Study design and participants
This study was undertaken within the framework of an ongoing prospective study based in memory clinics, with participants primarily recruited from the National University Hospital (NUH) and a limited number (n = 21) from St Luke’s Hospital, Singapore. Detailed study design and rationale have been previously described [15]. In brief, participants were considered eligible if they were ≥ 50 years old, possessed sufficient language skills for neuropsychological assessment, and met the diagnostic criteria specified below. Exclusion criteria included diagnoses of major psychiatric illness or substance abuse disorder, cognitive impairment due to traumatic brain injury, multiple sclerosis, tumor, epilepsy, or systemic disease, and significant visual or auditory abnormalities. Participants were assigned at research consensus meetings into one of the following diagnostic categories: (1) no cognitive impairment (NCI): Absence of objectively measurable cognitive impairment in a formal neuropsychological test, (2) cognitive impairment no dementia (CIND): presence of objective cognitive impairment in at least one cognitive domain, as determined by performance on a locally-validated neuropsychological test battery, without fulfilling the diagnostic criteria for dementia as outlined in Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition (DSM-IV) [16], and (3) dementia: diagnosed in accordance with DSM-IV criteria [16].
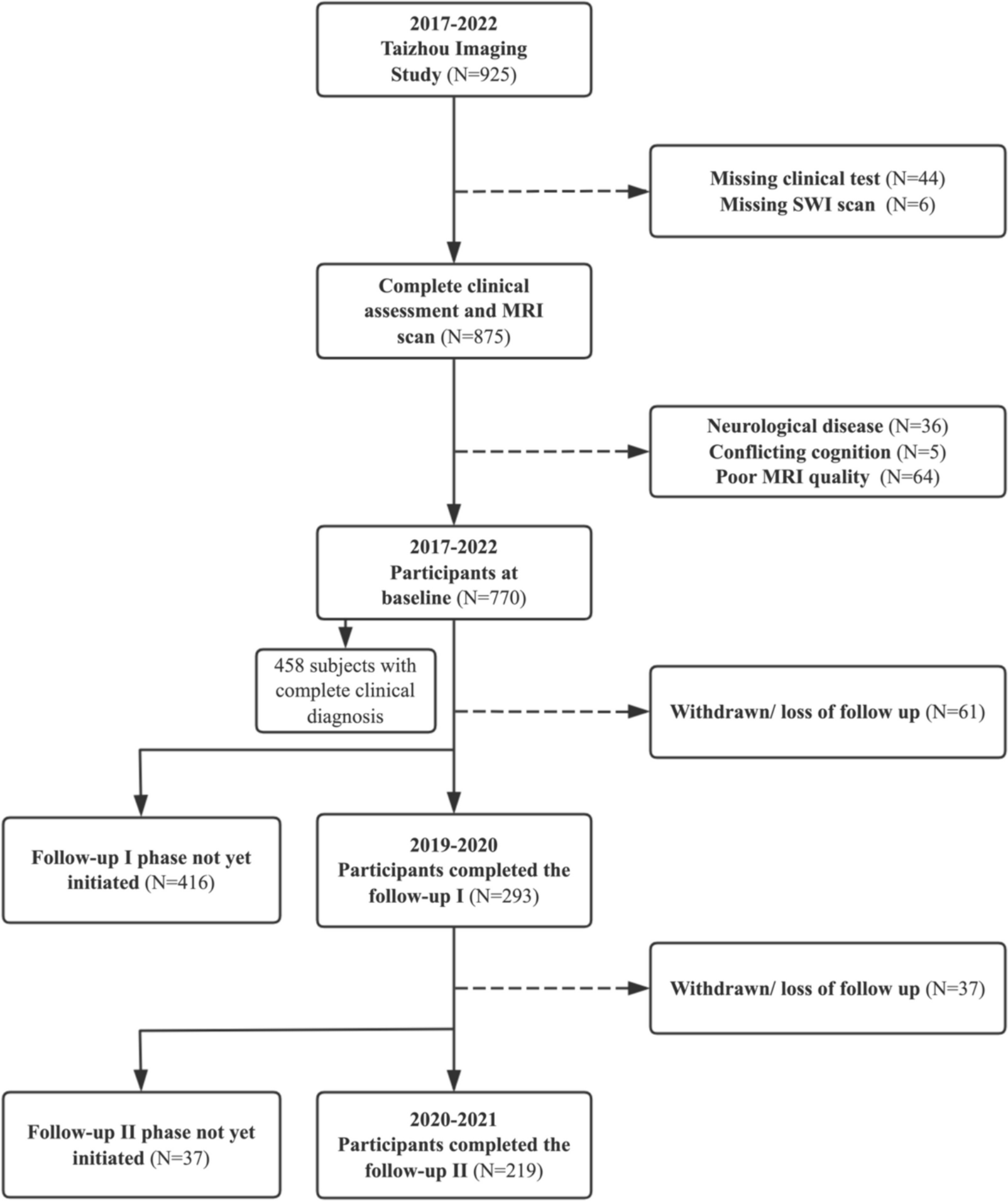
All participants were subjected to a thorough evaluation, including physical examinations and neuropsychological assessments, along with brain MRI scans. From the total of 700 participants recruited between August 2010 to August 2020, participants with either missing or suboptimal quality brain MRI scan (n = 44), and those with incomplete baseline neuropsychological data (n = 2) were excluded. In the main analysis, 654 participants (n = 637 recruited from NUH) were included for the cross-sectional analysis, and 614 participants (n = 600 from NUH) for the longitudinal analysis after excluding 40 participants without any follow-up. To investigate the potential role of Alzheimer pathology in the association of diabetes and cognitive decline, a subset of participants with available baseline p-tau181 (n = 506) and p-tau181/Aβ42 ratios (n = 478) were included. Of these Alzheimer biomarker subset groups, 476 with baseline p-tau181 and 448 with baseline p-tau181/Aβ42 ratios had at least one follow-up study visit and were therefore included for the longitudinal analyses.
Neuroimaging
At baseline, brain MRI scans were performed using 3T Siemens Magnetom Trio Tim scanner, with a 32-channel head coil at the Clinical Imaging Research Centre, National University of Singapore. The neuroimaging protocol included T1‐weighted, T2‐weighted, fluid‐attenuated inversion recovery (FLAIR), and susceptibility weighted images (SWI).
WMHs were segmented by the lesion growth algorithm (LGA) implemented in the LST toolbox (version 3.0.0), which requires both T1-weighted and FLAIR sequences [17]. The total whole-brain WMHs volume was log-transformed to reduce skewness. Additionally, the Modified Fazekas scale was used to assess WMHs severity [18].
Lacunes were characterized as round or ovoid lesions, typically ranging from 3 to 15 mm in size, localized in the subcortical regions, exhibiting low signal intensity on T1-weighted and FLAIR sequences, high signal intensity on T2-weighted images, and a hyperintense rim [19];
CMBs were identified as focal, round hypointense lesions with blooming effect on SWI and were graded using the Brain Observer Microbleed Scale [20];
CMIs were assessed using T1- and T2-weighted, as well as FLAIR images. They were characterized as hypointense lesions on T1-weighted images, with a diameter of less than 5 mm, confined to the cortex, and perpendicular to the cortical surface. The location of a hypointense cortical lesion identified on T1-weighted images was verified using FLAIR and T2-weighted images. The lesion was classified as a definite CMI if it exhibited hyperintensity or isointensity on FLAIR and T2-weighted images. Conversely, the lesion was excluded as a CMI if a hypointense signal was detected at the same location on FLAIR or T2-weighted images [21];
Cortical infarcts were characterized as localized lesions affecting cortical gray matter, exhibiting signal intensity resembling cerebrospinal fluid, accompanied by a hyperintense rim on FLAIR imaging, and variable degrees of tissue loss, with prominent adjacent sulci and ipsilateral ventricular dilation [19];
ICS was identified as a reduction in luminal diameter exceeding 50% in any of the assessed intracranial vessels, as evaluated through three-dimensional time-of-flight magnetic resonance angiography [22].
Based on MRI markers of small vessel disease (SVD) included in our study, we calculated the total SVD burden on an ordinal scale from 0 to 4, with 1 point added for each of the following: ≥ 1 lacunes, ≥ 1 CMBs, ≥ 1 CMIs, and the presence of WMHs with ≥ 2 Fazekas score. There were 486 participants with at least 1 follow-up CeVD data. We developed an incident CeVD score on an ordinal scale from 0 to 5, assigning 1 point if any incidence or progression observed in lacunes, CMBs, WMHs (as defined by the Modified Rotterdam Progression Scale), cortical infarcts, and ICS.
Neuropsychological assessment and ascertainment of incident dementia
All participants annually completed neuropsychological assessments that included Clinical Dementia Rating Sum-of-Boxes (CDR-SOB) and a locally validated neuropsychological battery [23]. This battery, aligned with the recommendation of the National Institute of Neurological Disorders and Stroke and the Canadian Stroke Network (60-minute NINDS-CSN) [24], evaluated six cognitive domains: Attention (Digit Span Forward and Backward), executive function (Verbal Fluency, Color Trail Test A&B), language (15-item modified Boston Naming Test), visuospatial function (Rey Complex Figure Test-copy), visuomotor speed (Symbol Digit Modalities Test), and memory (Rey Complex Figure Test-immediate/delayed recall and recognition, Hopkins Verbal Learning Test immediate/delayed recall and recognition). Composite z-scores of global and domain-specific cognition were computed as previously described [15]. Higher z-scores indicated better cognitive performance.
Dementia diagnoses for each participant were made at weekly consensus meetings attended by a panel comprising neurologists, psychologists, and researchers. Incident dementia was defined as the transition of participants from NCI or CIND to dementia, and the diagnosis of dementia was made according to DSM-IV criteria [16].
Plasma sampling and analysis
Non-fasting blood was collected from participants and subjected to plasma extraction before storage at − 80◦C until analysis. All biomarker measurements were performed by evaluators blinded to clinical data at the Sahlgrenska Academy, University of Gothenburg, Sweden, utilizing the Simoa HD-1 or HD-X platforms (Quanterix, Billerica, MA, USA). Detailed methodology has been described previously [25]. In brief, p-tau181 was quantified using the AT270 mouse monoclonal antibody (MN1050; Invitrogen, Waltham, MA, USA), specific for the threonine-181 phosphorylation site, through an ultrasensitive Simoa immunoassay. Aβ42 was determined using the Neurology 3-plex A assay kit (Quanterix, Billerica, MA, USA).
Diabetes assessment and covariates
Diabetes was defined by either self-reported history of diabetes or the use of glucose-lowering medication at each study visit. There were 48 participants with a self-reported history of diabetes who did not report using any glucose-lowering medication. A detailed questionnaire was administered to all participants to collect information on age (years), sex, education (years), current smoking (yes/no), and medical history, including hypertension, hyperlipidemia, stroke, atrial fibrillation, myocardial infarction, coronary angioplasty, pacemaker implantation, and congestive heart failure. All medical history was verified by medical records if available. Cardiovascular disease (CVD) was defined by presence of atrial fibrillation, myocardial infarction, coronary angioplasty, pacemaker implantation, or congestive heart failure. Apolipoprotein E (APOE) ε4 status was determined by the presence of at least one ε4 allele.
Statistical analysis
We compared baseline characteristics between diabetes and non-diabetes using Pearson’s chi-squared test (for categorical variables), two-sample t test (for continuous normally distributed variables), or Mann-Whitney U test (for continuous non-normally distributed variables). Poisson regression was used to explore association of diabetes with lacunes, CMBs, CMIs, ICS, and cortical infarcts at baseline as count data, while linear regression was used to examine association of diabetes with log transformed WMHs. The models were adjusted for age, gender, and education (Model 1), and additionally for current smoking, hypertension, and hyperlipidemia (Model 2). When the outcome was small vessel disease, further adjustments were made for other MRI markers of small vessel disease (Model 3).
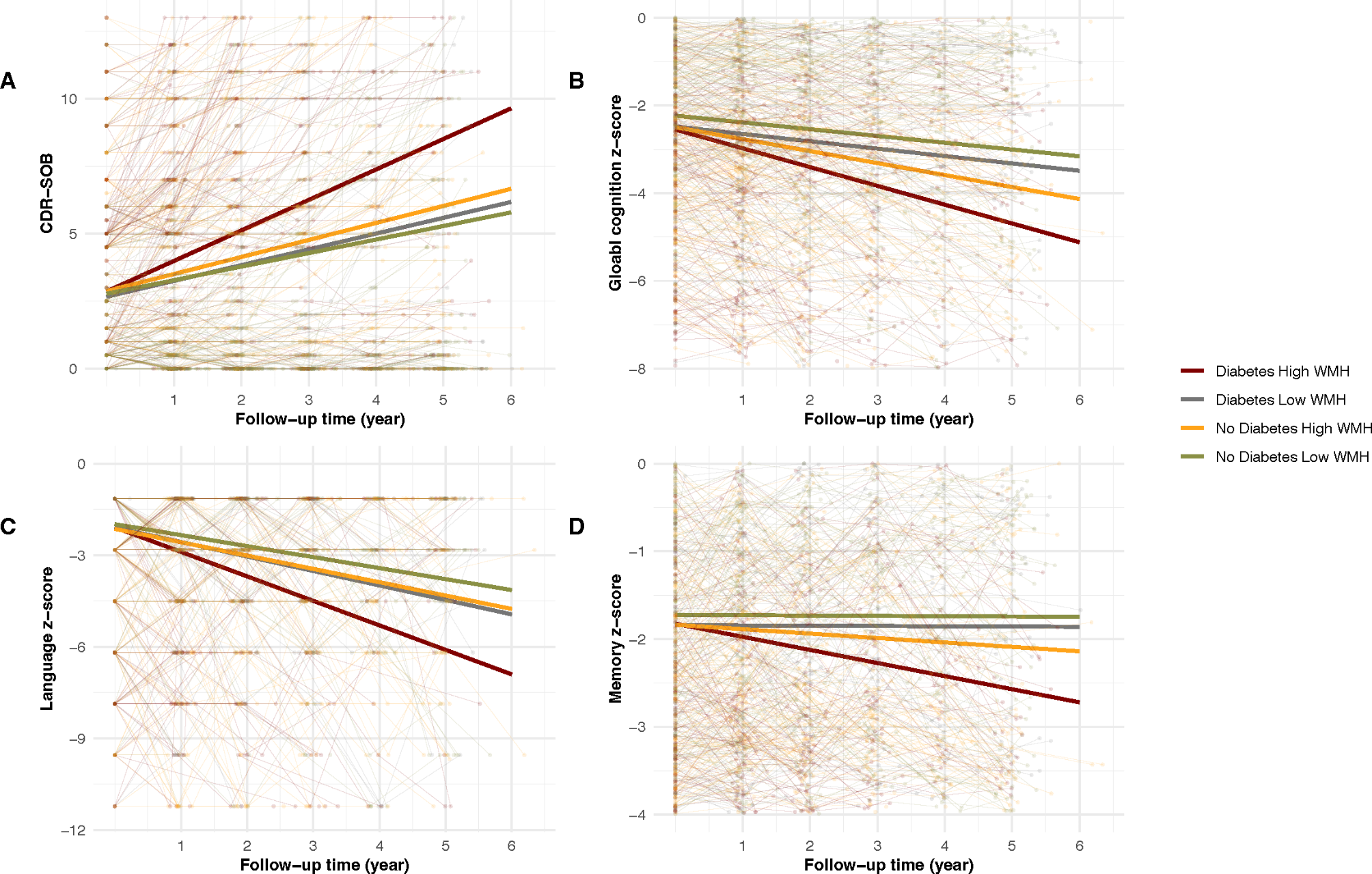
Next, generalized estimating equation (GEE) analysis was performed to investigate the independent effect of diabetes on cognitive decline by introducing 2-way interaction term (diabetes × time). Following this, we introduced 3-way interaction term (diabetes × CeVD marker × time) to examine the interactive effect of diabetes with each CeVD marker and total SVD burden on cognitive decline. Moreover, we used linear mixed-effects models as sensitivity analyses to account for random effects that could be induced by different study sites. In these analyses, log-transformed WMH volume was used as a continuous variable, while other CeVD markers were analyzed as count variables. Given the clinical relevance of the Fazekas scale in assessing WMH severity, an additional sensitivity analysis was conducted using a three-way interaction term (diabetes × Fazekas scale × time) to explore potential clinical implications. Statistical significance for 3-way interaction terms was established at p < 0.05. To account for multiple comparisons across 6 MRI markers of CeVD, we applied the Bonferroni correction, which resulted in a more stringent significance threshold of p < 0.0083 (0.05/6). If any significant interactive effects were found, incident CeVD score was adjusted to examine whether these interactive effects are independent of changes in CeVD markers. Binary CeVD markers were further used to better visualize these interactive effects. Specifically, WMHs were dichotomized into high versus low load, with high load WMHs defined as having a WMH volume ≥ 50th percentile of the study population in the main analysis and having Fazekas score ≥ 2 in the secondary analysis, whereas the remaining CeVD markers were dichotomized into presence versus absence. All models were firstly adjusted for age, gender, education, APOE genotype, study sites, hypertension, hyperlipidemia, current smoking, CVD, and baseline cognitive diagnosis. Considering the overlap between participants defined as diabetes and those who use glucose-lowering medication in our study, we adjusted for use of glucose-lowering medication in a separate model. Since existing evidence indicate that diabetes and stroke jointly lead to incident dementia, we repeated the same analyses for cognitive decline among stroke-free participants. If significant interactions between diabetes and CeVD were found, subgroup analyses were performed accordingly. Although p < 0.05 was considered statistically significant for group comparisons, Bonferroni-corrected significance cutoffs, p < 0.0083 (0.05/6), were used to address multiple tests across 6 cognitive subdomains when examining the association between diabetes and cognitive decline.
To explore whether Alzheimer pathology mediates any associations of diabetes with cognitive decline, we added blood-based Alzheimer biomarker and its interaction with time into the models where any subgroups demonstrated a significant effect of diabetes on cognitive decline. All models were adjusted for age, gender, education, APOE genotype, hypertension, hyperlipidemia, current smoking, CVD, and baseline cognitive diagnosis. We firstly utilized p-tau181 to maximize statistical power with a larger sample size (n = 476). Additionally, we performed a sensitivity analysis using the p-tau181/Aβ42 ratio (n = 448), as it has been shown to better reflect brain amyloid pathology in our previous study within this cohort [26].
Finally, we explored whether any significant interactive effect persisted among dementia-free participants with respect to global cognitive decline and incident dementia, using GEE models and Cox proportional hazards models, respectively. In the Cox proportional hazard model, we added 2-way interaction terms (diabetes × CeVD marker) to examine the interactive effect of diabetes and CeVD on incident dementia. All models were adjusted for age, gender, education, APOE genotype, hypertension, hyperlipidemia, current smoking, and CVD. Missing data for covariates were imputed via multiple imputations, using chained equations through the package “mice”. All p values presented were two-sided, and a value of p < 0.05 was considered statistically significant. All statistical analyses were performed with R (version 4.2.1).





留言 (0)