The period between birth and childhood is critical for the development of numerous organ systems. One of the growth markers for the clinical examination and evaluation of illnesses and abnormalities in these organs is the size of these organs as liver, spleen, and kidney size [16].
In the initial phases of parenchymal diseases, the only finding would be increased size. Therefore, being aware of normal organ size for each age would facilitate the management of the subjects in terms of treatment, further evaluation, or follow-up [17]. However, a physical examination is not enough accurate to detect small increases in organ size [5]. For example, the spleen may be palpable in 15% to 17% of healthy neonates and 10% of healthy children, but in most children, it must be 2 to 3 times its normal size before it is palpable. Ultrasound may therefore first detect organ size abnormalities that indicate disease [6].
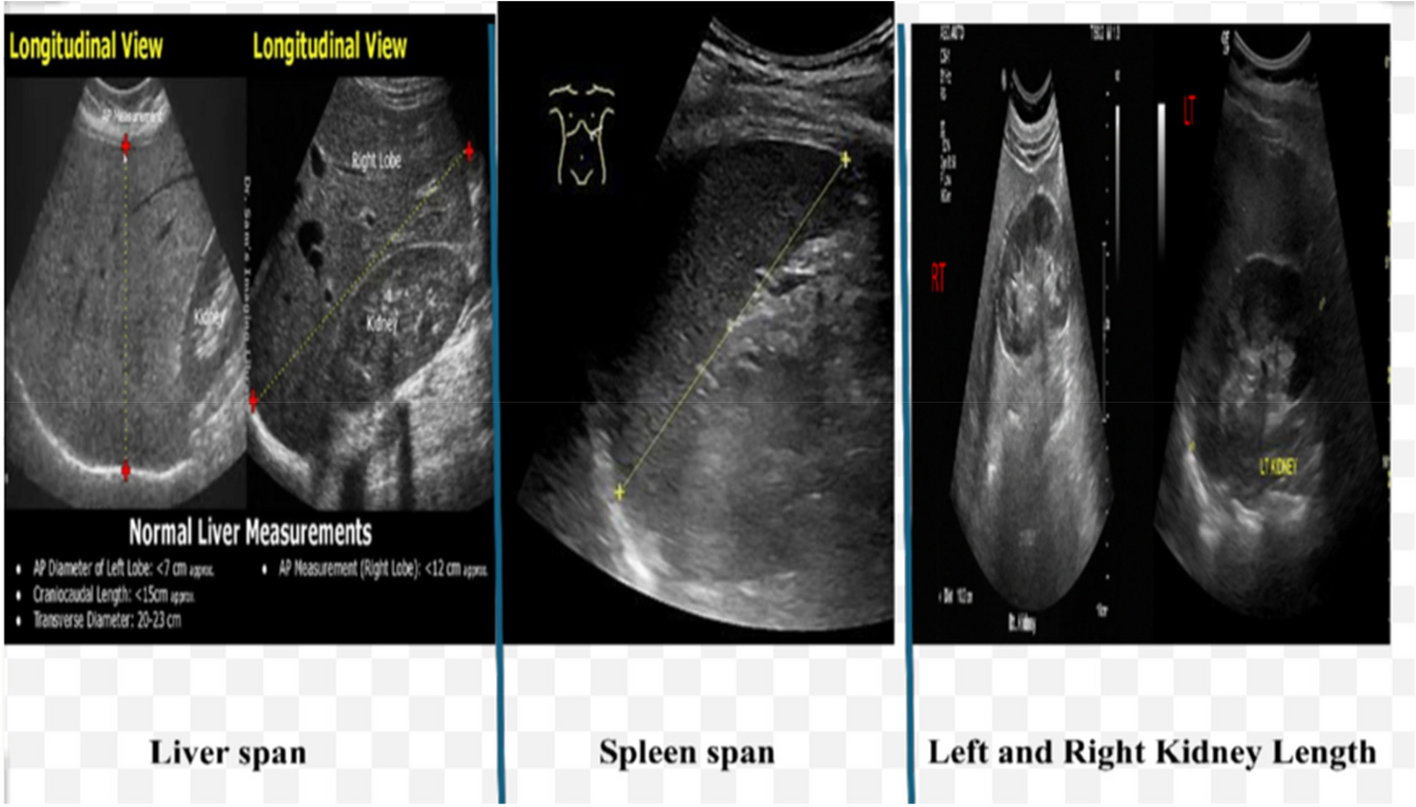
Ultrasound is an important imaging modality in children because it is a safe, quick, portable, and accurate method for the measurement of liver, kidney, and spleen size [7]. It is an established diagnostic and screening tool to assess a variety of clinical concerns. Ultrasound is used in everyday practice for emergency, inpatient, and outpatient care. Measurement of abdominal organ dimensions in children of all ages is performed in the monitoring of abdominal organ growth patterns, diagnosis, and follow-up of patients with a variety of diseases [15].
Our study provided a standard set of normal ranges of liver, kidney, and spleen size according to the age of Egyptian children, as determined by ultrasonography and clinical examination. Developing growth charts from our measures defining the normal range of measures for the liver (clinical and ultrasound), spleen, and both kidneys in Egyptian children from birth to 18 years (Tables 1, 2 and 3), (Figs. 3, 4 and 5) will be a helpful tool for radiologists and clinicians who need valid measurements that account for variability in the organ measurement to avoid overestimation of cases with enlarged organs.
Table 1 Z score of liver span (cm) for children from birth to 18 years clinically and ultrasound assessmentTable 2 Z score of spleen span (cm) for children from birth to 18 years by sonographic assessmentTable 3 Z score of kidney length (cm) for children from birth to 18 years by sonographic assessmentOn clinical and ultrasound examination, the liver span, splenic length, and kidney size were positively correlated with the patient’s age, weight, and height. The significant correlation between the sizes of the internal organs with the child’s age, weight, and height is an expected physiological correlation related to the normal growth and development pattern with advancement of the age in children.
Concomitant with our results Dhingra et al. on determining the normal values of liver and spleen size by ultrasonography in 650 Indian children, declared that the liver and spleen length significantly correlated with the patient’s age and height/length of the subjects (P = 0.0001) [3].
Huang Y et al., Kim JH et al., and Megremis S et al. demonstrated that there was no difference in abdominal organ size between boys and girls [17,18,19]. This finding was concomitant with our results as we did not find any significant differences in measures between males and females, the measures were nearly comparable so we used unisex charts.
Despite that, the study of Warnakulasuriya et al. supported our results in the absence of significant difference in the longitudinal measurements of the spleen and kidneys between both sexes, they found a significant difference in the longitudinal length of the liver between the two sexes [20].
In addition, Umeh et al. on assessing the normal sonographic dimensions of the liver, spleen, and kidneys in healthy southwest Nigerian children, found a significant correlation between the organ length and the child’s weight, height, body mass index, and body surface area, in which patients with a higher weight, height, body mass index, and body surface area tended to have larger organs [21].
The Z score of liver span (cm) for Egyptian children from birth to 18 years was assessed both clinically and by ultrasound with differences between both readings not exceeding 1 cm in the same age group, the difference was minute, especially in children above the age of 6 years.
After birth, the measures of the liver size were near that of the spleen. On observing the growth pattern of the liver and spleen with the advancement of age, it was observed that by the age of 18 years, the liver reached nearly double its birth size, while by the age of 18 years, the spleen reached triple its birth size.
In the current study, the Z score of both kidney lengths showed just minimal variation between the sizes of both kidneys ranging from 0 to 4 mm in the same individual. In agreement with our results, Warnakulasuriya et al. on assessing the ultrasonographic parameters of the liver, spleen, and kidneys among a cohort of 357 school children in Sri Lanka aged from 5 to 13 years of age, found that the longitudinal length of the left kidney was longer than that of the right one, but the difference was not statistically significant [20]. We had a limitation in our study regarding kidney and liver measures; we measured only the length as we had a large sample size so we used it as screening for nephromegaly and when suspected volume should be measured to confirm it.
In addition, Bayramoğlu et al. demonstrated that the size of the left kidney was greater than the right kidney, while according to the constant ratios and considering the maximum kidney size, it is understood that the size difference between the 2 kidneys will not exceed 1 cm [16].
Ethnic differences in the liver, spleen, and kidney measures were reported [22]. So, establishing nomograms for each ethnic group will enable better interpretation of sonographic assessments in the pediatric population.
Our Egyptian reference ranges of age-based liver, spleen, and kidney size were nearly 1 cm larger than that of the children in Turkey as reported in the study of Bayramoğlu et al. [16]. In the study of Waelti et al. on assessing the normal sonographic liver and spleen dimensions in a central European pediatric population, the liver sizes were nearly 1 cm larger than our Egyptians measures in the same age group especially those below 10 years [7].
A number of contemporary studies of normative sonographic liver size in children with different ethnicities have been published and include a Turkish population aged 0–16 years in 1998 [23], a Brazilian population aged 0–7 years in 2009 [24], an Indian population aged 0–12 years in 2010 [3], a Nepalese population aged 0–15 years in 2014 [25] and a second Nepalese population aged 0–15 years in 2015 [15].
With changes in nutrition, and genetic and environmental factors between countries, the timing of puberty also differs between ethnicities. African American boys commence puberty the earliest, at around 9 years of age, while Caucasian and Hispanic boys commence on average at age 10 years [26, 27]. This further emphasizes the importance of using charts based on data from the same ethnicity.
Our study had many points of strength, first is that it covered all the pediatric age groups with a considerable number of participants in each age group, which was insufficient in the previous studies. The second is that we checked carefully for inter and intra-observer variability with the elimination of the conflicting cases. As the mid-clavicular line is known to vary widely when evaluated by different observers, we predetermined it for the sonographic assessments, thus, consistency of measurement was ensured. A single radiologist performing the ultrasonography removed the inter-observer bias.







留言 (0)