
記住我






It will highlight important adopted/adapted recommendations discussing rationale behind.
R1: Access to kidney transplantation in children (R1–15) — our guideline starts its address to paediatric nephrologists at CKD clinics, dialysis staff, and children’s families, discussing whom and when to refer to kidney transplantation? [EPG-R1–R15], thus confirming early orientation for families of CKD children at GFR 30 ml/min/1.7 m2 with kidney transplantation, being their best treatment option as compared to dialysis (EPG) (R1.8). A GFR 15 ml/min/1.7 (or higher level if severe symptoms) justify their referral to transplantation within 6–12 months of anticipated dialysis(R1.2). Earlier or later referral depends on donor availability, considering that pre-emptive KT show the best outcome (R1.8). Non or late referral as recommended (R1.9) was related to miss communication between nephrologists, dialysis, transplantation teams, and patient family neglect despite being informed and educated. However, lack of donor remains as the most leading cause (EPG) (R1.8). Dialysis support for cases with reversible barriers, until properly managed, was clear (R1.2–R1–5), while absolute contraindications were raised as well (R1.3) (Table 1). Recommendations about living kidney donation, pre-emptive KT, and MDT members are included in [R:1.8, R:1.10], while those related to age, weight, and nutritional assessment were clearly referred to (R:1.10]–[R:1.15]. Recommendations in this area are adopted as KDIGO 2020. Controversies for optimum lowest weight and height differ between centres were clarified in [R:1.12, 13, 14]. However, surgical team approval for child body habitus that accommodate adult size kidney is crucial (EPG) [R:1.15]. Superiority of pre-emptive KT has been widely discussed in the literature R [10,11,12]. (Table 1summarizes indications for referral and delay and contraindicates kidney transplant).
Table 1 EPG access to kidney transplantationR2: Assessment EPG R:2 of potential donor and transplant recipient prior to kidney transplantation must be done simultaneously in paediatric KT, since children on dialysis or CKD clinics are regularly assessed and monitored for associated morbidities, while donors will be assessed just once available. D&R assessment steps are summarized in Tables 1, 2, 3, 4, 5, 6, 7 and 8.
Table 2 Assessment targetsTable 3 Recipient assessmentTable 4 EPG donor assessmentTable 5 Guidelines for contraindications of living donation (donor selection)Table 6 Pre-transplant preparation policy steps in Nephrology and Transplantation Unit/Urology and Nephrology Center, Mansoura UniversityTable 7 Donor approval contentsTable 8 Parents approval contentsRecipient assessmentR2: Identification of the primary renal disease — We preferred to be the start in recipient evaluation since *(1) despite clinical assessment is regularly done for CKD children in CKD clinics or dialysis wards, many remain with unknown cause (14% total transplants); *(2) early identification of IKD will lead to better donor selection and ensure their families about less recurrence risk; *(3) identification of diseases with high recurrence risk to inform donor and recipient and share with MDT discussion about treatment plan (KT vs dialysis); *(4) secondary immune complex renal damage related to drugs, infections, and autoimmune disease should be controlled prior to transplant to ensure clinical and serological remissions; and *(5) urologic causes of ESRD may need extended imaging, metabolic workup, genetic testing, and surgical intervention prior to KT.
R2.1: Identification of genetic kidney disease (IKD) (refer to guideline supplement) — genetic recommendations require special discussion in any Pediatric Kidney Transplantation Guideline [6, 13, 14], IPNA 2020 [13], BTS 2018 [6], and Kidney International Reports (2022) [14]. Therefore, this area was well covered in our EPG/PKT recommendations by chair of scientific committee for Egyptian Genome Project and Inherited Kidney Disease (IKD) Group. Reasons behind our concern are as follows:
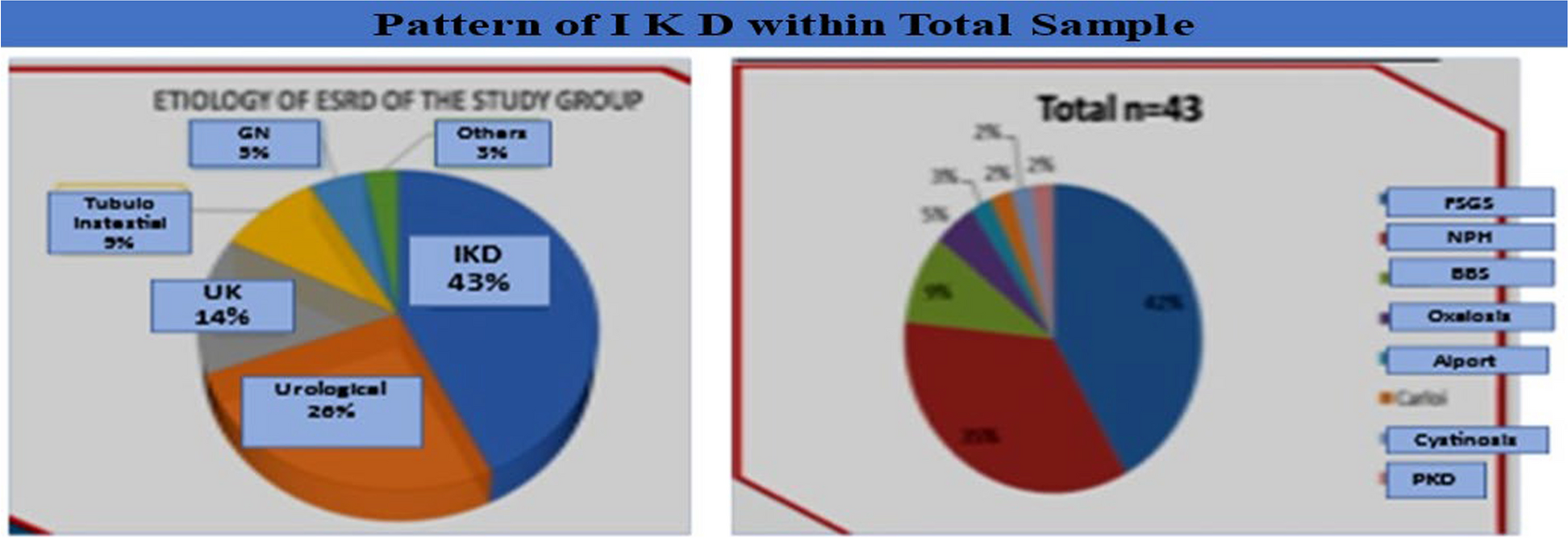
1)Egyptian profile for IKD 2009–1017 showed IKD 43% of total paediatric transplants, PKD 2%, hyperoxaluria 5%, Alport 3%, NPHS 35%, cystinosis 2%, genetic FSGS 42%, and syndromic 11% [2] (Fig. 1).
2)Genetic Expert team is essential for assessment of renal phenotype/genotype of recipients, genetic tests required, interpretation of results, proper donor selection, and family counselling (refer to R2.1a). Disease-specific recommendations for PKD, SRN, familial haematuria, and hyperoxaluria should receive special concern [R2.1b]. Living-related donor assessment [R2.1c] ensures proper donor selection for better graft outcome as well as avoid donor risk of de novo disease if missed diagnosis as carrying the mutation (Figs. 2 and 3) illustrates workup for living donor genetic assessment (refer to recommendations summery supplement) supplement.
3)Paediatric Kidney Transplantation Guidelines should focus on early identification of IKD since its recurrence is rare and their diagnosis determines their management plan [R2.1d], e.g.:
Donor selection depends on inheritance pattern; dominant variants justify nonrelated donors, while recessive variants allow related donors in most genetic diseases after thorough GT of the related donor. Both D&R should be genetically tested to avoid graft loss and ensure donor safety, especially in re-transplant with previous graft loss related to disease recurrence, e.g. FSGS, a HUS, and C3 GN.
Combined liver/kidney transplantation and not kidney alone for hyperoxaluria type 1.
Ensure safety of potential-related doners with same mutations from getting de novo disease, e.g. Alport, aHUS, and C3GN.
Early identification with target GT will avoid patients with FSGS of plasma exchange section (PES) sessions and will allow a better donor selection and ensure family with low recurrence risk. Primary FSGS was a very common cause for childhood SRNS, especially when start early and progress to ESRF rapidly. NPHSI, NPHS2, Alport COL4A 3,4,5, beside others are the most reported types.
Identification of mutation in a HUS and C3GN will avoid potential donors with mutations and confirm the need for complement inhibitor in some TCR to avoid recurrence.
Fig. 1
Primary renal disease among transplanted children, Cairo University Children Hospital 2009–2017, total cases 128 (Moustafa B. 2019) [2]
Fig. 2
EPG genetic recommendation for related living donor
Fig. 3
General and specific recommendations [R2. 1a, b] (refer to guideline supplement) afford needed knowledge to ensure both recipient and donor safety and better transplant outcome [14] (Figs. 2 and 3) show suggested workup for living donor. For extended recommendations in this area, refer to guideline link or article supplement, EPG Paediatric Kidney Transplantation Guidance.
R2.2: Identification of diseases with recurrence risk (RR) — adopted/adapted R BTS 2018, KDIGO 2020FSGS show 20–50% recurrence. Primary types show high incidence with early graft loss that makes LDKT not totally accepted NG BTS. Genetic types show low risk; however, related donor must be genetically tested for nephrin and podocin among others, to exclude the variant (1B KDIGO). Prior graft loss due to recurrence is considered a contraindication to LDKT unless donor and recipients are informed about the risk and approving NG BTS. Routine pre Kt PE is not recommended (2D KDIGO). Membranous GN RR does not contraindicate transplantation; however, D&R should be informed (NG BTS, 1B KDIGO) especially if prior graft loss (GL) (2D KDIGO). Anti-PLA2R ab should be tested prior to KT (2C KDIGO).
SLE risk for recurrence is small, D/R must be informed (B2 BTS), and KT to be done when recipient is in clinical and serological remission with minimal IMMS (1D KDIGO). Antiphospholipid pre-transplant assessment will determine anticoagulant plan (1C KDIGO).
ANCA vasculitis and good pasture disease recurrence risk (RR) do not contraindicate KT, transplantation when clinically nonactive for 6 months to 1 year and disappearance of antibodies (NG BTS, D KDIGO). Alport S recurrence is low but with a risk for de novo anti-GBM B2BTS www.transplantationjournal.com.
MPGN: We suggest candidates with C3G to be screened for genetic or acquired causes of alternative complement pathway dysregulation for treatment plan and assessment of recurrence risk (RR) (2C KDIGO). Recurrence risk fluctuates from 48% to reach 80% in re-transplant. Secondary types improve with treatment of the cause (2C KDIGO). We suggest candidates with C3G to be screened for genetic or acquired causes of alternative complement pathway dysregulation for treatment plan and assessment of RR (2C KDIGO). Genetic types show high RR. It is accepted for KT after discussion with MDT, pre-transplant GT for D/R, avoiding living-related donors, and considering both recipient disease recurrence and donor de novo disease NG-(BTS).
aHUS: We suggest grading RR, as HR, MR, LR, NG, and BTS, to determine role and availability of complement inhibitor or combined liver-kidney transplant NG BTS. We prefer nonrelated donor after completing genetic tests. Deceased donors KT in available countries are preferred since negative genetic tests do not totally exclude the variant NG(BTS).
R3: Immunological assessment [EPG; R3.1–3] [refer to supplement] RSHI/BTS 2015, BTS 2018EPG R3.1 as well as BSHI/BTS 2015 [R17], BTS18 [R5], and IPNA 2020 [R13] confirmed the value of blood group and HLA compatibility of donor and recipient for successful transplantation (AI BTS 2018) and also confirmed.
EPG R3.2 is that early and frequent screening of HLA-specific antibodies every 3 months or after any allo-sensitization event (1A BSH1 2015) [15,16,17].
R3.3 recommends use of complement dependant cytotoxicity (CDC) and flow cytometry (1A BSH12015) [15,16,17,18], pointing to high sensitivity of Luminex technology and allowing assay using beads coated with multiple classes 1 and 2 HLA (A, B, C) and HLA (DR, DP, DQ) that give bead assay with semiquantitative numeric fluorescence value (MFI).
Crossmatch using CDC detects HLA and non-HLA, IgG, and IgM, and crossmatch with flow cytometry can detect ab classes that are not detected by CDC being more sensitive [17]. Both are to be done preliminary and 1 week prior to transplant.
R3.4 recommends orientation of transplantation team with basic applied lab immunology kidney transplant workup regarding needed tests, sensitivities, and specificities, when to be repeated, and assessment of rejection risk with lab parameters with their accepted levels by most HLA labs.
R3.4 discussed limitations in desensitization for ABO, and HLA incompatible transplantation in our country was discussed since it needs special expertise and facilities that are unavailable in many countries and makes donor change as a better option (1A BSH1 2015) [17, 18].
When discussing immunological assessment guidance in children versus adults, we must consider that children have longer expected age survival that makes its age-related graft survival looks shorter, and a situation that makes a call for retransplant is possible. Therefore, rigours avoidance of sensitization in first transplant is protective for future graft. The strong immune system of children despite post-KT immunosuppression constitutes another challenge. IMMS dose is high and might be toxic in pre-sensitized. In GIT and hepatic pharmacokinetics, drug intolerance varies between children, thus making frequent monitoring a must. Children’s strong immune system makes their antigen-specific tolerance not yet a reality [19].
The Cairo University Children Paediatric Transplantation 9-year registry reported for HLA (1, 11): zero mismatch 4%, < 3/6 41% and > 3/6 55% and for DR: zero $%, 1/2 86%, all recipients PR: < 20% by Luminex (FC), and final CM: negative by CDC just before transplantation (Fig. 4).
Fig. 4
Egyptian profile immunological status (HLA, CM) transplanted children 2009–2017, Cairo University Children Hospital (CUCH) (Moustafa B. et al. 2019) [2]
R4: Psychosocial assessment recommendations — KDIGO 2020 in EPG are comprehensive because of the following:
Our community is lagging psychosocial support team and tools prior or after KT [R 4.2a, b, c].
Team's target that recipients should include *nonadherent adolescents [R4.3], [R4.4], [R4.9] who need referral to supportive programmes and for *those with cognitive or learning defects [R4.1], psychosocial disorders [R4.2], without social care [R4.3], and who need extra support after TX [R 4.3]– [4–9].
Team members should include the following: Transplant psychologists, social worker, specialized nurse, family members or caregivers, and treating doctor.
Tools to be used for assessment need family and treating doctor involvement. SIPAT assessment tool with its Arabic format is suggested in our EPG, for use in our community prioritizing its use for adolescent recipient being already an approved tool. EPG suggest putting a modified form for children with involvement of their families and care givers as recommended area for future research moderated by transplant psychologist and social workers [R4.2.C] [20]. SIPAT has no paediatric version; it is used for both children and adults. So far, there are no published studies on its use in children [21]. As with other psychosocial tests for children, a qualified psychologist will decide whether a child can complete the psychosocial assessment independently or with parental assistance. Parental involvement in the assessment is crucial for children below 12 years old since the cognitive and emotional development of younger children cannot express their concerns about such complicated details of KT. Adolescents (13–18 years old) generally have a mature cognitive capacity to understand the transplantation and its implications, but they may vary in their emotional maturity and honesty. Most experts consider the age of 12–13 years as the minimal age for independent completion of psychosocial assessment [22, 23].
Psychosocial assessment [SIPAT] suggested for children (Table 9)
A.Readiness level (patient/family) includes [R4.6].
Knowledge about disease that causes RF
Process of transplantation
Willingness for transplant
Compliance and adherence
Life style needed changes after transplant (diet, exercise, fluids, habits).
B.Social support system: Available, functioning and reliable, and housing condition
C.Cognitive function: Learning and academic status
D.Psychological status (anxiety, depression, trustfulness vs deceptive behaviour) (see appendix)
*Stanford Integrated for Transplant (SIPAT), Stanford University Medical Center (Maldonado et al. 2008)* [20]
EPG recommends support and educational programmes for transplanted children and their families to reduce nonadherence and improve child willingness, readiness, family lifestyle, and social support. KDIGO 2020 psychosocial recommendations were totally adopted with permission in our EPG and translated to Arabic language (see EPG appendix implementation tools English and Arabic formats) [20].
Table 9 Psychosocial assessment modified SIPAT suggested for use in paediatric kidney transplant (child’s families are involved)R5: Morbidity assessment for cardiac, haematological, malignancy, and bone disease in children (KDIGO 2020)Paediatric recommendations for assessment of morbidities require to respect their unique challenges. Adapted recommendations considered that (1) paediatric specialist consultation to approve child candidacy is essential in some situations, and (2) our source guideline KDIGO recommendations are mainly addressed for adults.
Therefore, adaptation was crucial to suit children CKD profile. The following recommendations related to each speciality were highlighted since they present for the transplant nephrologist a grey area that needs specialist advise.
R5.1: Pulmonary recommendation — We suggest chest imaging prior to KT for all R. candidates and also pulmonologist assessment and extended imaging for asthmatics, tuberculous, smokers, cystic lung lesions, interstitial fibrosis, pulmonary hypertension, autoimmune diseases, syndromic, and metabolic, for exclusion of those with severe obstructive or restrictive lung disease from KT (KDIGO 2020, GPP).
R5.2: Neurological recommendations — Progressive neurodegenerative diseases, syndromic, genetic, metabolic with extra-renal manifestations, impaired cognitive function, or severe psychiatric disorders need neuro and psychosocial consultation for transplantation candidacy. Assessment should be considered if their quality of life is expected to be improved after transplant or not, and supportive programmes should be available for those approved for KT (GPP — good practice point).
R5.3: CVD recommendations raised the high significance of BP assessment, ECG, echo, and tissue Doppler in assessment and cardiac consultation for any child indicated for kidney transplantation. Those with cardiac disease, abnormal echo indices, dyslipidaemia, uncontrolled hypertension, arrythmias, thrombotic history, long period on dialysis, and pulmonary hypertension should have rigorous assessment by a cardiologist. Left ventricular dysfunction (ejection fraction < 30%, severe valvular disease, severe heart failure, pulmonary pressure > 60) contraindicates transplantation. Multisystem renal diseases as autoimmune D, syndromic children, and metabolic disorders as children with hyperoxaluria with high oxalate load should do cardiac US with speckle tracking US at time of diagnosis and followed yearly or according to results and disease evolution (C. (OxalEurope) 2022). Cardiac MRI may be requested prior to transplantation (NG [24] European Hyperoxaluria Consortium (OxalEurope) Registry 2022).
Antihypertensives should be used to control hypertension prior to KT (2A KDIGO), to be stopped only at the day of the operation to allow adult graft perfusion on operation (NG KDIGO 2020).
R5.4: Haematological recommendations: We do not recommend routine thrombophilia screening (1C KDIGO), only in candidates with reported thromboembolic events or positive family history (2C KDIGO). Systemic lupus erythematosus patients or those with features of antiphospholipid syndrome should be screened for APL Abs (2C KDIGO). Children on anticoagulants or antiplatelets should not be excluded from kidney transplant (NG KDIGO).
Single antiplatelets (aspirin, clopidogrel) can be continued while waiting for KT (NG KDIGO). The decision to delay KT for those on dual antiplatelet is to be made in consultation with haematologist and when the risk of stopping medication or operating while on treatment exceeds the anticipated benefit of transplantation. Antiplatelets except aspirin should be stopped 5 days prior to transplantation unless risk of thrombosis is high (NG KDIGO) [R5.4].
Clopidogrel, as a platelet aggregation-inhibiting drug, in addition to inhibition of cyclooxygenase pathway by aspirin has not been approved for paediatric use. However, it has been long used off-label and reported its safety [25].
Although rivaroxaban and dabigatran have been approved as ODACs for use in paediatrics, we do not suggest its use except when there is expertise using DOACs perioperatively and access to DOACs reversal agents (NG. KDIGO). Considering that there is limited data on its safety and effectiveness of reversal agents in paediatric patients and being expensive and not available in our institution, therefore prothrombin complex concentrate PCCs might be used as an alternative option [26]. In a recent survey of paediatric haematologists on paediatric PTS requiring reversal of life-threatening bleeding secondary to direct factor Xa inhibitor DFXaL, they found a 44% preference for use of adexanet alfa which is used for reversal of rivaroxaban with 55% choosing PCC [27]. Rodriguez, V. initial phase 2 trial is using a newer drug ciraparantag, which can neutralize DFXaL [apixaban & rivaroxaban] and heparin [28]. Idarucizumab is currently being investigated in children [29].
Therefore, EPG recommends switch to warfarin as oral anticoagulant with available reversal agent vit. K as an alternative option considering the limited expertise with DOACs reversal [R5.4].
Low-molecular-weight heparin should not be recommended for postoperative routine use and should be avoided in HIT [R5.4]. All scenarios discussed should be approved by transplant haematologist.
Candidates with sickle cell disease or thalassemia not to be excluded from KT, in the absence of active or severe extra renal sickle cell disease, and after haematologist assessment (IC KDIGO)
Leukaemia, lymphoma, PTLD, and prior hematologic malignancy to be transplanted only after achieving long remission and approved by transplant consultant haematologists and oncologist (NG KDIGO). Oncologist consultation for candidacy should be done for all premalignant or HR of accelerated progression: www transplant journal.com.
R5.5: GIT recommendations — although KDIGO consider upper endoscopy not a routine indication for all recipient, it is EPG suggested as routine for our TCR children since gastrooesophageal reflux GERD will be identified. Long-term use of steroids and some IMMS after transplant are not GIT tolerated and require proper upper GIT assessment [R5.5] (GPP).
We recommend delaying KT with acute pancreatitis, high S amylase for 3 m until resolved (NG), and not to exclude chronic pancreatitis from KT (NG KDIGO).
IBD are not excluded from KT. Delayed if active, screened for bowel cancers, and time of KT should be approved by gastroenterologist (NG KDIGO).
R5.6: Delay cases with acute hepatitis until recovery — cases with liver cirrhosis should be well assessed by hepatologist for oesophageal varices, screened for hepatocellular carcinoma, to decide management plan as liver kidney transplant (KDIGO).
R5.7: Diabetic CKD children are candidates for kidney transplantation since we do not have pancreatic-kidney transplant option; they need well assessment and metabolic control prior to TX and frequent follow-up. Combined use of steroids and TAC in such HR group should be well assessed per case (GPP).
R5.8: Mineral bone disease (MBD), hyperpara, is common among CKD children as they are mostly on conventional dialysis 3 h/3 days/week, which do not allow proper phosphate clearance, and severity of pre-transplant SHPT can lead to post-transplant THPT hyperparathyroidism and an increased risk of graft loss [30, 31]. Secondary hyperparathyroidism (SHPT) and tertiary hyperparathyroidism (THPT) with bone disorders ar a great challenge in children that is expected to progress especially after long use of steroids after transplant. Bone problems will be evident within the first month after transplant. Risk factors include age, sex, frailty, previous fractures, hyperpara, and cumulative steroid exposure. Therefore, several nephrologists stress the importance of treating SHPT before kidney transplantation to reduce the incidence and prevent complications of THPT in transplant recipients [32, 33]. Post-TX vitamin D, bisphosphonates calcitonin, and cinacalcet should be used. Since cinacalcet is expensive and non-affordable, and surgery remains as controversy in children, management of bone problems in children remains a challenge.
EPG R5 recommends measuring Ca, phosphorous, and PTH before transplantation. Treat hyperpara medically or surgically before TX as KDIGO-CKD-mineral and bone disorder (CKD-MBD guideline D2) [34]. Parathyroidectomy should be considered for those with failed medical treatment or severe complications of hyperpara B KDIGO. Parathyroidectomy in children when failure of medical treatment deserves further surgical expert care [R5.8].
R6: Infection status assessmentPre-TX viral screening for infection for donors and recipients is crucial. Recipient vaccination and boosting as well as post-transplant viral monitoring and antiviral prophylaxis are adopted from KDIGO 2020, considering our local profile as reported in 9 years registry 2009–2017 of Egyptian transplanted children in Cairo University Children Hospital [2] that showed all donors and recipients were HBVsAg and HIV Ab negative at the time of transplantation, thanks to compulsory HBV vaccination. Recipients with + CMV constitute ¼ of total paediatric transplants where HR (D + R −) 18% and most common CMV status was (D + R +) 79%. All donors showed normal Ab titre for HCV, while 20% of the recipients showed low titre viremia; they were all on HD, and many received direct-acting anti-hepatitis C virus drugs (DAAD) prior to TX (Fig. 5) [2].
Our national EPG strategy for children with HCV prior to KT needed to be tailored, since they showed the following: *high incidence among CKD on HD, *low virulence genotyping, and *seronegative donor availability. Such status suggests pre-KT antiviral treatment unless the available donor is HCV + . DAAD approval by ethical committee based on local clinical trials supports the start of treatment with regular PCR monitoring after KT. Accepting TCR with short remission after treatment is related to time of donor availability.
Compulsory HBV vaccination in children and boosting those with low titre prior to TX, screening of D&R with HBVs and core Ab, and non-accepting HBV donors protect TCR from acquired infection. Our protocol for other viruses is adopted as KDIGO [EPG 6.1].
EBV and CMV were adopted as KDIGO (refer to Recommendations) [EPG R6.1].
Since TB in our community starts to show up despite vaccination, we confirm pre-transplant TB screening workup and, whenever, sterile pyuria for its exclusion [EPG R6.2].
Recurrent and complicated UTI should be treated before KT and followed as recommended by KDIGO [EPG R6.4].
Fig. 5
Viral status (HCV, CMV) transplanted children 2009–2017, Cairo University Children Hospital (CUCH) (Moustafa B. et al. 2019) [2]
R7: Urological assessment (R1 to 10) of paediatric recipient is crucial in our area, since 33% of total paediatric transplants are 2ry to urological causes. Our national recommendations are mostly adopted/adapted from EAU and KDIGO considering our local paediatric urological profile of kidney and UT challenges and HR factors as well as good practice points GPP reflecting our transplant surgeons experience, e.g. EPG recommend.
R1: Cong. anomalies of kidney and urinary tract (CAKUT) and voiding dysfunction, stones, obstructive uropathies, and VU
留言 (0)