
記住我







Data were extracted from the Health Insurance Review and Assessment Service (HIRA) database, a nationwide database that includes approximately 97% of the entire population of South Korea. Comprehensive data, including demographics, disease diagnosis based on the International Classification of Diseases, Tenth Revision (ICD-10) code and rare intractable disease (RID) code, medications, and medical procedures, are included in the HIRA database [15]. The RID code is registered after a thorough review by the National Health Insurance (NHI) and the corresponding healthcare institution to ensure compliance with the uniform diagnostic criteria provided by the NHI [16].
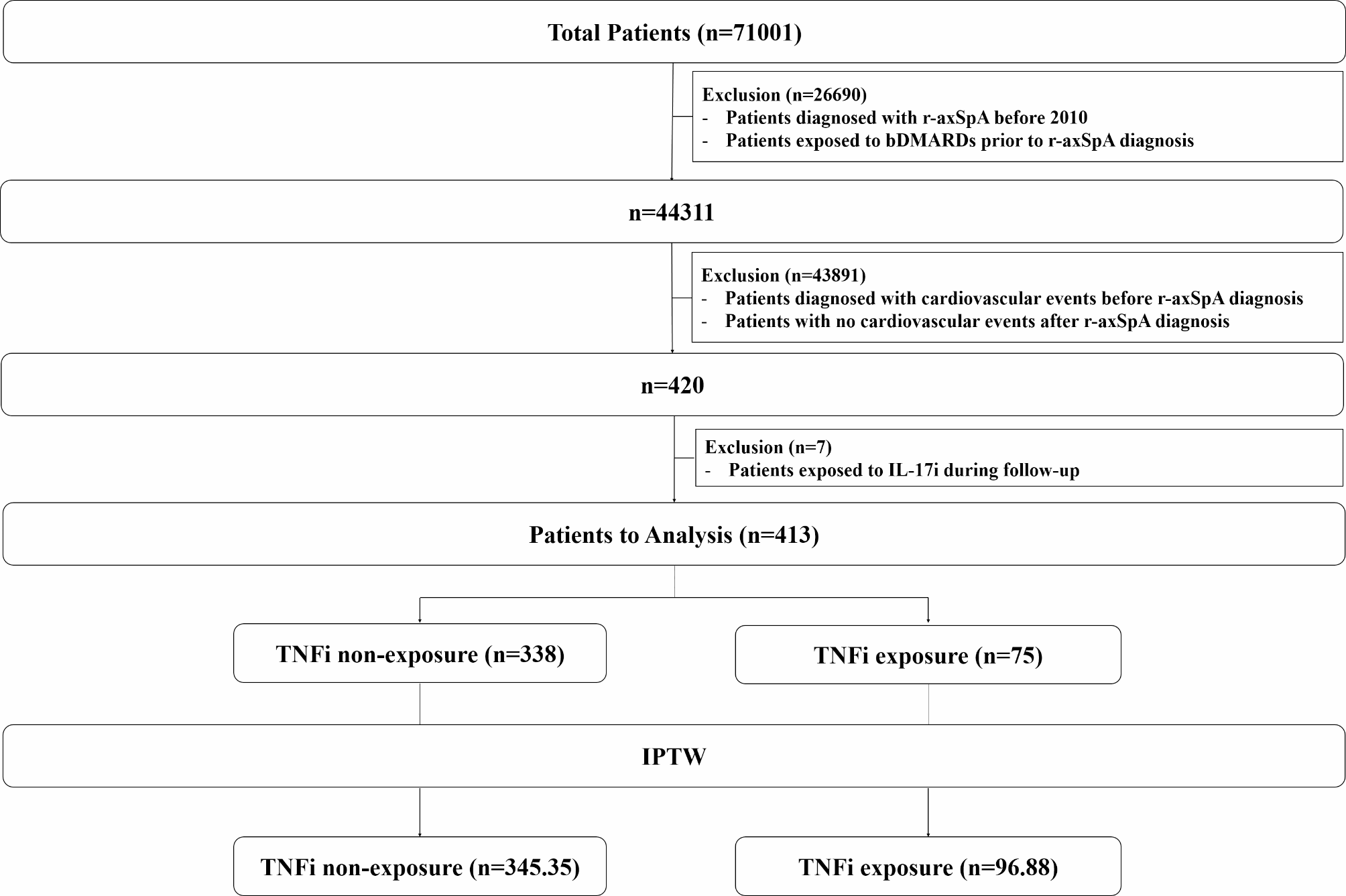
Study cohortAll patients with r-axSpA were initially screened from the database. r-axSpA was defined as ICD-10 code M45 with RID code V140 [16]. Patients with the following criteria were excluded: (i) diagnosis of r-axSpA before 2010, (ii) any bDMARDs exposure prior to the diagnosis of r-axSpA, (iii) cardiovascular events (myocardial infarction [MI] or stroke) prior to the diagnosis of r-axSpA (as patients with cardiovascular events prior to r-axSpA diagnosis might have different risk of recurrent cardiovascular events before and after they are diagnosed with r-axSpA, patients with cardiovascular events prior to the r-axSpA dianosis were excluded to avoid the influence of r-axSpA itself), (iv) no cardiovascular events after the diagnosis of r-axSpA, and (v) exposure to interleukin-17 A inhibitors (IL-17i) during follow-up. As a result, 413 patients with r-axSpA who were diagnosed with cardiovascular events after r-axSpA diagnosis were included in the analysis (Fig. 1). The index date was defined as the date of the first diagnosis of cardiovascular events. Patients were followed from the index date to the date of cardiovascular event recurrence, the last date with claims data, or December 31, 2021, whichever occured first.
Fig. 1
Flowchart of the study. r-axSpA, radiographic axial spondyloarthritis; bDMARDs, biological disease-modifying antirheumatic drugs; IL-17i, interleukin-17 A inhibitors; TNFi, tumor necrosis factor inhibitors
This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (IRB No: 3-2023-0271). The HIRA database provides fully anonymized data, and therefore, the requirement for informed consent was waived.
ExposureExposure to TNFi was assessed as a binary variable (ever used during follow-up: yes or no). According to the national reimbursement policy of South Korea, TNFi can be initiated in patients with active disease despite treatment with non-steroidal anti-inflammatory drugs (NSAIDs) with or without conventional synthetic DMARDs for at least 3 months.
Covariates and outcomeAge, sex, disease duration of r-axSpA, and the presence of hypertension, type 2 diabetes, dyslipidemia, and chronic kidney disease (CKD) on the index date were included as covariates. Hypertension was defined as ICD-10 codes I10‒I13 and I15 with prescriptions for antihypertensive agents; type 2 diabetes was defined as ICD-10 codes E11–14 and at least one annual claim of a prescription of antidiabetic agents; dyslipidemia was defined as ICD-10 code E78 with prescriptions for lipid-lowering agents; and CKD was defined as ICD-10 code N18 or N19 [17, 18]. Medications (methotrexate, sulfasalazine, glucocorticoids, non-selective NSAIDs, selective cyclooxygenase-2 [COX-2] inhibitors, antiplatelet agents, anticoagulants, statins, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, beta-blockers, sodium-glucose cotransporter-2 inhibitors, and glucagon-like peptide-1 receptor agonists) used during the follow-up were also included as covariates.
The outcome of this study was recurrent cardiovascular events (MI or stroke). MI was defined as ICD-10 code I21 or I22 during hospitalization; stroke was defined as ICD-10 code I63 or I64 during hospitalization with claims for brain magnetic resonance imaging or computed tomography [19]. Any MI or stroke event that occurred at least 28 days after the first event was considered a recurrence [20].
Statistical analysesPatients were categorized into TNFi non-exposure and TNFi exposure groups. Characteristics are summarized as mean (± standard deviation) or numbers (%) for continuous or categorical variables, respectively. Student’s t-test was used for comparing continuous variables, and the χ2 test or Fisher’s exact test was used for comparing categorical variables between the two groups (TNFi non-exposure vs. TNFi exposure). The number of outcomes (%) and crude incidence rates were calculated for the TNFi non-exposure and exposure groups, respectively.
To mitigate confounding by indication, we used inverse probability of treatment weighting (IPTW) based on the propensity score. The propensity score for TNFi exposure was estimated using a multivariable logistic regression model that included age, sex, disease duration, hypertension, type 2 diabetes, dyslipidemia, and CKD. Patients who were not exposed to TNFi were assigned a weight of 1/(1–propensity score) and those who were exposed to TNFi were assigned a weight of 1/propensity score. After IPTW, continuous variables were expressed as the weighted mean (standard error), and categorical variables were expressed as weighted numbers (%). An inverse probability weighted Cox regression analysis was performed to assess the hazard ratio (HR) and 95% confidence interval (CI) of recurrent cardiovascular events according to TNFi exposure. A univariable model was used, followed by a multivariable model adjusted for medications (use of methotrexate, sulfasalazine, glucocorticoids, non-selective NSAIDs, selective COX-2 inhibitors, antiplatelet agents, anticoagulants, statins, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, beta-blockers, sodium-glucose cotransporter-2 inhibitors, and glucagon-like peptide-1 receptor agonists). All reported p-values are two-sided, and statistical significance was set at p < 0.05. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
留言 (0)