
記住我
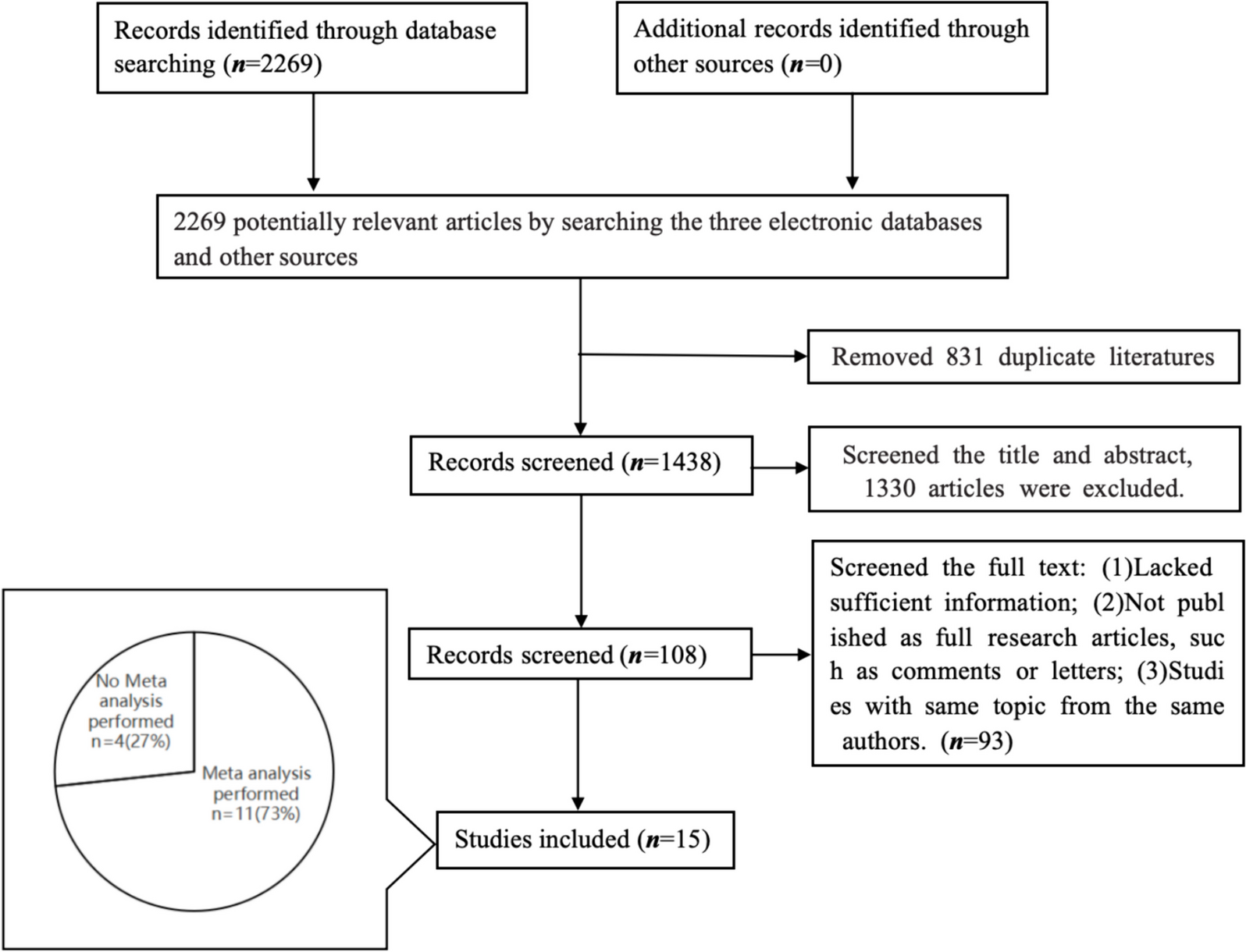
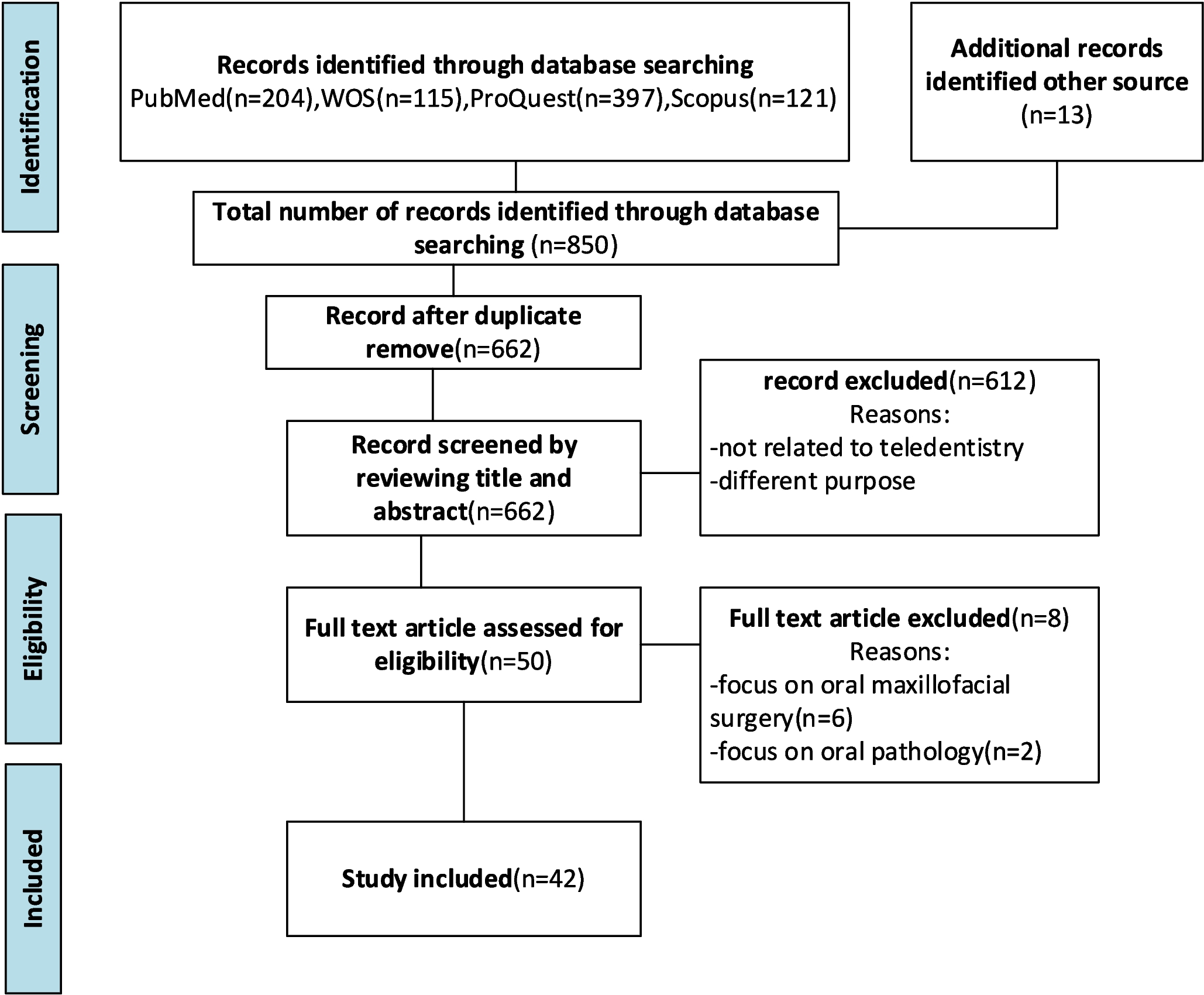
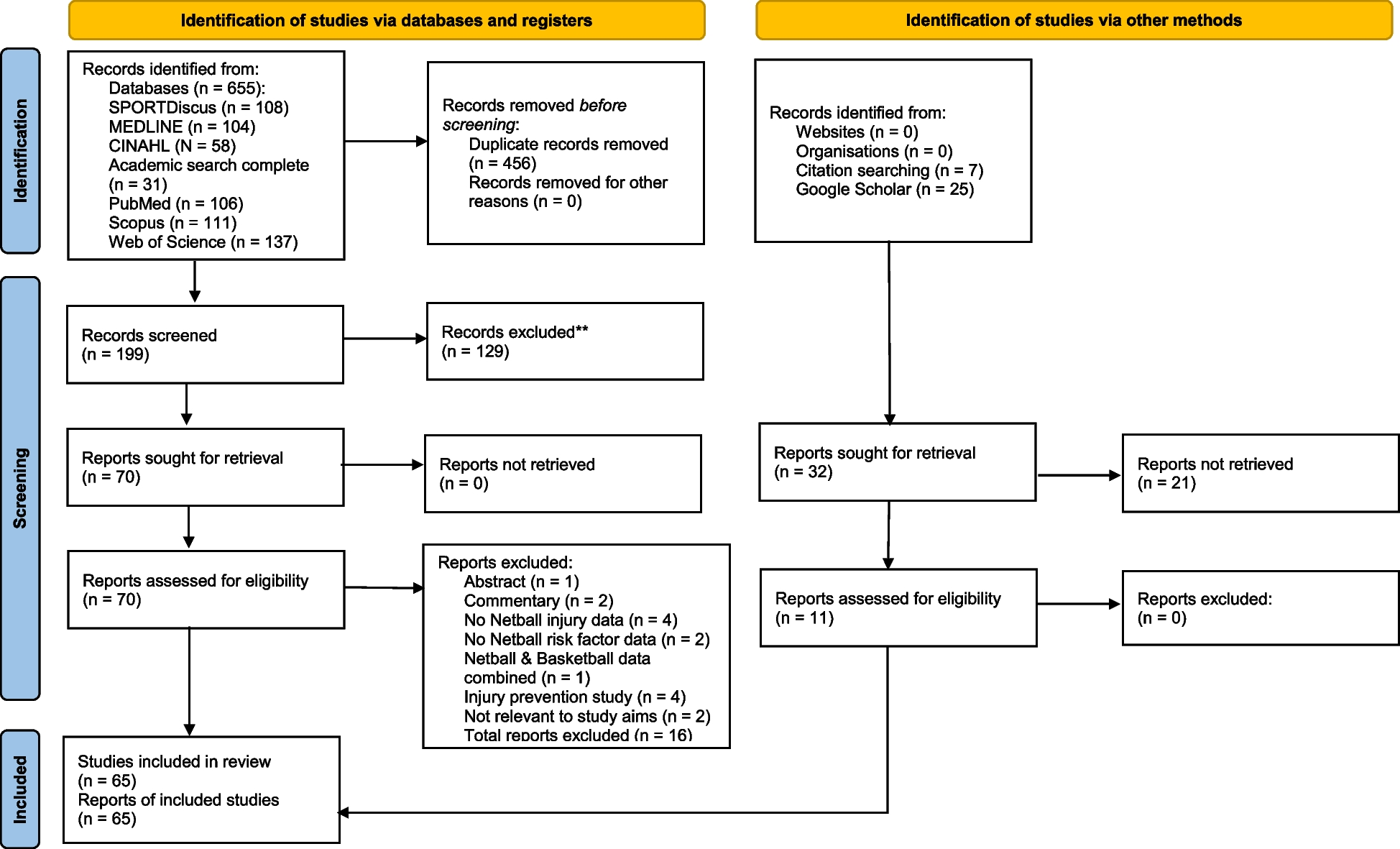

On September 5th, 2022, 18, 30, and 42 articles were retrieved from the three databases of PubMed, EMBASE, Web of Science, and Cochrane Library, respectively. Of the total of 90 articles, 34 were duplicated records, and 17 articles that were only registered in the study protocol or ongoing clinical trials were excluded. Remained 39 articles were screened and 24 were excluded by confirming the abstract. Fifteen articles were retrieved and 10 were assessed for eligibility (Table 1). One abstract that was difficult to determine whether it is randomized controlled [17] and four abstracts that can be replaced with full-text articles were excluded. In addition to database searching, 3 articles were found as a result of the search through the citation of the previous studies, and one (MacAllister’s full-text article of the REPAIR study) could be added by excluding two that were not RCT. However, the abstract of the REPAIR study [18] was excluded as a duplicate of the newly included full-text article. Among the studies, Nielsen’s article was a 1-year follow-up report of Krogstrup’s CONTEXT study, and Veighey’s article was a long-term outcome of MacAllister’s REPAIR study. Finally, 8 studies and 10 reports were included. This can be confirmed in the PRISMA 2020 flow diagram in Additional file 3. Table 1 summarizes the characteristics of the included articles. From this paragraph on, all included studies were not mentioned in citation lists.
Table 1 Characteristics of included studiesMortality, which is the primary endpoint, was confirmed in 4 articles (MacAllister, Nicholson, Nielsen, Veighey). Among the outcomes to evaluate kidney graft function, DGF was extracted in 5 articles (Kim, Krogstrup, MacAllister, Nicholson, Wu), and graft rejection was confirmed in 3 articles (Bang, MacAllister, Nielsen). Among the laboratory results, 3 articles reported tCr50 as a continuous variable (Bang, Kim, Krogstrup), which other 3 articles recorded the number of patients with tCr50 achieved within 24 h (Kim, MacAllister, Nicholson). eGFR at 12 months after transplantation was extracted the results from 4 articles (Bang, Kim, MacAllister, Nielsen).
The risk of bias results finally determined by the corresponding author are shown in Fig. 1. Figure 1A is the risk of bias for finally-reported mortality, which is the primary outcome. Figure 1B, C shows a risk of bias assessments for secondary outcomes, delayed graft function, and acute rejection, respectively. The risk of bias evaluated by two independent researchers showed an 80% concordance rate, and None of the risk of bias assessments reported contradictory results, with one researcher assigning a low risk while the other assigning a high risk for the same item. Two studies that were not full-text articles did not evaluate the risk of bias (Bongu, Chen). Two out of 8 full-text articles were at high risk (Krogstrup, Wu). Four were low risk of bias (Bang, Kim, MacAllister, Veighey). Publication bias could not be evaluated because of few included studies.
Fig. 1
Assessment of the risk of bias by the Cochrane risk of bias tool (RoB 2). RoB was evaluated for three outcomes: A the mortality finally reported, B the incidence of delayed graft function, and C graft rejection within 12 months posttransplant
Effect of RICPrimary endpoint (Fig. 2)Fig. 2
Forest plots evaluating the primary outcomes of remote ischemic conditioning for patients who underwent kidney transplantation. Each plot shows the effect on mortality at 3 and 12 months after transplantation and finally reported mortality
Mortality of patients within 3 months of transplantation was reported in 302 patients in two studies (Nicholson, Nielsen). However, since no death occurred in Nicholson's study, it could not be synthesized into the outcome. 1 out of 249 in the RIC group and 0 out of 153 in the sham group died within 3 months, and there was no significant difference in mortality (RR, 3.11; 95% CI, 0.13–75.51, P = 0.49).
Mortality of patients within 12 months of transplantation was reported in 628 patients in two studies (MacAllister, Nielsen). Three out of 416 patients in the RIC group and 3 out of 212 in the Sham group died, and the mortality rates were not significantly different (RR, 0.70; 95% CI, 0.14–3.45, P = 0.67). Heterogeneity was low (I2 = 0%).
The mortality finally reported in the included studies could be found in four articles (MacAllister, Nicholson, Nielsen, Veighey). Since the follow-up study of MacAllister’s report was Veighey’s report, only Veighey’s results were used. Fourteen out of 456 in the RIC group and 11 out of 252 in the sham group died. There was no significant difference between the two groups, but clinically, the mortality rate was reduced by half in the RIC group (RR, 0.49; 95% CI, 0.21–1.11, P = 0.09). Heterogeneity was low (I2 = 0%).
Among the mortality rates collected at the three time periods, short-term mortality (3-month post-transplant mortality) tended to increase in the RIC group, but mid- to long-term mortality (12-month post-transplant, or the latest reported mortality) was higher in the sham group than in the RIC group.
Secondary endpoint (Fig. 3)Fig. 3
Forest plots evaluating the secondary outcomes of remote ischemic conditioning for patients who underwent kidney transplantation. Each plot shows the incidence of delayed graft function (A), the incidence of graft rejection within 12 months (B), the time required for a 50% decrease in baseline serum creatinine concentration [tCr50, hours] (C), the incidence of tCr50 less than 24 h (D), and eGFR at postoperative 12 months [ml/minute/1.73 m.2] (E)
DGF occurred in 103 of a total of 1027 patients. It occurred in 50 out of 624 patients in the RIC group and 53 out of 403 in the sham group. Although the incidence was less in the RIC group, there was no significant difference (RR, 0.64; 95% CI, 0.30–1.35, P = 0.24). It showed low heterogeneity (I2 = 31%). Graft rejection within posttransplant 12 months occurred in 88 of 796 patients. There were 58 of 501 in the RIC group and 30 of 295 in the sham group, and there was no difference between the two groups (RR, 1.13; 95% CI, 0.73–1.73, P = 0.59) (Fig. 3B). Heterogeneity was very low.
Of the 440 patients in whom tCr50 could be confirmed, it took 29.0 h for 219 patients in the RIC group and 26.6 h for 221 patients in the sham group. Again, there was no difference between the two groups (MD − 2.21 h; 95% CI − 17.23–12.81, P = 0.77). Heterogeneity was moderate (I2 = 61%). The number of patients with tCr50 within 24 h was 170 out of 420 patients. One hundred nine of 288 patients in the RIC group and 61 of 132 in the sham group were within 24 h, and there was no significant difference between the two groups (RR, 0.98; 95% CI, 0.61–1.56, P = 0.93). Heterogeneity was almost high (I2 = 75%). The eGFR at 12 months after transplantation was 62.0 and 58.4 ml/minute/1.73 m2 in RIC-applied 506 patients and 309 patients in the sham group, respectively. The eGFRs of the two groups were not significantly different (MD 2.15 ml/minute/1.73 m2; 95% CI − 0.61–4.92, P = 0.13). SMD was 0.12 (95% CI − 0.02–0.27, P = 0.10). The heterogeneity was very low (I2 = 0%).
All outcomes that excluded non-low-risk studies were re-evaluated for sensitivity analysis. The validity of the 3-month mortality rate could not be assessed as it did not include any low-risk studies. Both mortality within 12 months (RR, 0.32; 95% CI, 0.02–5.11, P = 0.42) and finally reported mortality (RR, 0.43; 0.19–0.99, P = 0.05) remained non-significant differences between the RIC group and sham group. Secondary outcomes, including DGF (RR, 0.64; 95% CI, 0.14–2.94, P = 0.57), graft rejection (RR, 1.04; 95% CI, 0.59–1.82, P = 0.90), tCr50 (MD − 3.67 h; 95% CI − 21.17–13.82, P = 0.68), tCr50 within 24 h (RR, 1.15; 95% CI, 0.69–1.90, P = 0.59), and eGFR (3.07–0.38) − 6.53 0.08) all yielded non-significant results. A funnel plot to evaluate publication bias could not be created because there was no integrated result of more than 10 studies across all outcomes. Additional file 4 provides the quality of each result value evaluated using the GRADE. All primary outcomes were found to lack precision due to the small number of studies and participants. In addition, studies related to tCr50 did not always show the same tendency and showed high heterogeneity, so the inconsistency was evaluated as serious. Because the RIC protocol was slightly different for each study, serious indirectness was evaluated in terms of indirectness when the location or time period of the application of RIC was different. As a result, mortality within 12 months, the incidence of delayed graft function, and tCr50 were judged to be of very low-quality evidence. The other outcomes also appear to be low quality of evidence.
Subgroup analysisAlthough a plan for subgroup analysis was registered in PROSPERO, the authors judged that the number of studies included in this meta-analysis was so small that a subgroup analysis with sufficient evidence could not be performed. Therefore, the results of the subgroup analysis were not reported.
留言 (0)