In this review, we synthesised the available primary studies on the outcomes of paediatric cataract surgery with intraocular lens implantation in SSA.
Patient characteristics and presentation
All the studies in this review had a male preponderance of participants even though there is no biological evidence to support a sex-specific male predisposition in the prevalence of congenital or non-traumatic developmental cataracts [29]. Some studies [21, 24] reported one reason is that in a lot of African communities, boys are awarded a higher societal value than girls. Other studies on paediatric cataract surgery from Africa have reported the similar findings of gender discrepancy with similar explanations [30, 31]. These findings suggest a need to improve equitable access to paediatric cataract surgery in SSA.
The majority of the participants in the studies experienced a long preoperative delay which is not uncommon in SSA [25]. African studies that investigated the reasons for lag time and its association with visual outcomes defined delay as ‘more than 12 months’ before receiving a cataract operation [25, 26, 32]. This is likely due to pragmatic reasons, as it is a routine occurrence to have children with cataracts present late to the hospitals. In principle, for congenital and infantile cataracts, by the time the children are delayed for 12 months, the optimum time for surgery has passed [33, 34].
Mwende et al. [32] reported on the causes of delayed presentation for non-traumatic cataracts in Tanzania. They found that a longer distance from the eye care facility significantly increased the delay in presentation. Furthermore, there was a positive correlation between rising maternal socio-educational status and a reduction in delay in presentation. This is because these mothers are more likely to have some knowledge of the problem and the treatment that exists. They are also more likely to have the financial means to access eye care services and accept the surgical services offered.
The lag time from the studies in this review was not qualified; it is unclear the extent of delay that resulted from late recognition of the cataract by the children’s caregivers, delay in accessing eye care services, and the delay that resulted from waiting for surgery after presentation to an eye care facility. This information would be crucial in formulating an approach to dealing with the primary barriers that exist at the community level. One study from Southwest Nigeria that investigated the factors associated with early versus late presentation to tertiary eye care facility found that children whose cataract was detected by their mothers were more likely to present to the eye care facility within 3 months of detection [35]. In addition, these children were also more likely to present at a younger age than cataracts detected by other caregivers [35]. This suggests that educating and empowering mothers about cataract in children may be a tool in the arsenal of tackling blindness from childhood cataracts.
Preoperative assessment
This review found that the proportion of blind eyes preoperatively in all the studies ranged from 50 to 100%. Preoperative findings are essential in prognosticating the outcome of surgery. The presence of strabismus and/or nystagmus can adversely affect outcomes, and their prevalence varies widely among studies [36]. Strabismus prevents the development of binocular vision, and the amblyopia it causes can have adverse aesthetic and psychological effects on the child [36]. Moreover, the presence of nystagmus and strabismus are indications that substantial visual deprivation has occurred [24]. Other studies have reported an association between poor preoperative vision and limited improvement in post-operative visual acuity [22, 25, 28, 37].
Visual outcomes
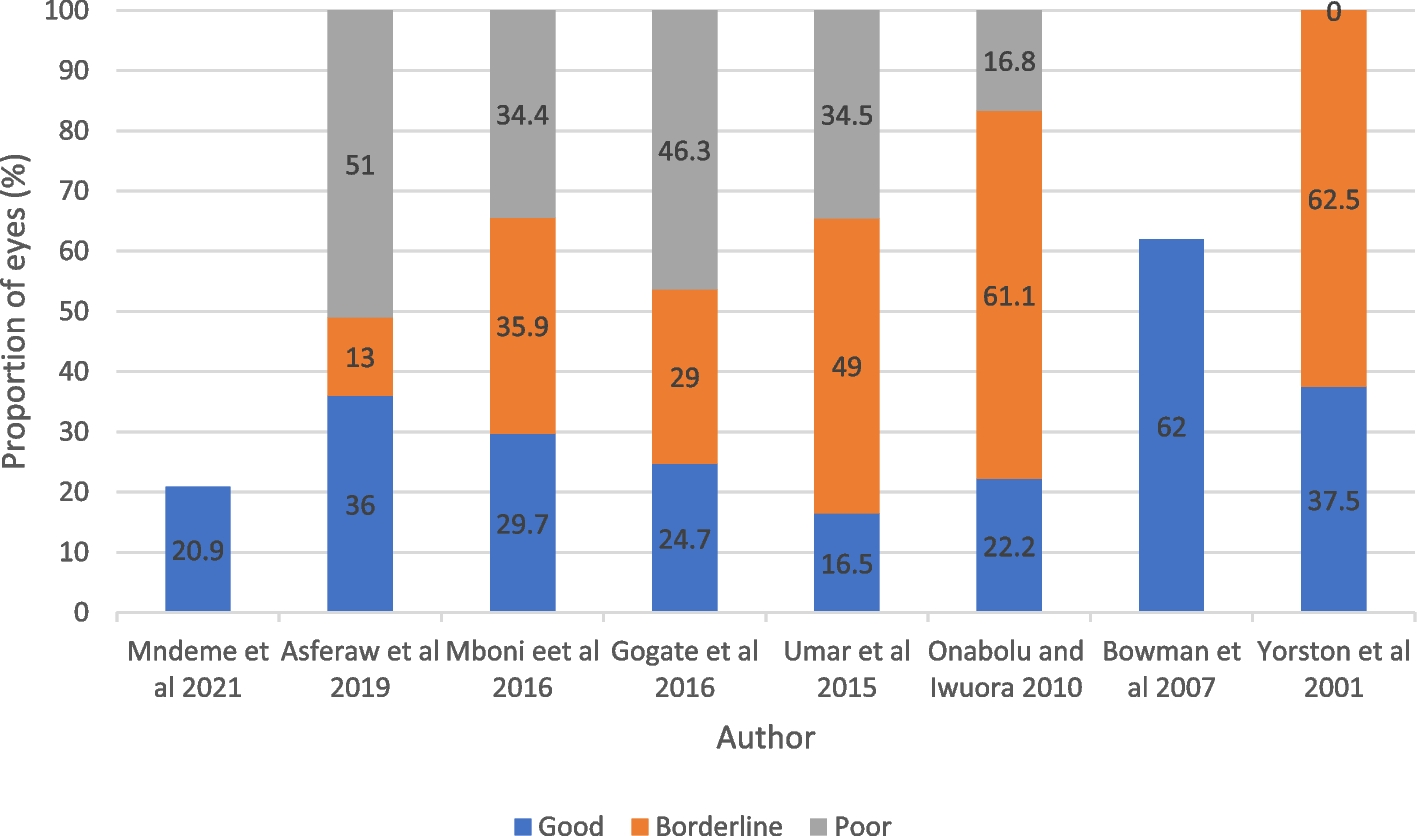
During our literature review, we did not find standardised benchmark indicators for outcomes of paediatric cataract surgery comparable to the WHO guidelines established for adult cataract outcomes. Similarly, in their work on outcome indicators in paediatric cataract surgery, Nihalani et al. [38] did not identify any publication focused on benchmark indicators in paediatric cataract surgery. As such, the WHO categorisation was used in this review. The pooled proportion of eyes that achieved a good visual acuity in the short-term period was 31% (CI, 20–42). Although we did not find studies from high-income countries that defined the cut-off for ‘good visual outcomes’ as 6/18 like in the studies in our review to offer a direct comparison, there were several studies that used the cut-offs of 6/12 and 6/15 (Additional file 1: Appendix 7) The American studies Peterseim et al. [39], Wilson et al. [40], and Struck et al. [41] reported that 27 (91%) (CI, 80–97), 48 (72%) (CI, 59–82), and 13 (85.7%) (CI, 66–100) of eyes achieved a visual acuity of 6/12 or better good visual outcome at the last follow-up visit, respectively. In the UK, a study by Cassidy et al. [42], 25 (73.5%) (CI, 51–80) children achieved a visual acuity of 6/12 or better. Furthermore, the European study Ambroz et al. reported that 34 (54.0%) (CI, 41–67) of eyes achieved a post-operative acuity equivalent to 6/15 of better. Although these studies are not a direct comparison, the cut-offs of 6/15 and 6/12 are a higher standard of visual acuity. It thus suggests that outcomes that are achieved in middle- and high-income countries are superior to those from SSA.
It has been proposed that during visual development, there is a short, well-defined period in early life where the neuronal pathways are robustly restructured in response to sensory input [43, 44]. Years after this ‘critical period’ the same stimuli have less influence on visual development. What follows from these findings is that the occlusion of one eye during this critical period in early life results in the development of a suboptimal visual acuity in the deprived eye that persists into adulthood if left uncorrected [45]. Our expectation would be that children with developmental cataract would obtain better visual outcome because during the critical period, there was no sensory deprivation, and thus, they attained optimum vision prior to the cataract.
It should be noted that the visual outcomes in SSA may be better than those reported in this review. This is because of the lack of long-term follow-up for visual rehabilitation and maturation [25], especially in younger children. Moreover, the visual function is not limited to visual acuity and other factors such as contrast sensitivity and stereopsis need to be considered. However, no study in this review reported on post-operative contrast sensitivity testing, and only one study, Gogate et al. [25], measured stereopsis preoperatively and on follow-up visits. The majority of eyes had poor stereopsis, with only 9 (18%) children achieving better than or equal to 400 s of arc.
Post-operative follow-up
A comparison of the follow-up times from the studies in this review to those from studies in high-income countries revealed that the latter have longer follow-up times for patients. For example, in the American study Ledoux et al. [46], the median follow-up time was 3.65 years. Similarly, Repka et al. [47], in their multicentre study of 994 children, retained 88.4 and 66% of participants at 1 and 5 years. Follow-up in Africa is usually challenging for various reasons, such as the long distance from the tertiary eye care facility, which is coupled with poor road infrastructure, financial constraints, and lack of awareness of the importance of long-term follow-up [48]. Unfortunately, without appropriate post-operative follow-up, paediatric cataract surgery alone produces limited results [49]. The value of long-term follow-up visits can be evident if the child receives the appropriate care at each visit. In many parts of SSA, post-operative services from allied personnel such as orthoptists, refractionists, and low visual aid service providers are lacking [50]; thus, the care received is likely to be suboptimal.
Post-operative complications
Acute uveitis is more common in children as they mount a greater inflammatory reaction following intraocular surgery due to an immature blood-aqueous barrier [51]. Patients are typically prescribed topical steroid eye drops and cycloplegics post-operatively [51]. These were prescribed in all the studies included in this review. Literature shows a variable incidence of uveitis after paediatric cataract surgery. The proportion of eyes with acute uveitis in this review varied from zero in Gogate et al. [25] to 30.5% in Yorston et al. [21]. This is comparable to isolated studies from the west. In the American study by Ledoux et al. [46], no eyes in their series of 139 children had post-operative uveitis, whereas in the UK study by Cassidy et al. [42], uveitis occurred in 28.2% of eyes. However, the pooled proportion of uveitis in our study was found as 12% (CI, 2–21).
Glaucoma is a significant risk in paediatric cataract surgery. Recent multicentre prospective studies in high-income countries reported the incidence of glaucoma after paediatric cataract surgery to be 10% in the first year of follow-up, with the condition occurring in both aphakic and pseudophakic eyes [52, 53]. The highest proportion of eyes with elevated intraocular pressure was 2.9% in Mndeme et al. [28]. Glaucoma after paediatric cataract surgery is typically late-onset open-angle glaucoma [11], although it can be observed within the first few months following surgery. Most early-onset glaucoma is due to vitreous pupillary block or inflammation. But with advances in technology, changes in surgical techniques and the appropriate use of anti-inflammatory medication post-operatively, early-onset glaucoma is much more uncommon [54]. The low number of eyes that developed glaucoma in our review can be explained by the short follow-up time. Therefore, it can be anticipated that if there were a longer follow-up, there would be a larger proportion of eyes seen with glaucoma.
Eyes that have undergone cataract extraction are at an increased risk of retinal detachment. Like aphakic or pseudophakic glaucoma, retinal detachment is also a long-term complication. In Denmark, a study of 1043 eyes of children aged 0 to 17 years by Haargaard et al. [55] reported that 25 eyes developed retinal detachment after a mean duration of 9.1 years after surgery. They further reported an overall 20-year risk of retinal detachment of 7%. This highlights the need for lifelong monitoring in these patients. Our review has low numbers of eyes that developed retinal detachment for the same reason as the low number of glaucoma, which is the short follow-up time.
Heterogeneity in the effect sizes
Analysis output for good visual acuity revealed that Q-statistic was 55.83 with p-value less than 0.0001, and I2 statistic was 87% (CI, 78–93). This indicated the presence of large heterogeneity in the effect sizes. This may result from the clinical and methodological differences across studies in this review. As previously outlined, there were variations in how the surgical procedures were conducted. Furthermore, in some studies, there was one surgeon who performed paediatric cataract surgeries, whereas some studies had multiple surgeons. In addition, the small number of studies included in the review may be the reason heterogeneity in the effect sizes is uncertain. Subgroup analysis based on whether biometry was done or not, and whether single IOL or multiple IOL types were used revealed small heterogeneity which was not significant in any of the strata. This indicates that in addition to the small number of studies considered, heterogeneity in the effect sizes was largely due to variations in the methodological designs of the studies.
Challenges that result in inferior outcomes in sub-Saharan Africa
Early surgical intervention is recommended for bilateral congenital cataracts to improve visual outcomes [33], and for unilateral cataracts, this intervention is recommended even earlier [34]. As seen from this review, the majority of patients had a lag time of more than 12 months and, in some cases, more than 36 months. In high-income countries, there are surveillance programs for routine screening of neonates for early recognition of any lens opacity and thus provide timely surgical intervention [56]. On the other hand, in low-income countries, research suggests that long lag times are multifactorial, ranging from sociocultural barriers at the community level to logistical and organisational barriers within the health care system [57]. In some cases, the late presentation is due to poor health-seeking habits of the child’s guardians, as illustrated in Gogate et al. [25], where a quarter of guardians stated the reason for the delay in seeking help as ‘did not see the need to come to hospital.’ In situations where the symptoms are painless and not considered life-threatening, there may be a delay in presentation to tertiary eye facility for treatment [58].
Another reason for poor outcomes is the shortage of specialised paediatric ophthalmologists in SSA to cater to the immense burden of paediatric cataracts. Accessing sub-specialty training for paediatric ophthalmology is difficult, especially in Francophone Africa; thus, there is a continued lack of skilled eye care providers needed in tertiary hospitals [59]. In addition, there is a lack of visual rehabilitation facilities in SSA, especially for very young children. The standard of practice for managing these children is to prescribe contact lenses in lieu of intraocular lens implantation due to the increased risk of post-operative complications and higher reoperation rates in this patient group [60,61,62]. However, their use in SSA is impractical [21]. The majority reside in rural areas where clean running water is scarce, making personal and ocular hygiene a challenge [63]. This is further compounded by the high cost of the lenses and lens cleaning solutions. Other associated problems such as the risk of microbial keratitis and lens loss also limit the use of these methods [8]. There is a paucity of research on the safety and effectiveness of these interventions in the African context. With all the problems surrounding contact lens usage and the rise of published case series reporting promising results with intraocular lens implantation in younger children [39, 64,65,66], some paediatric surgeons are now moving to primary intraocular lens implantation in younger children.
Whether children are left aphakic or have intraocular lens implantation, they still require optical correction to maximise visual outcomes [67]. Although glasses are more appropriate for the African setting, there are few children who get the glasses even after being refracted. For instance, the Madagascan study Randrianotahina et al. [68], in their series of 86 children, found that despite three-quarters of patients having refraction performed, only 3.5% received glasses. Furthermore, the glasses may break or get lost [21], after which they may not be replaced. Other challenges in prescribing glasses to children include difficulties obtaining accurate refraction and the availability of suitable frames for very young children [21].
Strengths and limitations
This review has scope for novelty in adding to the knowledge gap regarding paediatric cataract surgery. To our knowledge, this is the first review focusing on collating outcomes of visual outcomes of paediatric cataract surgery across sub-Saharan Africa. The inclusion of primary research studies combined with rigorous article screening and quality assessment provides a comprehensive evaluation of the available evidence.
A limitation of this review is the presence of significant heterogeneity within the included studies. Given the context of the SSA setting, the nature of the study population, and intervention under investigation, identifying controlled trials for more accurate and reliable estimates proved challenging. Nevertheless, it is important to note that this review emphasised narrative synthesis of the results over quantitative analysis, aiming to highlight the underlying reasons behind the observed findings.
Caution is advised when interpreting our pooled estimate of good outcomes, as not all factors influencing post-operative visual acuity were systematically analysed. For example, the primary studies lacked information on the measures employed for visual rehabilitation in patients. Moreover, for those implementing amblyopia treatment, details on treatment compliance and the ultimate visual outcomes post-treatment were not reported. There was also no information provided on optical correction compliance for those who received glasses. Lastly, the follow-up period for most of the studies was very short; thus, visual acuity conducted on the young infants may not be reliable. A longer follow-up of patients is needed to further discuss the surgical outcomes of cataracts in SSA.


留言 (0)