
記住我




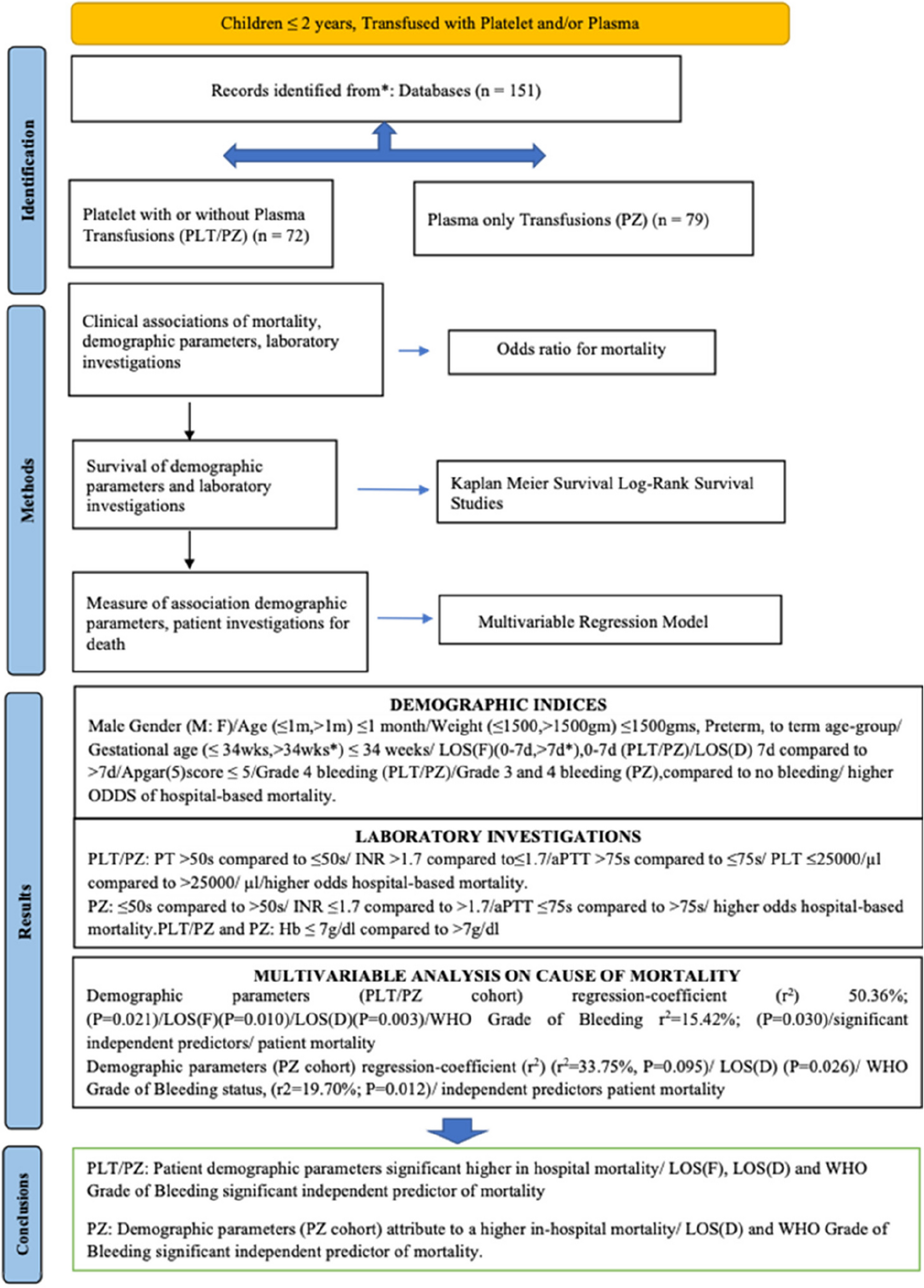


We prospectively evaluate the clinical, biochemical, and radiological data for 88 children, in outpatient clinics of the Department of Pediatrics, Cairo University Children’s Hospital, classified into 3 groups: group (A) included 22 patients with clinical, biochemically, and/or genetically proved cystinosis; group (B) 44 pathological control patients previously known chronic kidney disease (CKD) other than cystinosis, matching the age and renal stage of cystinosis patients; and finally group (C) 22 healthy pediatric volunteers with matching age. The study design and inclusion of patients are illustrated in a flow chart (Fig. 1).
Fig. 1
Flow chart of study design and inclusion of patients
The study has been performed in accordance with the Helsinki Declaration Ethics Code, 1964 for experiments including humans with its later amendments and was approved by the research ethics committee at the Faculty of Medicine, Cairo University (Approval code #MD-88–2020). Informed written consents from guardians of all participants were obtained after elucidating the aim of the work and methodology.
Demographic and clinical data of cystinosis and other CKD children were obtained from patients’ follow-up medical records. CKD staging in the study population was classified according to eGFR values calculated by the modified Schwartz formula [15].
Neuromuscular manifestations with any subsequent impairment of function were reported. A full neuromuscular evaluation was performed for all patients, including assessments of muscle tone and power using the Medical Research Council (MRC) muscle power scale, deep reflexes of both upper and lower limbs, proximal and distal reflexes using the National Institute of Neurological Disorders and Stroke (NINDS) scale, as well as sensory examination, coordination, and gait assessment. Other possible complications that may result from neuromuscular affection were also reported, such as swallowing dysfunction and restrictive lung disease.
Biochemical assayBiochemical evaluation (for participants of group A&B) includes kidney function tests, electrolytes, and inflammatory biomarkers: CRP, ESR, chitotriosidase enzyme activity, and human galectin-3 (GAL-3). The activity of plasma chitotriosidase enzyme was checked through the fluorogenic substrate 4-methylumbelliferyl-β-DN,N′,N″-triacetylchitotrioside (4-MU-C3) as previously described [16] In short, ten microliter of plasma was mixed with 100 μL of 0.022 mmol/L 4-MU-C3 (Sigma) in Citrate/Phosphate buffer, pH 5.2, 0.1/0.2 mol/L and incubated at 37 °C for 15 min. The reaction was stopped using 2 mL of 0.5 mol/L Carbonate/Bicarbonate buffer, pH 10.7. Quantification of the resulting fluorescence using a calibration curve for the substrate product 4-methylumbelliferone on the spectrofluorometer (FP6200, Jasco, Tokyo, Japan). Results were reported in nmol/ml plasma/h. Galectin-3 in serum was assayed by a commercial ELISA kit (ELK2790, ELK, Wuhan, China) according to the manufacturer’s protocol.
MRI of upper and lower limb musclesMRI radiological evaluation was conducted for participants of groups A & C. MR imaging of shoulders, arms, hands, thighs, and calf muscles was performed. MR studies were performed without IV contrast injection. Sedation was required for children less than 6 years and uncooperative older patients. Only seven patients needed sedation using oral chloral hydrate as a sedative and hypnotic drug.
Conventional magnetic resonance imaging was performed for both cases and control in random order. The radiologist was blinded to their clinical and laboratory data to avoid bias and to enhance the reliability of the findings.
The following muscles were evaluated:
Upper limb: proximal and distal muscles: deltoid, biceps, intrinsic muscles of the hands (thenar and hypothenar) (Fig. 2).
Fig. 2
Axial T1WI of upper limb muscles in cystinosis patient: 1 deltoid, 2 biceps, 3 intrinsic muscles of the hand (thenar and hypothenar). A Out of phase. B In phase
Lower limbs: posterior compartment of thighs and leg (biceps femoris, semitendinosus, and semimembranosus) and (soleus, gastrocnemius, and peroneal muscles) (Fig. 3).
Fig. 3
Axial T1WI of lower limb muscles in cystinosis patient: 1 muscles of posterior thigh compartment: (biceps femoris, semitendinosus, and semimembranous). 2 Muscles of posterior leg compartment: (soleus, gastrocnemius, and peroneal muscles). A Out of phase. B In phase
Image sequences included axial FSE T1 without fat suppression and axial STIR WI with fat suppression. The MRI sequence parameters used in our study include the following:
*T1: [out of phase] TE 2.4, TR6.7 and [in phase] TE 2.8, TR 6.7.
*T2: [STIR] TE 72, TR 1300.
*slice thickness: 4–5 mm.
*FOV: adjusted according to patient size and imaged body part. For example, the axial image to include both shoulders FOV 357 X 409.
All imaging studies were performed using a 1.5 Tesla MRI machine (Magnetom Aera, Siemens Healthiness, Germany) with a 32-channel phased-array torso coil.
MR data were transferred to and analyzed at an imaging workstation (Syngo MMWP, Siemens Healthineers, Erlangen, Germany). Conventional MR sequences (T1WI and STIR WI) were analyzed for visual assessment of muscle volume and signal intensity.
Statistical methodsData was analyzed using IBM© SPSS© Statistics version 23 (IBM© Corp., Armonk, NY) and JMP® version 13.2.1 (SAS© Institute Inc., Cary, NC). Continuous numerical variables were presented as mean and standard deviation (SD) representing normally distributed data and median and interquartile for non-normally distributed data. Intergroup differences were compared by the independent-samples t-test, Mann–Whitney U test, and Kruskal–Wallis test. Categorical data was presented as numbers and percentages and differences were compared using Fisher’s exact test. Ordinal data was compared using the chi-squared test. A two-sided p value < 0.05 was considered statistically significant.
留言 (0)