Survey to J-TRC webstudy participants
The J-TRC webstudy is an online registry designed to enroll preclinical AD subjects for preventative trial facilitation [20]. The details of the J-TRC webstudy have been described in our previous reports [18, 19]. Briefly, the J‐TRC study for preclinical and prodromal AD was launched in Japan in 2019 under a research license agreement with the Alzheimer's Therapeutic Research Institute. It has two main study components: the J-TRC webstudy and J-TRC onsite study. The J‐TRC webstudy (https://www.j-trc.org/), which is designed based on the APT Webstudy (https://www.aptwebstudy.org/) for Japanese cognitively normal elderly volunteer participants aged 50–85 years, is monitored by web‐based remote assessment of the cognitive function instrument (CFI) [21] and CogState [22] every 3 months. The J-TRC website is accessible only domestically within Japan. Within approximately 4 years since its launch, the J-TRC web study has recruited more than 10,000 eligible online participants from all over Japan. Individuals with an increased risk of elevated brain amyloid or cognitive decline are referred to the J‐TRC onsite study for detailed in‐person cognitive assessments, APOE genotyping, blood biomarker testing (e.g., plasma Aβ and p-tau), and determination of brain amyloid status by amyloid PET. The J‐TRC onsite study, which is designed based on the TRC‐PAD in‐person study in the United States, aims to build a large (n > 300) cohort of Japanese individuals with preclinical AD.
The procedure of our online survey is largely in accordance with our previous online survey conducted in June 2023 in terms of J-TRC website usability [23]. On September 25, 2023, we extracted the data of J-TRC webstudy participants eligible for this survey: those who had completed registration to the J-TRC website, given consent to participate in the study, and completed one or more CFI tests. Among them, 10,414 web study participants with valid e-mail addresses were included as eligible users to be sent an invitation e-mail containing the web address of the online questionnaire. E-mails were sent in the morning (6:00 am–7:00 am), only once per participant during the period between November 28 and December 2, 2023. The timing of this survey corresponds to the interval period between the full approval of lecanemab in Japan in September 2023 and the publication of the Optimal Clinical Use Guideline (OUG) of lecanemab in Japan on December 19, 2023. This means that at the time of the survey, questionnaire respondents had little idea about what kind of regulations might actually be in place for eligible patients and treatment facilities. No incentives (e.g., monetary gifts or lotteries) were provided to the questionnaire respondents. We have not sent thank-you mass e-mails with reminders.
An online questionnaire was administered using Google Forms provided in the Japanese language (https://www.google.com), without requiring personally identifiable information (e.g., name, account ID, e-mail address, or date of birth). It can be accessed via PCs, tablets, or smartphones. We used an anonymous method for collecting responses: we did not require respondents to log into their Google accounts to answer the Google Form questionnaire, nor did we require them to fill in their J-TRC webstudy accounts. This is because we wanted to gain as many responses as possible, even at the expense of respondents’ traceability. Consequently, we were unable to exclude potential duplicate responses from the same individual. However, to reduce double responses, we included a caution statement “Please respond to the questionnaire only once.” within the invitation e-mail.
Dropout analysis of the survey has been conducted and reported elsewhere [24], revealing significantly higher response rates among women (e.g., relative risk (RR) of response approximately 1.2 compared to men), lower response rates among non-retired individuals (RR approximately 0.8 compared to retired individuals), and lower response rates among younger individuals compared to older individuals.
Survey to specialist clinicians
Prior to our current online survey, with the cooperation of relevant academic societies, we had designed some of the questions in our survey in collaboration with other paper-based surveys on similar issues (i.e., perceptions of DMT treatment) that had been conducted in October and November 2023 with medical specialist clinicians in the field of dementia treatment or radiology. These surveys were led by one of our authors (T.A) and his colleagues as a special research project supported by the Ministry of Health, Labour, and Welfare. The cooperative design of questions was intended so that our results can be comparatively analyzed with the results obtained from specialists. Specialists certified by the Japan Society for Dementia Research (https://square.umin.ac.jp/dementia/) or the Japanese Psychogeriatric Society (http://www.rounen.org) were asked to answer the survey for specialists in dementia treatment, and specialists certified by the Japanese Society of Nuclear Medicine (https://jsnm.org) or members of The Japanese Society of Neuroradiology (https://neurorad.jp) were asked to answer the survey for specialists in radiology.
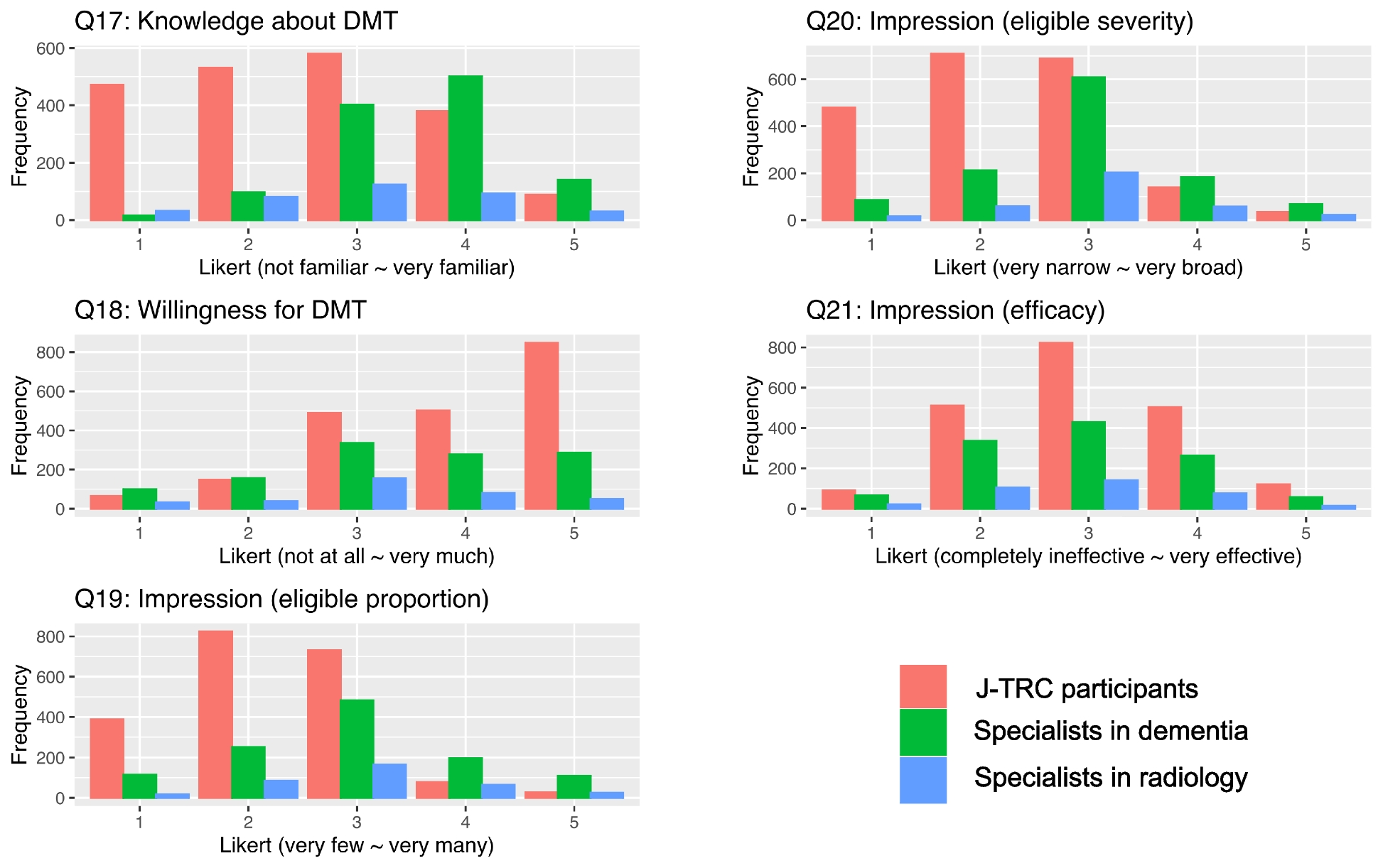
The commonly-designed questions are shown in Table 1: self-evaluated knowledge about DMT (Q17), willingness to receive DMT treatment (Q18), impressions about the range of DMT eligibility (Q19, Q20), impression about the efficacy of DMT (Q21), impressions about blood based biomarkers (e.g., plasma Aβ) (Q28), and perceptions about prioritizing treatment (Q41-Q45).
Table 1 Commonly designed questionnaire contents across surveys to J-TRC users and specialistsThe survey of dementia treatment specialists gathered n = 1,157 eligible responses, and the survey of radiology specialists had gathered n = 361 eligible responses. We obtained result data of answers to the commonly-designed questions, and used them for comparative analysis with our survey results. Dropout analysis of the surveys of specialists was not conducted because we have not obtained individual specialists’ personal background information (e.g., age and sex).
Questionnaire
The questionnaire was made up of 55 questions in total following the background explanations for each topic, over 19 pages written in Japanese, requiring approximately 30–40 min to complete. The English-translated version of questionnaire explanations, questions, and answer choices are provided in Additional file 1. Questions are composed of those about the respondents’ attributes (Q1-Q16, Q33, Q55), and those about the respondents’ perceptions of DMT drugs or related affairs (Q17-Q32, Q34-Q54). Among these 55 questions, 22 are mandatory to answer. The majority of the questions required the selection of only one answer choice that best applied, but for some questions respondents were asked to select multiple answers that applied.
Questions Q41-Q45 are about prioritizing treatment. The question Q41 is “As mentioned above, it may not be possible to provide treatment to everyone who need it for various reasons such as insufficient preparedness of healthcare systems or financial issues. What do you think about prioritizing or limiting the treatment based on certain criteria?”, and the questions Q42-Q45 are modified versions of Q41 from specific points of view. The question Q41 asks about the pros and cons in general terms for prioritizing DMT treatment by service providers (i.e., medical facilities or doctors) or by patients. This question assumes a hypothetical case of practical shortcomings in the preparedness for DMT treatment, asking whether it is acceptable to prioritize service providers (i.e., facilities and doctors) who should administer DMT treatment (“acceptable for prioritization of facilities”), and whether it is acceptable to prioritize patients who should receive DMT treatment (“acceptable for prioritization of patients”). Prior to this question, detailed explanations about the background circumstances as to why resource shortcomings in DMT treatment may occur are shown in the questionnaire page.
The modified questions Q42-Q45 focus on specific point of view (unlike in general terms in Q41) in considering the pros and cons of prioritization: medical rationale (Q42), health economic perspectives (Q43), impact on patients’ lives (Q44), and addressing socially vulnerable people (Q45). These questions do not include specific examples of the assumed settings, and they simply ask respondents’ impressions of pros/cons of prioritization in terms of these points of view. In general, it has been widely observed in clinical practice to limit eligible patients or facilities for some specialized treatments based on the safety and efficacy of the treatments, such as in the form of practice guidelines. This is also true in the case of lecanemab treatment, since AUR [4] and OUG [13] for lecanemab require that eligible patients have an MMSE score of 22 or more and a CDR-GS score of 0.5 or 1 at baseline. Such criteria exclude non-eligible patients from the ranking of referrals for treatment, which means that “patient prioritization from medical rationale” (Q42) has been in some ways accepted to varying degrees. Thus, we set Q42 as a reference to measure the degree of acceptance toward prioritization in other similar questions (Q43-45).
Statistical analysis
Data acquisition period was determined as four weeks from the day of invitation e-mail sending. All data preprocessing and analyses were conducted using R software. First, answers to questions for J-TRC webstudy participants are summarized: numerical variables and Likert scale answers are summarized using median and interquartile range (IQR), and categorical variables are summarized using frequency and proportion (%).
Second, we analyzed Likert scale results (scales: 1–5) on the impression about DMT drugs (Q17-Q21) for integrated data comprised of J-TRC participant survey and specialist surveys. For each scale score in Q17-Q21, we conducted linear regression analysis using the following equation:
where \(_\) is the intercept and \(Data\) is the survey group of participants (i.e., J-TRC webstudy participants, specialists in dementia treatment, and specialists in radiology). In this model, \(_\) is the coefficient we want to obtain in order to understand the difference in the responses among the examined data groups.
Third, we analyzed perceptions regarding the prioritization of treatment (Q42-Q45), using data from the J-TRC participant survey and specialist surveys. Responses to Q42-Q45 were bifurcated into a binary variable indicating acceptance towards prioritizing patients receiving DMT treatment (e.g., choices [c] and [d] for “yes”, and choices [a] and [b] for “no” towards it), or acceptance towards prioritizing facilities administering DMT treatment (e.g., choices [b] and [d] for “yes”, and choices [a] and [c] for “no” towards it). These question answers to Q42-Q45 were collapsed into a single variable that represents a set of (four) repeated measures for each survey respondent, and we conducted mixed logistic regression analysis on the target binary variable (i.e., “acceptance towards prioritization of patients (or facilities)”) based on the following equations, which allowed us to account for within-participants variability:
Model (B-1): \(log\left(_\right)=_+Focus \cdot _+Respondent ID \cdot _\)
Model (B-2): \(log\left(_\right)=_+Focus \cdot _+Age \cdot _+Sex \cdot _+Education \cdot _+Living \cdot _+Retired \cdot _+Family \cdot _+Respondent ID \cdot _\)
Model (C): \(log\left(_\right)=_+Focus \cdot _+Respondent ID \cdot _\)
In the equations above, Data is the survey group of participants (i.e., J-TRC participants, specialists in dementia treatment, and specialists in radiology). The target variable in the above models is the acceptance towards prioritizing patients (yes/no, in model [B]) or facilities (yes/no, in model [C]). \(_\) represents the fixed intercept, Focus is a categorical variable on the specified point of focus (i.e., Q43-Q45) with the Q42 response as a reference, and \(_\) denotes a random intercept by the respondent [25]. Model (B-2) was only applied to J-TRC participant data. The variable \(Age\) represents the respondent’s age in decades, Sex denotes whether the respondent is female, \(Education\) indicates additional education years after graduating from high school (e.g., 0 indicates graduation from high school), \(Living\) refers to the respondent’s living arrangement (i.e., living alone or not), \(Retired\) denotes whether the respondent is currently retired or not, and \(Family\) means whether the respondent has any family history of dementia or AD. \(_\) is the coefficient we want to obtain. The obtained \(exp\left(\beta \right)\) corresponds to the adjusted odds ratio (OR). When the lower 95% confidence interval (CI) of OR is higher than 1, it is considered significantly high. The mixed logistic regression was performed using R package [26]. Some questions, including Q41-Q45, were not mandatory to answer, leading to missing values in the analysis: for the analysis with models (B) and (C), a listwise method was used to deal with the missing values.
Ethics
The J-TRC webstudy was approved by the University of Tokyo Graduate School of Medicine Institutional Ethics Committee (ID:2019132NI-(3)), and online informed consent was obtained from individual participants upon registration. The online survey was also approved by the local ethics committee.





留言 (0)