
記住我






A 34-year-old G3P1L1A1 with spontaneous conception at 30 weeks of gestation complicated by fetal growth restriction and maternal overt diabetes which was well controlled. She was referred to our center in view of newly found Doppler changes suggestive of absent diastolic flow with brain sparing effect. She was subsequently admitted for urgent cesarean section and underwent primary low transverse cesarean section with delivery of a baby boy weighing 1.1 kg. The delivery was completely atraumatic and no cracks, or pops were appreciated by the obstetricians. The mother recovered from the surgery uneventfully. At the time of delivery, the newborn had Apgar score of 7 at 1 min which improved to 9 at 5 min. He was shifted to the NICU and kept on bubble CPAP and received one dose of surfactant after which he was stable on minimum settings on CPAP.
After delivery, the left arm of the baby was noted to have a lateral crease at the shoulder beyond the axilla with reduced spontaneous movements on the affected side compared to contralateral side. A detailed examination revealed swelling over the left shoulder and arm in hyperextended position with no active flexion of the affected arm. Restriction of movement was present but there was no pain on passive movements. The swelling was thought to be muscular in origin. There was a palpable void in the glenoid fossa. The limb was well perfused and pink, and the palmar reflex was intact. Clinically no generalized ligament laxity or neurological deficit was noted.
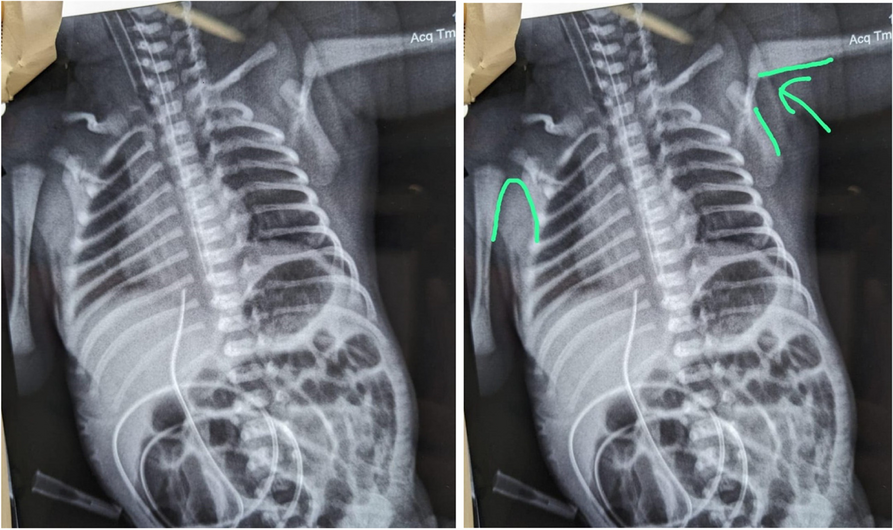
X-rays (Fig. 1) were obtained subsequently which confirmed the diagnosis of shoulder dislocation. The orthopedic department was consulted for the reduction of the dislocated shoulder.
Fig. 1
Anteroposterior radiograph in the newborn taken after delivery showing dislocated left shoulder (anterosuperior) and Shenton’s arc is broken. Also, distance between humeral head and glenoid increased due to superior and anterior dislocation
As shown in Fig. 1, there is incongruity of scapulothoracic arch in anteroposterior view of shoulder radiograph. This arch is disrupted, so there is subluxation/dislocation of shoulder. This is also known as Shenton’s line. Normally, it is a sharp inverse U-shaped line formed by medial aspect of the proximal humeral metaphysic and inferolateral border of scapula.
Gentle reduction was attempted by Kocher’s maneuver namely elbow flexion to 90°, adduction, external rotation, and forward flexion of the shoulder to lever the humeral head into the glenoid fossa [4]. Though no confirmatory clunk was appreciated, ultrasonography confirmed that the left cartilaginous humeral head was noted to be in the glenoid fossa. There was no physeal injury noted. The post-reduction X-Ray (Fig. 2) confirmed the same through restoration of the Shenton’s arc, although there was no ossification center noted in the humeral head.
Fig. 2
Anteroposterior radiograph after reduction showing Shenton’s arc is restored
The arm was swathed to the baby’s chest in an adducted and internally rotated position, with the elbow in flexion, while avoiding the nipple area while strapping.
Imaging repeated after 2 weeks revealed that there was no repeat dislocation, and no active management was suggested from the orthopedic department. The baby continued to spontaneously move the arm and perfusion of the upper limb remained intact after this maneuver. Biceps, triceps, hand flexor, and/or extensor function remained intact throughout the hospital stay.
After 2 weeks, ultrasonography of the shoulder joint was done which revealed that the humeral head was situated in the glenoid fossa. Subsequent follow-up visits at 6 weeks and 3 months confirmed the same. No new dislocation noticed.
It remains to be seen whether the shoulder might get dislocated again over time. Currently, the baby is discharged from the NICU and doing well.
留言 (0)