
記住我

The SR protocol followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocol (PRISMA-P) guidelines (Additional file II). The protocol has registered in the PROSPERO (CRD42024507187).
Review questionThis systematic review aims to explore the review question: “What are the patients’ experiences of being mechanically ventilated in ICUs in LLMICs?”.
FINER criteria (feasible, interesting, novel, ethical and relevant), as recommended by the Cochrane Handbook for Systematic Reviews (CHSR), were referred to while formulating the review question [18]. A preliminary scoping search from 15 to 25 October 2023 helped refine the review question. The scoping search helped establish the feasibility in terms of availability of evidence by identifying six relevant studies addressing the review question and novelty by lack of similar existing or ongoing SRs. A research priority-setting meeting among the concerned stakeholders (administrators, intensivists, ICU survivors and their families) established that the review topic is interesting, ethical and relevant [18].
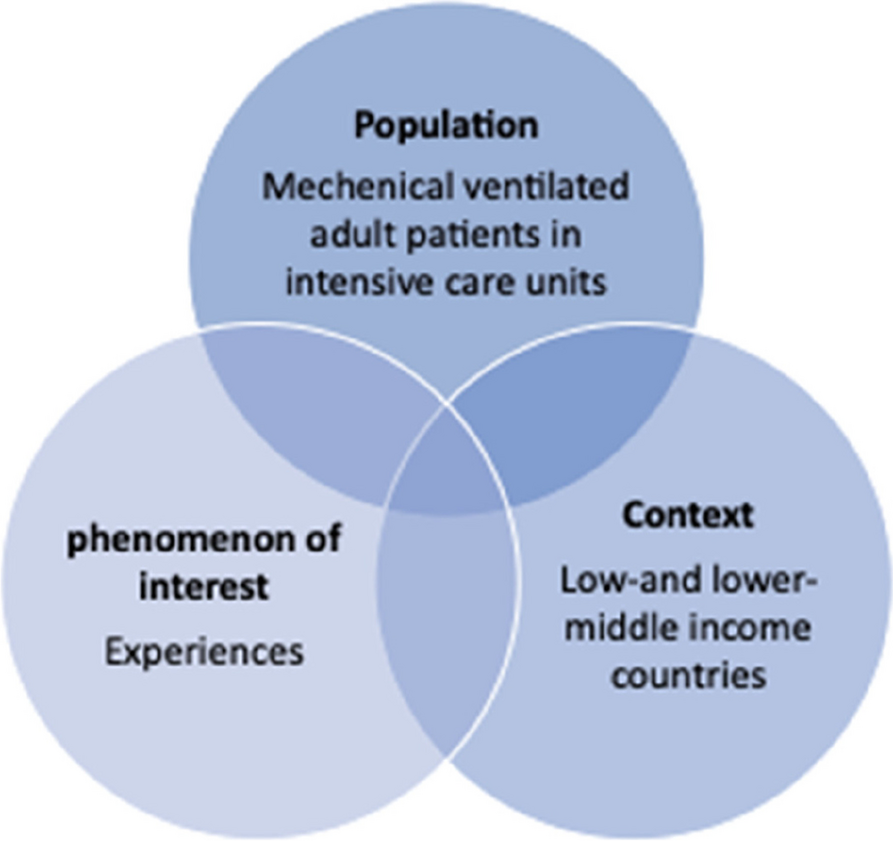
Eligibility criteriaExperiential reviews (focussing on experiences and perspectives) such as ours usually lack a comparator and outcome, making the traditional PICO framework not the best fit for such reviews [19]. PICO framework, as recommended by the Joanna Briggs Institute (JBI), translated our review question into key concepts (Fig. 1) [20].
Fig. 1
Key concepts guiding the eligibility criteria and search strategy
Study selection will be based on pre-defined inclusion and exclusion criteria (Table 1).
Table 1 Eligibility criteriaPopulationThe population of interest is adult (≥ 18 years) patients undergoing MV (both invasive and non-invasive) in ICUs. ICU settings will include medical ICU, surgical ICU, mixed medical-surgical ICU, neuro ICU, critical care, respiratory care, cardiac coronary and high dependency units. We will exclude studies of MV in home settings and hospital wards or settings other than ICUs. Studies with a mix of settings without data provided separately for patients undergoing MV in ICUs will be excluded.
Phenomenon of interestStudies exploring patients’ experiences of MV in ICUs. No restriction on the duration of MV or time limit on the collection of patients’ experiences after MV will be imposed. Studies exploring experiences of paediatric (< 18 years), non-patient population (caregivers, family members, healthcare professionals) or a mix of populations will be excluded.
ContextStudies set in low- and lower-middle-income countries as classified by the World Bank Country and Lending Groups (2024) [17]. We will exclude studies exploring experiences of patients from LLMIC residing and admitted in ICUs in upper-middle-income countries (UMICs) or HICs (e.g. Indians residing and mechanically ventilated in ICUs in the UK). Studies with a mix of population from LLMIC, UMIC and/or HIC without data provided for patients from LLMIC will be excluded. Additional file III outlines the operation definitions for key concepts adopted in this review.
Study designsWe will include empirical peer-reviewed literature exploring adult patients’ experience of undergoing MV in ICUs published since database inception to present. No restriction on study design will be imposed, and SR will include quantitative, qualitative and mixed-methods studies. We will exclude opinion and other nonempirical papers, conference abstracts and grey literature. Evidence synthesis will be excluded. However, reference lists of relevant SRs will be screened to identify any additional articles missed during database searching.
Information sourcesWe will search the following electronic databases: MEDLINE (Ovid), Embase (Ovid) and PsycINFO (Ovid), Cumulative Index to Nursing and Allied Health Literature (CINAHL, EBSCOhost platform), Scopus (http://www.scopus.com), Web of Science (Clarivate) and Cochrane Library (https://www.cochranelibrary.com).
To ensure literature saturation, we will manually scan reference lists of included studies and relevant evidence syntheses to identify additional studies [21]. Articles citing the included studies will be searched using Google Scholar to identify additional studies. Reference list screening and citation tracking will continue until data saturation, defined as no new relevant study being identified, an indicator for stopping further literature search [22]. In addition, PubMed’s related article search on all the included studies will be performed to reduce the likelihood of missing relevant studies.
Search strategyEfforts will be made to ensure that the literature search is transparent, comprehensive, robust and reproducible, with the aim to identify all the relevant reports [18, 20]. An initial scoping search of PubMed will be performed to identify free text words used to describe the key concepts. The search strategy will be developed iteratively with input from all the reviewers, going through and adapting from relevant SRs and going through the title, abstracts, thesaurus terms used to index and keywords used by the authors of the relevant articles. With the aim to comprehensively search the literature and identify the maximum relevant literature, text words will be combined with the MeSH terms in a “belt and braces” approach, and the latter will be exploded to increase the sensitivity of the search [22]. The database-specific thesaurus and free text words for a similar concept will be combined using the Boolean operator “OR” to formulate search strings for each individual concept. The search strings for individual concepts will be nested and combined with those for different concepts using the Boolean operator AND. A version control and an audit trail of all the iterations and changes made in the search strategy will be maintained.
The search strategy will be first devised for PubMed and CINAHL and sent to an experienced systematic reviewer and a subject expert for peer review. The final search strategy will be adapted for other electronic databases. No study design, date or language restrictions will be imposed on the search. However, only articles published in the English language will be included. Another experienced researcher will rerun the search strategies to rule out any syntax or other errors. An explicit, detailed and transparent reporting of search strategies (including database name, search platform, date run and corresponding number of hits) will be done. A draft PubMed search strategy is presented in Additional file IV.
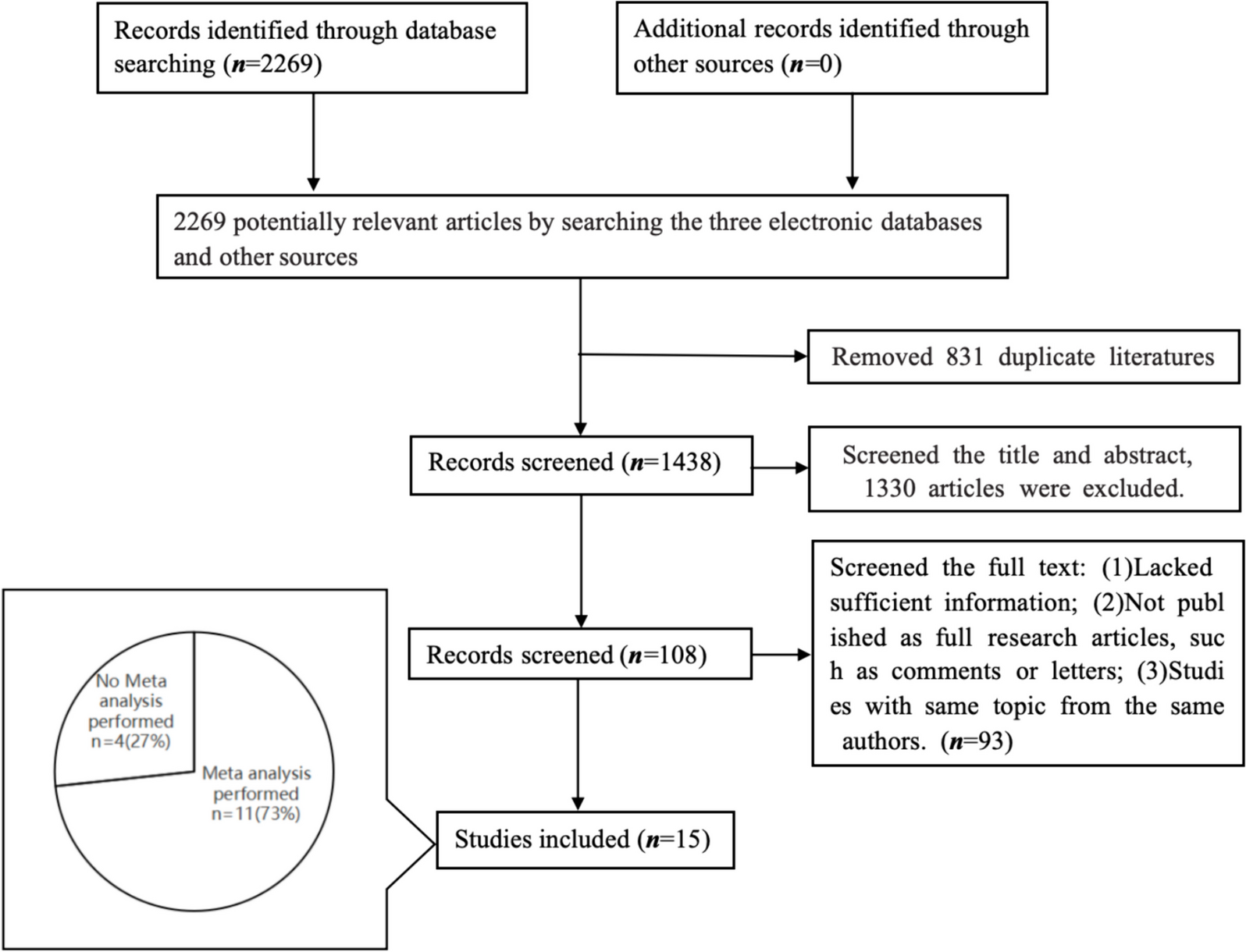
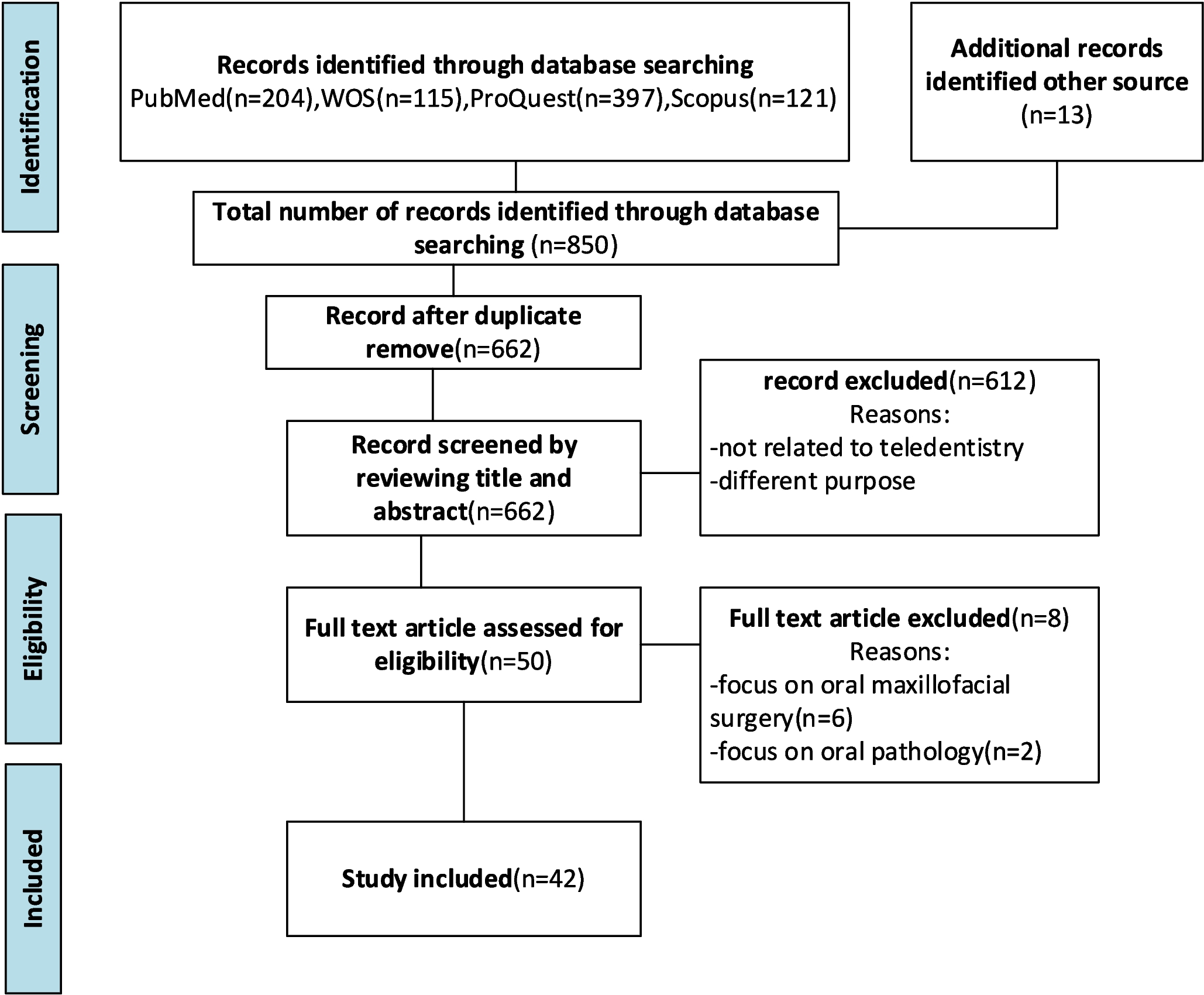
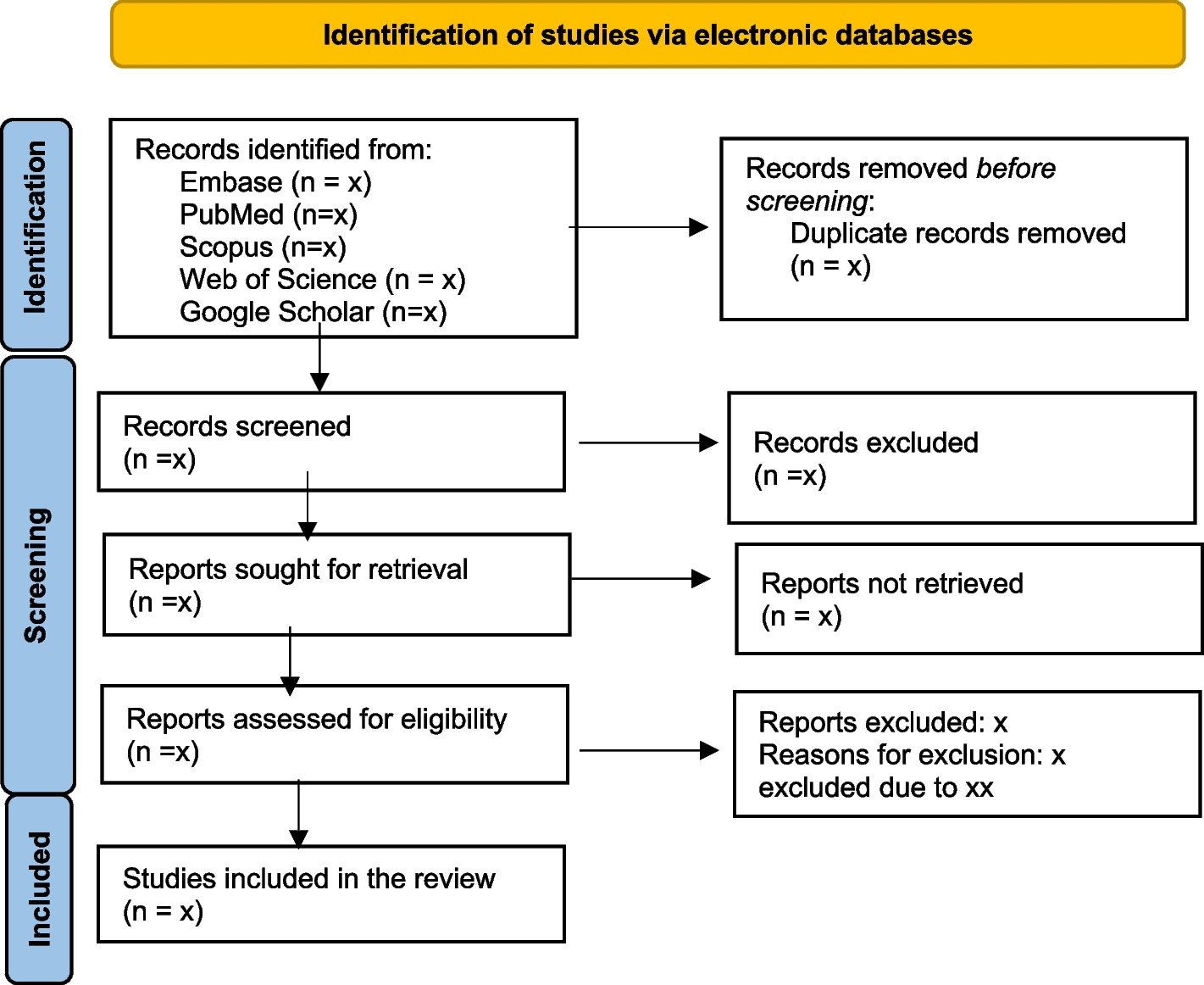
Data management and selection processAll records identified will be transported to EndNote reference manager software (V.20, Clarivate Analytics, Philadelphia, PA, USA), and duplicate entries will be removed. Deduplicated references will be exported to Rayyan (https://www.rayyan.ai/) in which two researchers will independently screen the title and abstracts to identify records that meet the inclusion criteria [23]. Full-text articles of potentially eligible records and those where eligibility could not be determined from the title and abstract will be retrieved and screened for inclusion by two independent reviewers. The final consensus will be made by referring to the a priori-specified eligibility criteria and whether the article answers the review question or not. Disagreements will be resolved through discussion between the two reviewers and arbitrated by a third reviewer where necessary. The search and selection process results, including the number of records excluded at each step and reasons for exclusion, will be reported in a PRISMA flow diagram (Additional file V).
The inter-rater reliability (IRR) among the reviewers will be calculated using percent agreement and Cohen’s kappa [24, 25]. Percentage agreement does not consider chance agreement among coders and hence has been discouraged as the sole indicator of IRR [26]. In that respect, Cohen’s k, by estimating and removing chance agreement, represents a chance-corrected measure of IRR [27].
Data collectionData extraction form and data itemsAn Excel data extraction form customized to meet the review aim, objectives, purpose and typology of studies identified during the scoping search will be developed, discussed and revised in consultation with all the researchers to avoid missing relevant data. Extracted data will include information on bibliographic details; study aims/objectives, participant characteristics, context and setting; study methods; data collection (including the timing of data collection) and analysis; and ethical issues, study findings and direct quotations from study participants to contextualize the authors’ interpretation of findings and to support our synthesized themes and subthemes (where appropriate).
PilotingThe data extraction form will be piloted in five studies to ensure that the data extraction form captures all the relevant information consistent with the research question and purpose [18]. The piloting will be done independently by two researchers, after which necessary changes will be made in agreement. Repiloting of data extraction form will be done to ensure that it is comprehensive and specific to our review purpose [28].
Data extraction by two independent researchersTo ensure rigour and minimize bias, two reviewers will do data extraction independently in parallel [18, 29]. Prior to data extraction, the two researchers will discuss in detail the instructions for data extraction and coding [18, 28]. Any discrepancies will be reconciled through discussions. An audit trail of disagreements and resolutions made will be maintained.
Outcomes and prioritizationThe primary outcome of interest will be patients’ experiences defined as patients’ self-report of their views, attitudes, perspectives, opinions, perceptions, difficulties, acceptance and satisfaction while undergoing a health procedure (MV) shaped by healthcare people, processes, physical settings and their expectations of healthcare [29]. Patients’ experiences will also include their self-report of emotions and physical (e.g. pain, thirst) and psychological (stress, distress, anxiety) factors while undergoing MV in ICUs. Apart from the outcome data, non-outcome data will be extracted to contextualize the findings of primary studies and assess their trustworthiness, applicability and transferability to other settings [28].
Critical appraisalCritical appraisal refers to appraising quality of studies for methodological rigor, trustworthiness, sources of bias and validity and reliability of their findings [30, 31]. Critical appraisal tools provide a stepwise and structured approach to systematically appraise the eligible studies and uncover their methodological limitations [32]. The choice of critical appraisal tool is influenced by the ease of use, brevity, the context in which it developed, availability (free or fee based) and research question, which in turn determine the typology of included studies, available expertise and resources [33]. Without clear-cut consensus, Noyes et al. recommend using a validated tool to assess the methodological strengths and limitations of the included studies [34].
Mixed-Methods Appraisal Tool (MMAT) will be used to assess the methodological rigour and risk of bias in included studies [35]. MMAT was found as the best fit as it has been specifically designed and used extensively to appraise different typology of studies (qualitative, quantitative and mixed methods) as identified during our scoping search, structured format, easy accessibility, ease of use, brevity and detailed guidance available for its use (Additional file VI) [36, 37]. MMAT was developed through a rigorous development process comprising of literature review, e-Delphi and researchers inputs and has been shown to be comprehensive, valid, reliable and feasible [35, 36].
The initial two screening questions of MMAT will ensure that the study being appraised is an empirical study and, hence, eligible for inclusion in this SR [35]. Each study will be appraised by using one of the five study-design-specific categories (qualitative, quantitative randomized controlled trial, quantitative non-randomized, quantitative descriptive and mixed methods) of questions provided in the MMAT. For each question in the study-design appropriate category, each study will be rated as yes (*quality criteria met), no (study does not satisfy the criterion) or can’t tell (lack of sufficient information to answer). Although initially recommended against [35], Hong et al. later reported a method to calculate the overall quality score of a study (Table 2) [38]. As per the recommendations, the overall quality score for mixed-methods studies will be the lowest score of the study components (quantitative, qualitative and mixed methods) [38].
Table 2 Overall quality score of each included studyTwo reviewers will do a critical appraisal independently, and discrepancies will be settled with consensus [35]. Critical appraisal involves judgment making necessitating two independent appraisers having experience in the domain assessed [35]. The MMAT will first be piloted independently by both reviewers on five studies of different study designs to ensure consistent application [18]. An audit trail of all the disputes and resolutions made will be maintained. To be more informative, both overall quality scores along with a detailed description will be provided [38].
No studies will be excluded based on critical appraisal. Exclusion of studies based upon quality appraisal may adversely impact the evidence synthesis by excluding methodologically less robust but important descriptive findings and excluding fewer studies available on the phenomenon of interest, which has been advised against [18, 33, 34, 39, 40]. However, depending on the quality appraisal results, we might do a sensitivity analysis to assess the impact of study quality on the SR findings [37].
Data synthesisThe findings of this review will be synthesized using Popay’s narrative synthesis [41]. Narrative synthesis is a well-recognized and recommended form of data synthesis, portraying findings as a trustworthy story. Popay’s narrative synthesis was chosen as it (1) allows the synthesis of quantitative results with qualitative findings from diverse study designs, thereby allowing comprehensive understanding and answering of the review question; (2) aims to adopt the same rigorous, systematic, transparent and non-bias approach to narrative synthesis as employed at other steps of a SR; (3) can be used for data synthesis for reviews addressing review questions as varied as effectiveness, implementation, needs and preferences; (4) has been successfully used as the synthesis method in a number of MMSRs (as reflected by 4833 citations on Google Scholar on 08 February 2024); and (5) synthesized findings can be and have been used to inform policy and practice: one of the penultimate goal of conducting a SR [41]. Rather than prescriptive guidance, Popay’s framework comprises of a number of steps (rather than stages) with an array of tools and techniques which can be utilized at each step [41]. Popay’s approach to narrative synthesis is iterative without the need to carry out steps in the same sequence as described [41]. This allows the flexibility needed to address the review type and study characteristics without compromising transparency and rigor [41].
Developing preliminary synthesisFirst of all, a brief textual description of each study detailing its aims, design, setting, participants, findings and limitations will be developed to familiarize with and contextualize the study findings. These study characteristics will be tabulated to identify patterns across the studies. This will form the basis for grouping studies on the basis of study designs and context, for example.
Considering the review question can be answered by both qualitative (phenomenological studies exploring patients’ experiences) and quantitative (cross-sectional surveys) study designs, a convergent integrated with a data-based convergent approach to data synthesis will be used [18, 42]. Data transformation in the form of qualitization of the quantitative results will be done [42]. Data transformation allows data transformation into mutually compatible and synthesizable formats, with qualitization (extracting survey questions as themes or textual narratives) being less prone than and recommended over quantization (converting qualitative findings into words or frequencies) [42]. The extracted findings will then be analysed thematically. Line-by-line coding of the extracted findings will be done. The process will be iterative without any a priori codes or categories.
Exploring relationship within and across studiesTabulation and grouping during the preliminary synthesis will help to explore relationships and patterns across studies. Heterogeneity in terms of population, duration of MV, timing of data collection after MV, context and methodology will be explored during this step. Idea webbing or concept mapping will be used to group conceptually similar codes into categories and explore relationships between the categories.
Data translation: thematic synthesisTranslation refers to identifying similar concepts expressed differently in different studies [37]. Though devised initially for qualitative studies, thematic analysis allows the translation of data from diverse study designs [41]. Meaningful subthemes and themes will be generated to understand patients’ experiences of MV in ICUs and the factors moderating these experiences. The aim of synthesized findings will be to allow an interpretative understanding of the current state of knowledge on the concept rather than just mere aggregation of the data [41, 43]. An iterative process will be followed wherein the themes and subthemes will be reviewed and refined in consultation with reviewers with previous experience in doing narrative synthesis. The SR findings will be presented as themes, subthemes and their explanatory narratives.
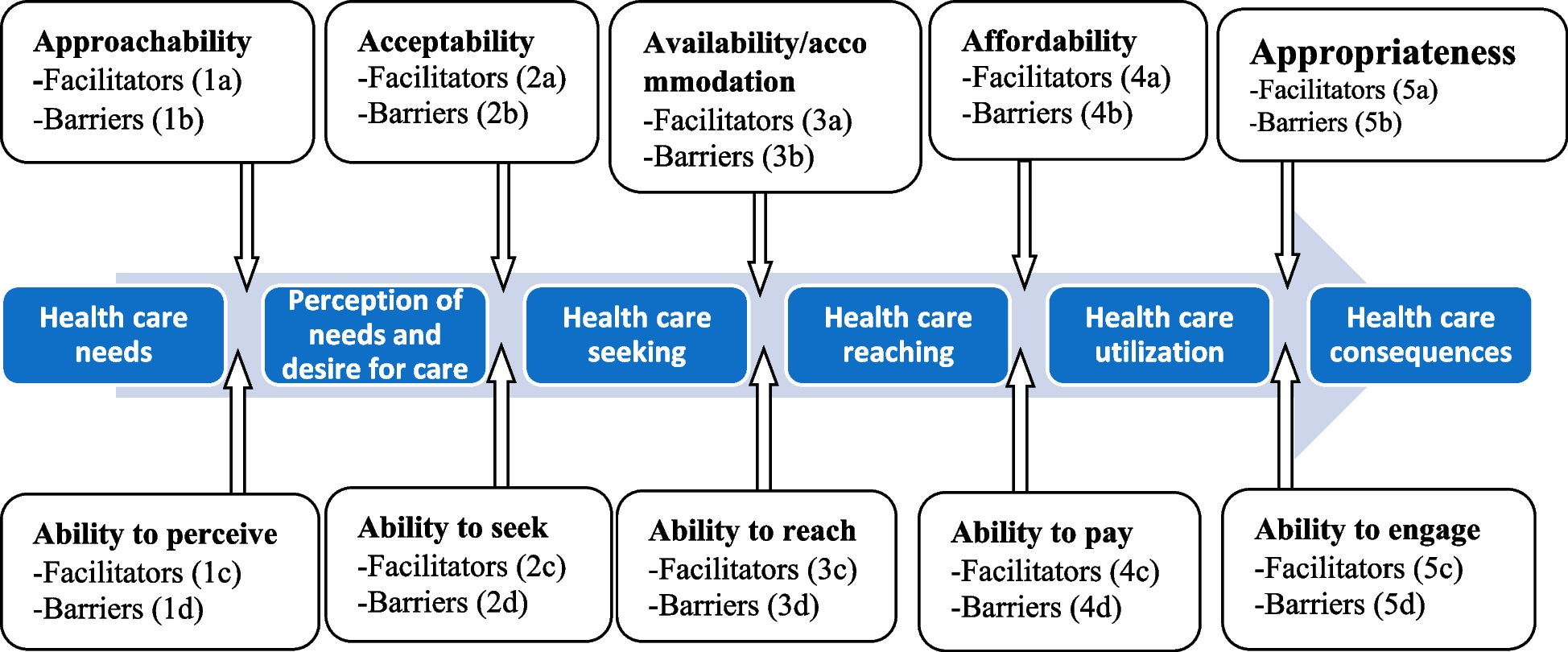
Theoretical framework to interpret the review findingsPopay suggested using theory to inform the review question and interpret the review findings [41]. Although an element of Popay’s framework, it is not mandatory to use theory [41]. PICO framework informed our review question, negating the need for theory at this stage. By linking, organizing and summarizing information, theories help make sense of the synthesized findings and provide a framework to facilitate understanding a complex phenomenon [44]. Depending upon the review findings, the theory may be used to facilitate the interpretation of review findings. This will allow an inductive approach to data analysis without any a priori categories.
Assessing the robustness of the synthesisThe findings of a SR are as trustworthy as the quality of the included studies [41]. The synthesis findings will be critically reflected upon its limitations, implications and studies (their methodological quality, sources of bias and concordance with the review’s aims) informing the review. Sensitivity analysis will be done to assess the impact of including studies of differing quality and studies employing different study designs (quantitative, qualitative and mixed method) on the synthesis findings [40]. To assess the impact of applying critical appraisal on the synthesis findings, we will calculate a quality score for each included study by dividing the number of quality criteria met (yes) by the total quality criteria possible [45]. A sensitivity analysis will be performed wherein it will be assessed whether the exclusion of weak quality studies (i.e. studies with a quality score of ≤ 0.5) impacts the depth, richness or complexity of the synthesis findings [
留言 (0)