trial will be adapted for CKD. The counseling approach is intended to help the patients resolve problems and make decisions to facilitate the patient’s participation and empowerment in care, and to consider the patients’ priorities along with the patient and set goals for self-care. A contextually relevant “nutrition and physical activity curriculum” will be developed in consultation with the Health Promotion Board (HPB). The recommendations will be based on Kidney Disease Improving Global Outcomes (KDIGO) management guidelines for CKD-specific diet and exercise. This will include limiting dietary sodium, low to moderate protein restriction according to CKD stage, preferably with at least 50% from plant-based sources, and increased low glycemic impact fruit [30], vegetable intake, and physical activity (at least 150 min per week of moderate-intensity), accounting for the presence of diabetes and other co-morbidities [31]. Moreover, smoking cessation, adherence to antihypertensive and anti-diabetic medications and statins, and avoidance of non-steroidal anti-inflammatory drugs (NSAIDs) and nephrotoxic agents will be emphasized. Home BP monitoring will be encouraged. The health coach’s first session will be 35 to 40 min in duration, and follow-ups in 1 month, 3 months, and then every 3 months for the project’s duration (3 months to 3 years).
All consultations will be delivered via a hybrid approach of in-person or telehealth/video meetings with a follow-up checklist (Additional file 1). Dedicated trial phones at the clinic will be used for video meetings with disabled texting and no recording features to protect patient confidentially.
2.Training physicians in algorithm-based standardized management of CKD and hybrid care delivery
A standardized treatment protocol based on KDIGO guidelines for CKD management, which includes risk stratification for ESKD using Southeast Asia Kidney Failure Risk Equation (SEA KFRE) risk equation (recalibrated by our team for Singapore [32], and for CVD will be reviewed and finalized by a team of nephrologists, cardiologists, dietician, sports physicians and pharmacologists in consultation with SingHealth primary care physicians. Based on the standardized treatment protocol developed, a physician management checklist (Additional file 2) will be designed. Primary care physicians (at least two from each of the 5 clinics) will be invited for training, and intensively trained over the Zoom platform in CKD management strategies as per trial protocol. The physicians will be trained in standardized CKD management, including nonpharmacologic and pharmacologic treatment algorithms, using a case-based curriculum over 2 sessions (Fig. 1). Refresher training sessions (1 session) also will be conducted yearly till the trial ends.
Fig. 1
CKD management algorithm for SKOPE patients
The target BP will be < 130/80 mm Hg, which takes into account the recommendations of KDIGO and the National Institute for Health and Care Excellence (NICE). A lower systolic blood pressure (SBP) target < 120 mmHg would be pursued in certain patients (i.e., with albumin-to-creatinine ratio (ACR) 30 mg/mmol or higher), if acceptable to the treating physician and the patient. Single pill combination (SPC) including renin–angiotensin–aldosterone system (RAAS) blocker and Hydrochlorothiazide-like diuretic (e.g., Hyzaar) will be offered to patients with eGFR ≥ 30 ml/min/1.73 m2. For those with eGFR < 30 ml/min/1.73 m2, individual drug prescriptions will be preferred. RAAS blockers will be the first-line antihypertensive agents, especially in the presence of diabetes and albuminuria 3 mg/mmol or higher, followed by thiazide-like diuretic and then calcium channel blocker (CCB). A loop diuretic (torsemide or furosemide) would be preferred over thiazide in the presence of edema. Moderate-intensity statin will be started on patients not already on lipid-lowering therapy.
All patients with eGFR ≥ 30 ml/min/1.73 m2 and (1) diabetes (regardless of ACR level) or (2) non-diabetes and ACR 30 mg/mmol or higher will be recommended for generic SGLT2i (dapagliflozin 10 mg daily preferably or empagliflozin 10–25 mg daily if diabetes). Other anti-diabetic agents will be adjusted if needed.
Target glycated hemoglobin will be between 6.5 and 7.5% (or between 7 and 8% if eGFR is less than 30 ml/min/1.73 m2) based on the KDIGO guidelines. Serum potassium and creatinine will be checked in 4 to 8 weeks on patients initiated on RAAS blockers or SGLT2i and flagged for action if levels > 20% of baseline.
Initial physician consultation would last about 15 min and would be completed preferably within 3 months post-randomization. Physician follow-up would be scheduled every 6–8 weeks and then every 3–4 months. At least one visit per year with a SKOPE-trained physician should be done. However, the frequency of follow-up clinic/remote visits will be determined and adjusted by level of risk factor (BP, glucose), albuminuria and eGFR changes, and symptoms, feedback from the nurse kidney health coach, at the discretion of the treating physician. Standardized referral criteria (Fig. 2) based on KFRE score, ACR levels, eGFR or ACR changes, and abnormalities or symptoms will be implemented. In every consultation and follow-up of intervention patients, the physician will also complete the physician management checklist (Additional file 2) with a total contact time of approximately 15–20 min.
Fig. 2
Nephrologist referral criteria
3.Regular CKD case review meetings
Regular CKD case review meetings will be held monthly for the first 2 months and then once every 3 months among trained nurses/service coordinators (health coaches), dieticians, and trained physicians to review the progress and CKD care plan with subsequent communication with the intervention patients, as needed. For each patient reviewed in the meeting, the health coaches will record the reasons for review, key points discussed, and action items for further patient management.
4.Subsidy of SGLT2i for CKD
At the end of each year after randomization, patients in the intervention arm who take SGLT2i (e.g., dapagliflozin or empagliflozin) as prescribed will receive a $30 voucher, regardless of whether they were already using SGLT2i before the trial or started during the trial. However, if the participants withdraw from participation during the study, they will not receive any voucher for SGLT2i treatment after the withdrawal.
Usual carePhysicians and nurses who are not trained in SKOPE treatment algorithms will treat patients in the usual care arm. There will be no restrictions on prescriptions for RAAS blockers, SGLT2i, or lifestyle advice. However, patients in usual care should not receive care from a SKOPE-trained health coach or physician trained in SKOPE intervention except in case of emergency, and will not receive trial-related subsidy on SGLT2i. However, advice regarding the management of CKD as per usual practice will continue.
Criteria for discontinuing or modifying allocated interventionsParticipants may choose to withdraw from the study at any time. However, any of the participants’ data collected until the time of withdrawal will be kept and analyzed. Participants may be withdrawn if they become ineligible, such as if the person has ESKD or cancer during the study. Involuntary withdrawal may occur due to failure to follow instructions, health or safety concerns, need for treatment not permitted in the study, or study cancelation. If this happens, the participant will be notified by phone or email. Study data collected up to that point will be retained unless otherwise requested.
Strategies to improve adherence to interventionsAs mentioned in the “intervention description,” both physicians and health coaches (site interventionists) will be trained before the intervention and retrained yearly. The health coaches will complete the follow-up checklist (Additional file 1) for each telephone follow-up, and trained physicians will complete the physician management checklist for each consultation. Case review meetings and subsidies for SGLT2i treatment will be tracked by a checklist and a log, respectively. All checklists and logs will be reviewed regularly. Additionally, the Principal Investigator (PI) and site interventionists will meet regularly to discuss challenges, share solutions, and ensure everyone is aligned. Standardized materials, including intervention slides, talking points, and a facilitator guide, will reinforce adherence.
Multiple strategies will be adopted to support participants’ adherence to the intervention. During the informed consent process, the CRC will ensure that participants fully understand the trial requirements and provide informed consent voluntarily. Throughout the trial process, the needs and preferences of participants will be prioritized. Moreover, 6 monthly telephone follow-ups will be done to monitor healthy behavior, medication adherence, and adverse events, and reimbursement will be provided to the participants for completing each yearly physical visit.
Relevant concomitant care permitted or prohibited during the trialRelevant concomitant care is permitted during the trial.
Provisions for post-trial careThe intervention is delivered by leveraging the existing healthcare system, which will also deliver post-trial care. The likelihood of harm from participation in the trial is low.
Outcomes Effectiveness outcomesThe outcome assessors will collect the outcome data yearly for all patients. The outcomes collected via participant interview include medication adherence, physical activity (international physical activity questionnaire (IPAQ) [33]), diet (8 questions adapted from locally validated 163-item semi-quantitative food frequency questionnaire (FFQ) [34]), and quality of life (EQ-5D-5L [35]). Data on medications, anthropometric measurements, BP, CVD risk score (if available), and laboratory tests will be extracted from electronic medical records (EMR), for the most recent visit before the assessment date. The clinical data will be linked with the Singapore Registry of Renal Disease for information on vital statistics and ESKD. Deaths from myocardial infarction, heart failure, or stroke (per ICD-10 codes) will be categorized as CVD deaths. The outcome assessors will also call the patients over the telephone at 6-month intervals on adverse events. Additionally, they will also extract process outcomes measures from the general practitioner (GP) and nurses’ notes.
Primary outcome measuresThe primary outcome will be the eGFR total slope from randomization to final follow-up at 36 months [36]. eGFR will be calculated using the CKD-EPI formula [29]. For the 3-year trial, 0.75 mL/min/1.73 m2/year eGFR slope reduction corresponds to 27% (95% CI, 20–34%) lower average risk for ESKD and is considered an acceptable endpoint for clinical trials by the US FDA and European Regulatory Agency [36].
Secondary outcome measures 1.Mean change in CVD risk score at 12, 24, and 36 months from the baseline as measured by The Million Hearts Longitudinal Atherosclerotic Cardiovascular Disease (ASCVD) Risk Assessment score [37]. The score is based on age, sex, race, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, treatment with statin, systolic BP, BP lowering medication use, diabetes status, current smoker and aspirin therapy.
2.Mean change in quality of life at 12, 24, and 36 months from the baseline will be assessed using EQ-5D-5L [35].
3.Proportion of receiving guideline-recommended therapies: SGLT2i, RAAS blockers, and statins at 12, 24, and 36 months from the baseline
Ancillary outcome measuresOther secondary outcomes of interest at 36 months will be as follows:
1.Proportion of subjects who experience either one of the following composite outcome and individual outcome of
a.Incident eGFR < 30 ml/min/1.73 m2;
b.Incident eGFR < 45 ml/min/1.73 m2;
c.Incident eGFR < 15 ml/min/1.73 m2;
d.Incident ACR > 30 mg/mmol (> 300 mg/g);
e.Incident dialysis; or
f.Major adverse cardiovascular events (MACE: composite of total death, myocardial infarction, coronary revascularization, stroke, and hospitalization because of heart failure) [9].
2.Proportion of subjects who experienced major adverse kidney events (MAKE)
a.Proportion of subjects with at least 40% decline in baseline eGFR or kidney replacement therapy (KRT) with mortality
b.Proportion of subjects with at least 40% decline in baseline eGFR or KRT without mortality
c.Proportion of subjects with at least 50% decline in baseline eGFR or KRT with mortality
d.Proportion of subjects with at least 50% decline in baseline eGFR or KRT without mortality
3.Mean change from baseline in KFRE score [38]
4.Proportion of subjects who experienced albuminuria defined as ACR ≥ 3 mg/mmol (30 mg/g)
5.Individual outcomes of the proportion of subjects who experienced
a.All-cause mortality
b.CVD deaths
c.Hospital admission due to coronary heart disease (CHD), heart failure, or stroke
6.Lifestyle
a.Mean change from baseline in a healthy diet
b.Median change from baseline in physical activity
c.Mean change from baseline in BMI
7.Adherence to medications
a.Mean change from baseline in adherence to antihypertensive medications
b.Mean change from baseline in adherence to antidiabetic medications
8.Mean change from baseline in antihypertensive medication (all and class specific) therapeutic intensity score (summary measure that accounts for the number of medications and the relative doses a patient received) [39]
9.Mean change from baseline in Framingham risk score (FRS) [40]
Cost-effectiveness outcomesWithin the trial cost per QALY gained will be based on incremental costs using an Activity Based Costing Approach, cost-offsets based on differential healthcare utilization based on medical and billing data, and self-reported changes in health-related quality of life based on responses to the EQ-5D-5L [35] at key assessments. Lifetime cost-effectiveness will be based on a disease progression model that converts changes in CVD risk scores to changes in lifetime QALYs. All analyses will be from the health system perspective as recommended by Singapore’s Agency for Care Effectiveness (ACE).
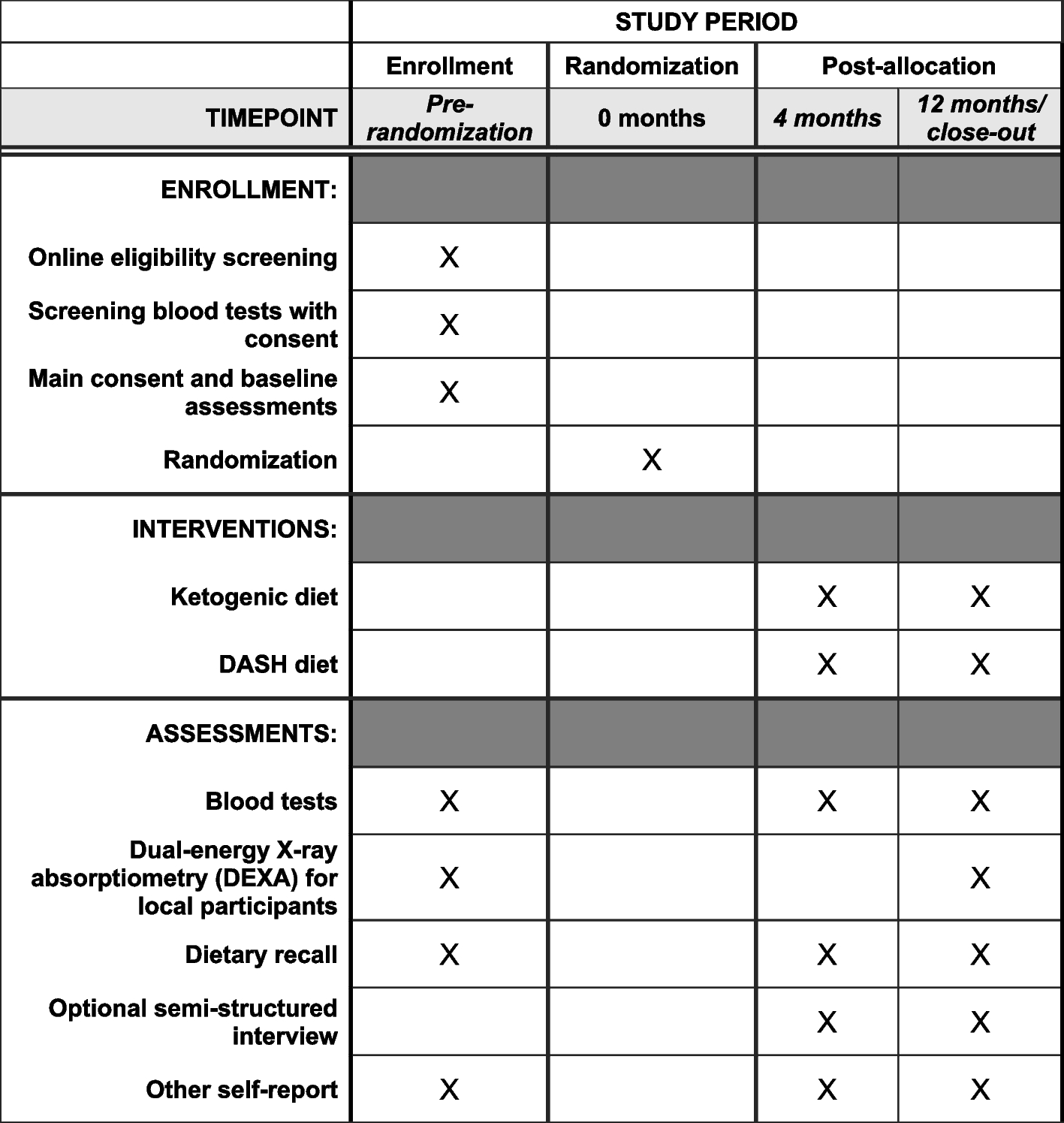
Participant timelineThe participant timeline is shown in Table 1.
Table 1 Timeline of study events for participantsSample sizeThe sample size calculated for the primary effectiveness aims to compare the total slope of change in eGFR at month 36 from the baseline between the intervention and usual care group. We anticipate a conservative effect size of at least 0.21 for the intervention on eGFR slopes with a less steep decline in the slope in the intervention group than the usual care group. The assumptions are based on the SingHypertension subgroup analysis of CKD patients and trials of SGLT2i [41]. Since SKOPE promotes CKD-specific lifestyle and pharmacologic therapies delivered via team-based structured care, its actual effect size is expected to be greater than 0.21 [42]. With an estimated standard deviation of 3.6 ml/min/1.73 m2 per year for the total slope of decline in eGFR, and a difference of 0.75 ml/min/1.73 m2 per year in the total slope corresponds to an effect size of 0.21 [13, 42]. The required total sample size will be 894 subjects (447 per arm) for 80% power at a two-sided 5% significant level, allowing for 20% drop-outs [41]. We plan to recruit an equal number of participants from SHP and NUP, with 447 participants in each cluster. Since the two NUP Polyclinics will recruit an equal number of participants, this results in (223.5) 224 participants from each, for a total of 448 from NUP. An additional 448 participants will be recruited from SHP, bringing the overall total to 896 participants.
For the secondary objectives (1a and 1b), 40 patients and healthcare professionals will be enrolled for pre-, during, and post-intervention.
RecruitmentThe trial will be conducted in 5 polyclinics in Singapore in two regional health clusters. The primary care team can identify and direct potential patients upon review of EMR to the trained CRCs at the clinic.
Upon permission from the primary physician/care team, the study team will also pre-screen the list generated via the Electronic Health Intelligence System (eHIntS) by the admin or data team and shortlist potential participants. CRC will collaborate with the physician to verify the eligibility of shortlisted patients. Those potentially eligible will be contacted on the phone by the CRC with approval from the physician/care team to invite them to participate in the trial and arrange a convenient time for a screening visit for interested patients. An invitation letter will be sent to the patients before they are called, and CRCs will call them following the standard phone script. The CRC will also approach potentially eligible patients, who visit the clinic in person. The CRC will complete the eligibility assessment and written informed consent will be obtained in person or via telephone. Screening for conditions like mental illness and terminal illness need access to patient’s medical records, where the CRC may face challenges. In that case, the CRC can do the preliminary assessment first, and formal verification of mental competence will be done when the patient visits the intervention and/or usual care physician in the clinic later.
The recruitment approaches in this study will be dynamic. Ongoing monitoring of recruitment progress will guide decisions on adapting these approaches as needed.
留言 (0)