
記住我
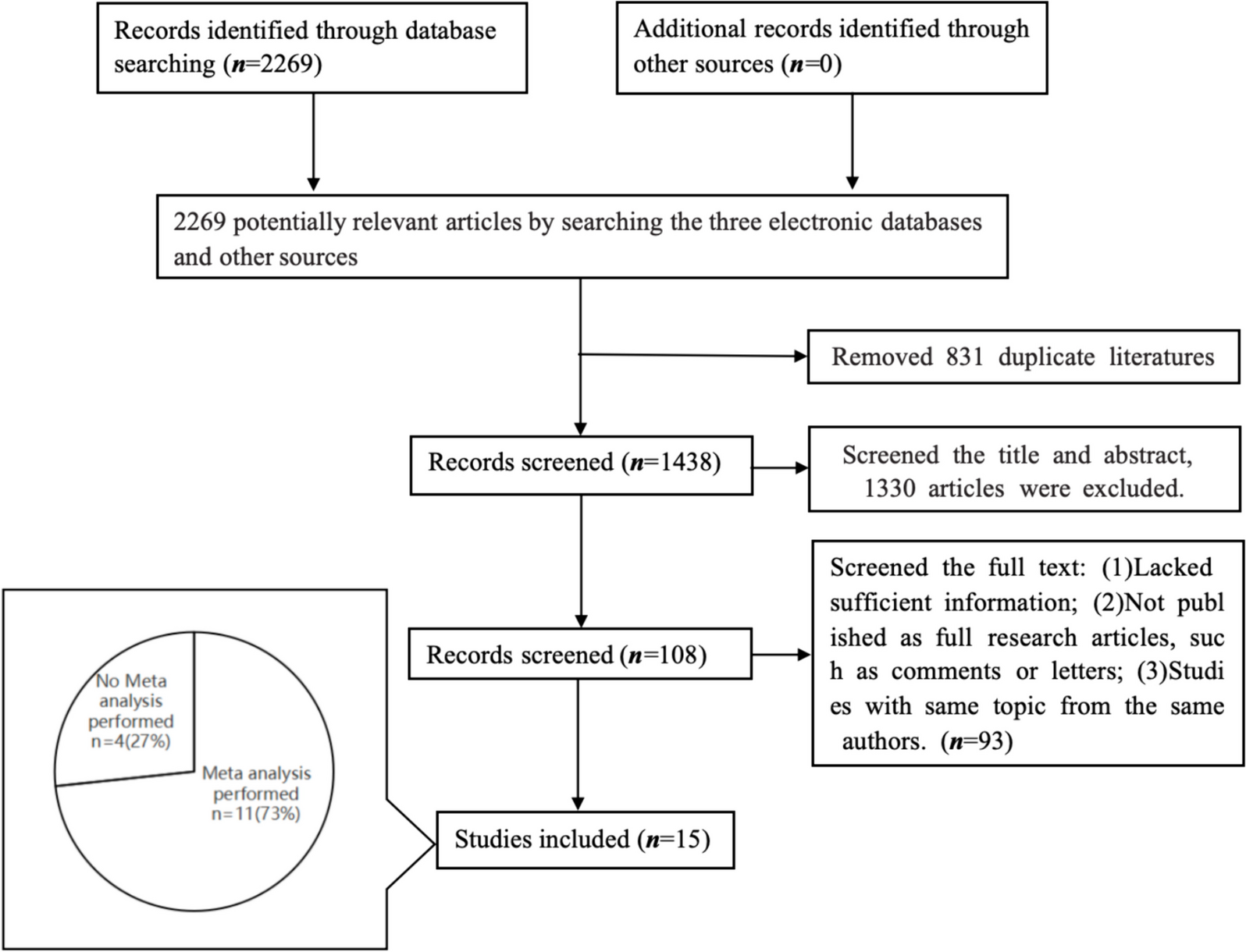
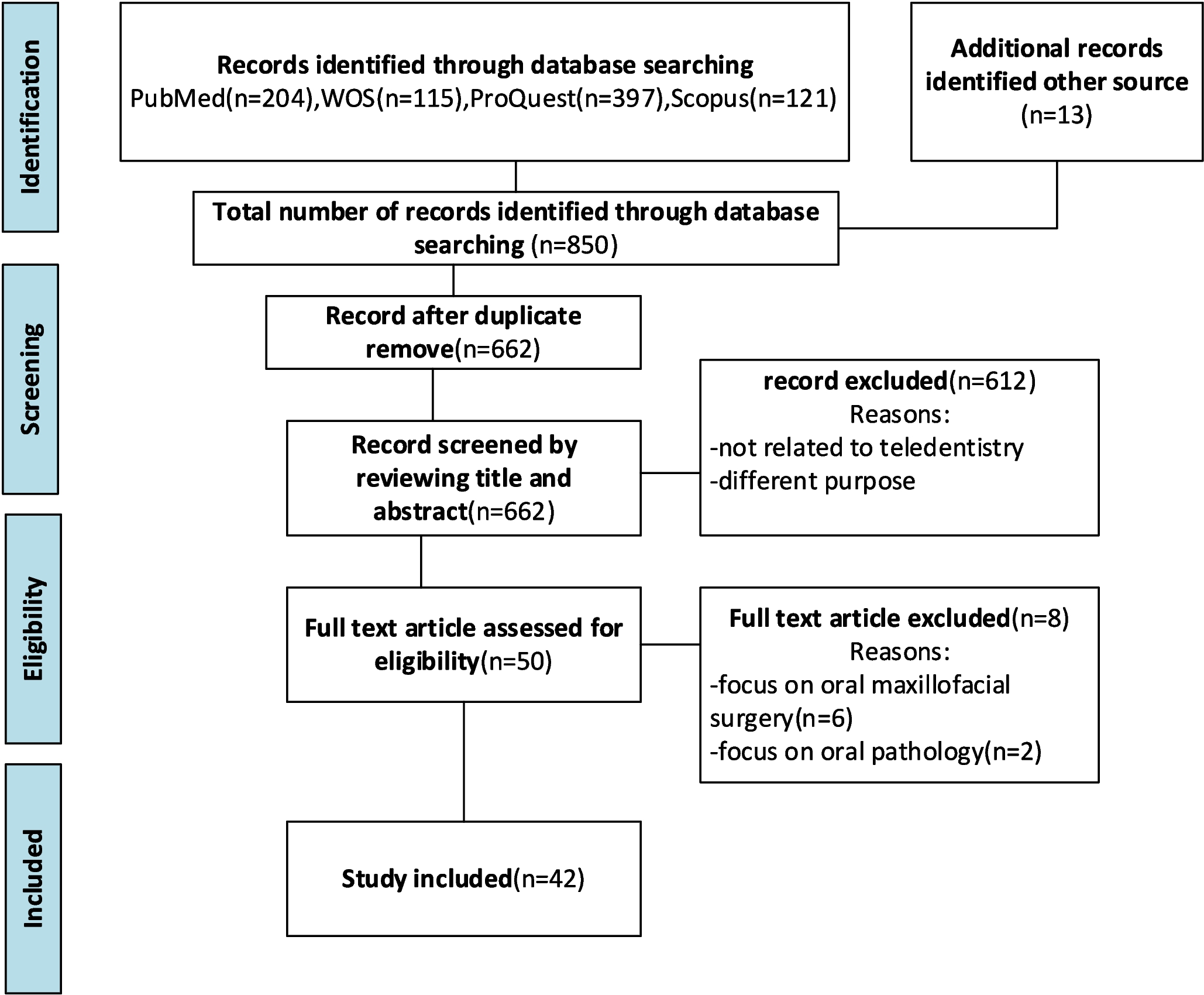
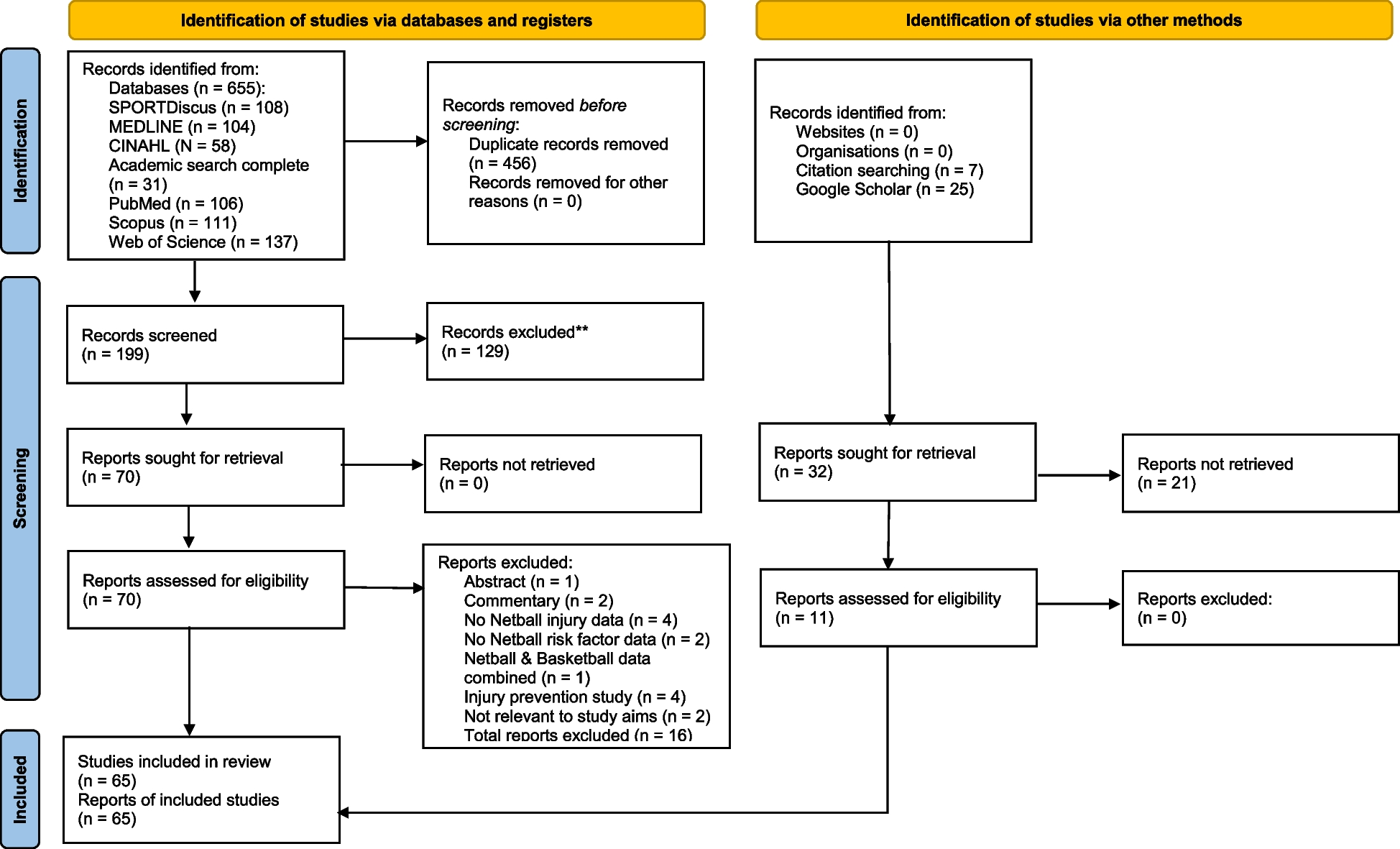
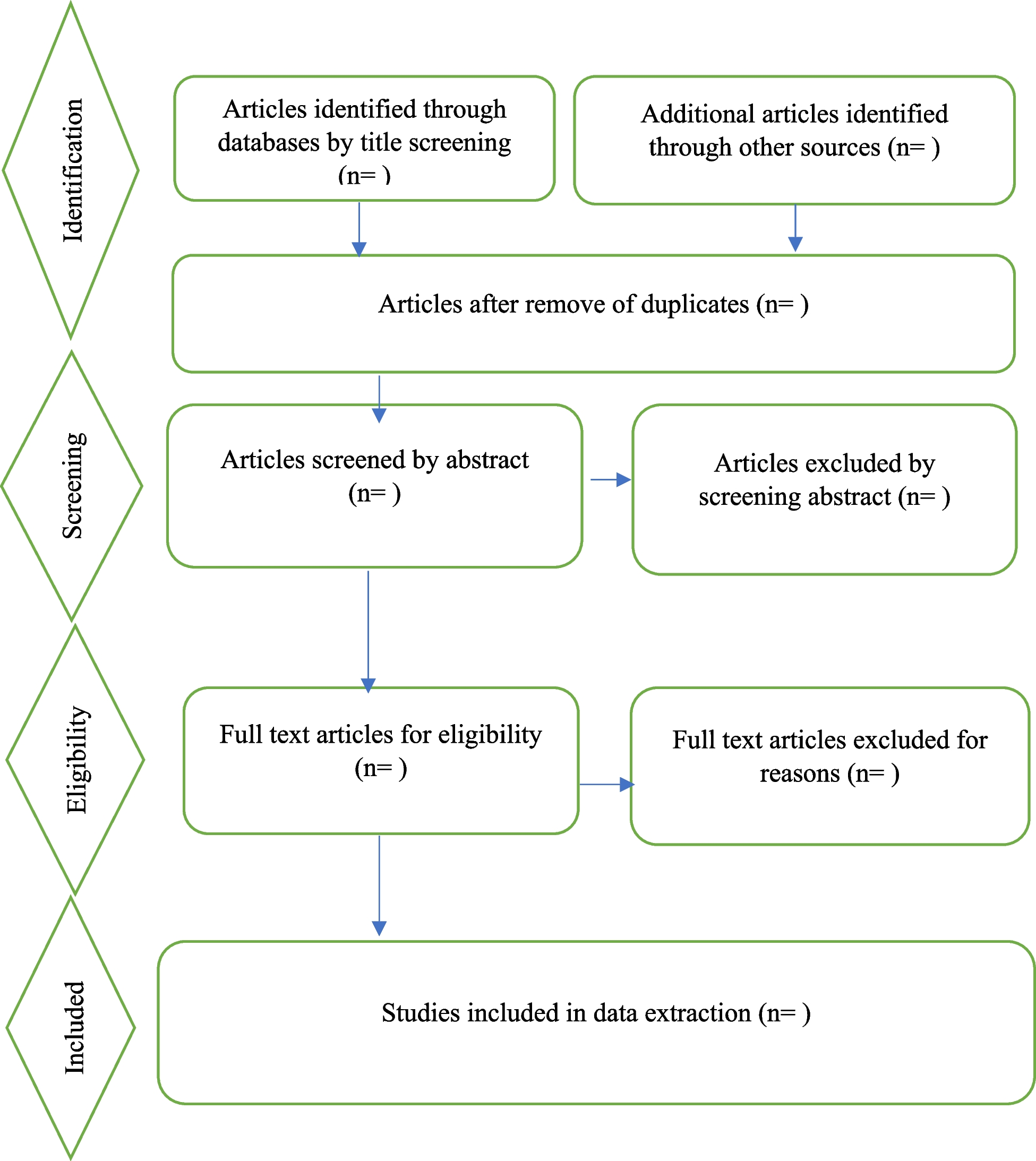

After comprehensive screening, eleven studies that met the eligibility criteria were retained for the qualitative evidence synthesis [43,44,45,46,47,48,49,50,51,52,53]. These studies were published between 2003 and 2022. Ten studies employed only qualitative methods [43,44,45, 47,48,49,50,51,52,53], typically using interviews and focus group discussions for data collection. One study used a mixed methods approach [46]. Participants of nine studies included only African-born women [43,44,45,46,47, 49,50,51, 53], while two studies presented data from women of African and Asian backgrounds [48, 52]. Responses specific to African-born women were extracted from these studies. The included studies were conducted in five Australian states, with most from Victoria [43,44,45, 49] and Queensland [46, 51, 53] (Table 1). Seven studies [43,44,45, 47, 48, 50, 52] met all quality criteria, while four studies [46, 49, 51, 53] met four out of the five criteria. Article screening and the selection process are illustrated in the PRISMA flow diagram [54] (Fig. 2).
Table 1 Characteristics of the studies included in the qualitative evidence synthesisFig. 2
PRISMA flow diagram indicating searches of databases, article screening and selection
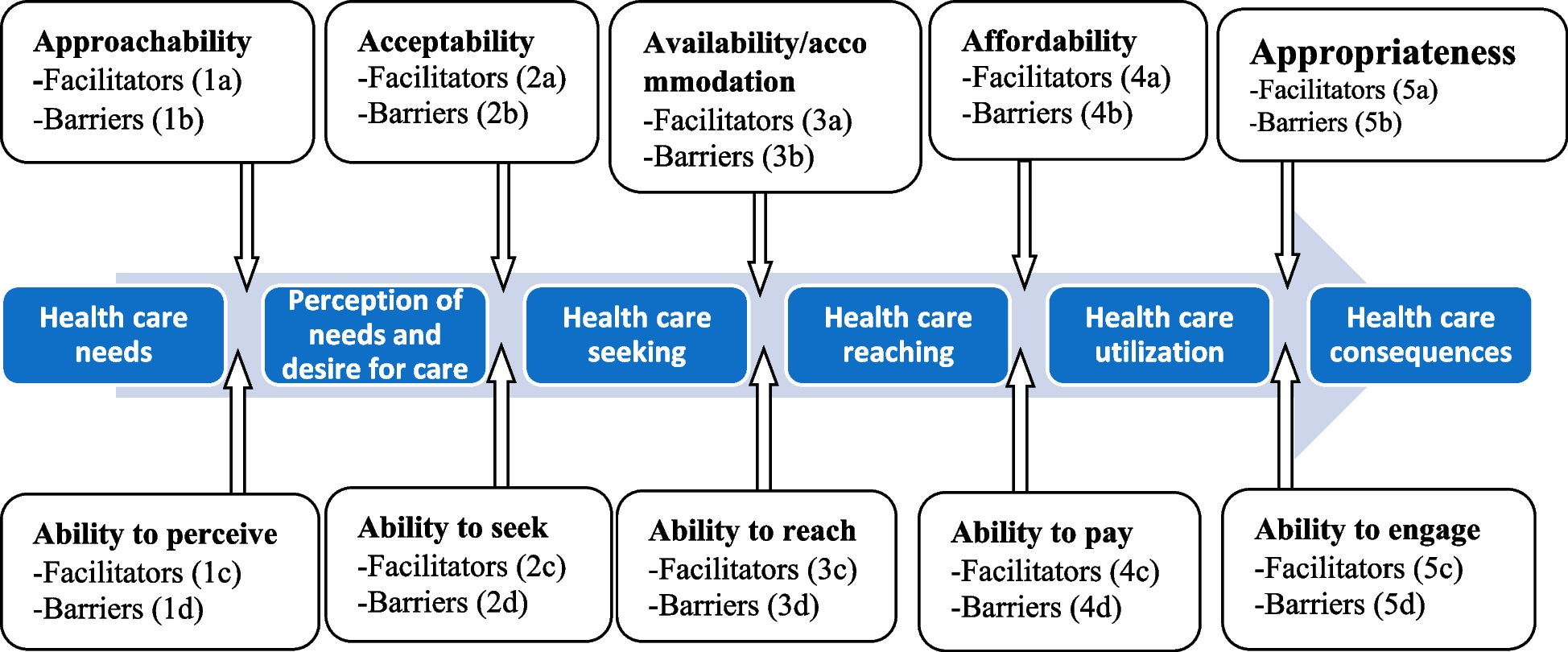
Qualitative evidence synthesisThe qualitative findings reported in the included studies are presented below under five Levesque et al.’s conceptual framework of healthcare access domains [22], and details of the themes are presented in Table 2. We also presented the barriers and facilitators of access to maternity care excerpted from all studies in Table 3.
Table 2 Barriers and facilitators identified from the included studiesTable 3 Barriers and facilitators of access to maternity care among African-born women living in AustraliaPerception of needs and desire for care ApproachabilityApproachability refers to the availability of adequate information about existing services and how people identify and reach for care [22]. The provision of maternal health education at the hospitals was considered a provider-side facilitator (1a) that supported African-born women to access maternity care [46]. However, African-born women reported several provider-side barriers (1b) for accessing maternity care in Australia. Most women claimed that a lack of maternal health information [43, 45] limited their understanding of the purpose of the services [48]. Due to a lack of knowledge about the available maternal health options [50] and a lack of knowledge about where to obtain the services [53], some women missed important maternity care appointments available at the early stage of pregnancy. A woman presented her concern: ‘Because it was my first time having a child here, and I don’t know exactly the places I have to go like hospitals. … I stayed at home until I was 7 months pregnant, I hadn’t been even to first check-up’ [50, p: 301].
Ability to perceiveThe ability to perceive is related to health literacy, knowledge, and beliefs about health and sickness [22]. It was reported that some women are interested in receiving information about maternal health, which we identified as the only user-side facilitator (1c) [45]. However, several user-side barriers (1d) were reported to affect women’s ability to perceive. Most women perceived childbirth as a natural process with medical assistance, including analgesia for labour pain [45, 51] and medical procedures during pregnancy [45, 49] being perceived as not necessary. The use of medical technology during labour was perceived as distressing for some women [46]. Therefore, some women preferred to labour at home for as long as possible, believing this would prevent birth interventions, including caesarean section [51]. For example, a woman reported rejecting medication for labour induction because she wanted only a natural birth [45, 48, 49], feeling alone and feeling different from others in the hospital environment [44, 51], and women’s belief in complementary (natural) therapies over modern medicine [51] were reported to hamper care seeking behaviour of African-born women. Here is a perception of a woman who avoided analgesia in the belief that it prolongs labour by cooling the pain: ‘… when you are on labour, then, um, instead you are given hot water, tea, hot tea, dry tea. … for the tablets, … it will cool the pain and still the baby will remain in me. So, I just want the pain should (escalate) so that it [baby] comes out’ [51, p: 467].
Health care seeking AcceptabilityAcceptability relates to how well healthcare services address an individual’s cultural and social needs for them to seek, access, and accept care [22]. Several provider-side factors, such as the welcoming and positive attitudes of midwives [44, 50], being understood by midwives and doctors [44, 52], and having access to bicultural social workers [47] facilitated (2a) African-born women to accept and access the services. Some women considered midwives as very kind [51] and were respectful to women’s culture during service provision [47], which helped to build trustful relationships [45]. African-born women appreciated being asked about their well-being during inpatient stays [51] and families being allowed to be present and provide support during childbirth [50]. For example, a respondent narrated: ‘…so, she tries to meet your needs in the way that you feel comfortable… so I think for her, she treats everybody the way they’re meant to be treated, because she doesn’t treat everybody the same. She kind of – she understands what people’s individual needs are…’ [47, p: 4].
Conversely, a range of provider-side barriers (2b) were reported to affect the acceptability of the services by African-born women. Discrimination [43], unmet needs for maternity care [47], and insufficient time for consultations [48] were reported to affect women’s access to maternity services. Furthermore, women’s care-seeking behaviour was diminished if their preference for female doctors was not met and when staff were angry and failed to respond to their requests [51]. For example, a woman narrated her concerns about service providers: ‘I don’t blame them. I know they are busy, but … You feel you need someone, you know, even if you want something and you press for the nurse, and they don’t come. You feel like … maybe they don’t want you; they don’t want to help you’ [51, p: 465].
Ability to seek careThe ability to seek care is related to personal autonomy, knowledge about the available options, and the freedom to obtain care [22]. A range of user-side facilitators (2c) were reported to improve African-born women’s ability to seek maternity care. Cultural assimilation helped some women develop the confidence to accept the Australian hospital system [45]. Some women felt welcomed and valued by service providers, which improved their ability to seek maternity care [44].
However, many user-side barriers (2d) were reported across studies to affect women’s ability to seek maternity care. Women’s religion was reported as a factor that affected the acceptability of maternity care [46, 49]. For example, a respondent narrated that she would rather die a good Muslim woman than be ‘contaminated’ by having a ‘pork injection’ (routine Heparin injection), which was believed to be a non-halal product [49, 45]. Being asked for private and personal information, such as whether women had been circumcised, was also considered culturally unsafe [47]. Some women preferred not to visit maternity services as they were being labelled and received racially stereotypical comments in hospitals [43]. As described by one respondent: ‘I think it’s hard and people already have these thoughts about you as you walk through the door, like as they see this African woman, they think oh she’s here to cause trouble. I even heard another midwife saying, ‘She should be happy that she’s in Australia” [43, p: 76].
Furthermore, a lack of social support, such as limited family involvement during labour [46, 48] was reported to affect African-born women’s ability to seek care. Prior negative maternity care experiences [47] and a perception of being ignored in hospitals [53] challenged some women's care-seeking behaviour. Women reported being unhappy with attending the service facilities when their culture was not respected, and the hospital food did not meet their religious requirements [46]. A respondent narrated: ‘I feel the staff have little understanding about my culture and … the importance of family during labour. My family was sent home... nobody informed me as to what happened … my family are not happy about it. Food was inappropriate…’ [46, p: 19].
Health care reaching Availability and accommodationAvailability and accommodation are defined as the physical existence of health resources within a geographical location with sufficient capacity to deliver care promptly [22]. Various provider-side facilitators (3a) that improved African-born women’s access to maternity services were related to this domain. Many women across the studies were positive about the availability of services in Australian hospitals [50,51,52]. Maternity services were close to women’s residential homes [44, 52], making accessing care easy. African-born women were happy to visit a facility where they could get multiple services at one point of care [52].
Nevertheless, women reported a few provider-side barriers (3b) that affected their access to maternity care. Despite the satisfactory midwifery care in hospitals, some women described a lack of postnatal follow-up services [43]. Other women reported being frustrated with visiting maternity services as the hospital waiting time was too long [46,
留言 (0)