The annual mortality rate from breast cancer stands at approximately 71,700, ranking it fifth among female tumor-related deaths. From 1989 to 2020, 460,000 breast cancer deaths were avoided among women in the United States, and the decrease in mortality is attributed to better, more targeted treatment and early detection through mammography screening [4]. In China, major cities like Beijing and Shanghai with specialized hospitals offer better standardized care, resulting in a five-year survival rate comparable to Western countries. However, there is a stark contrast in the five-year survival rates between big cities and smaller cities, towns, and rural areas. This difference may be due to the relative weakness in standardization in these regions. However, reports of comprehensive medical practice surveys of hospitals in all regions of the country are still unavailable, especially in the Northwest. In our study, we found that the central hospital in Xi’an absorbs more breast cancer patients. Meanwhile, its level of diagnosis and treatment is more advanced than the surrounding areas in Shaanxi. There was a trend towards centralization and specialization in diagnosing and treating breast diseases.
In this study, we found that more than 60% of patients with breast cancer were diagnosed at stages I and II. This proportion is lower compared to western countries where more than 70% of patients are diagnosed at these early stages, and it can even exceed 80% [10, 11]. In contrast, in developing countries only 20–60% of patients are diagnosed at earlier stages, while a higher percentage, ranging from 30 to 80%, are diagnosed at stages III and IV [11]. According to some studies in China [12,13,14] have also shown that between 60 and 70% of the patients are diagnosed in stage I and II. However, the 5-year survival rate for Chinese women with breast cancer from 2010 to 2014 was only 83.2% [15]. In contrast, the 5-year relative survival for patients diagnosed during 2012–2018 in the Americas was above 99% for stage I disease, 93% for stage II, 75% for stage III, and 29% for stage IV [4]. The proportion of early-stage breast cancer and the 5-year relative survival in China are both below those in developed countries. Early detection of cancer has been shown to greatly reduce breast cancer mortality rates in the long term [16]. Therefore, health education and intervention activities should be conducted to actively promote the importance of screening for breast cancers among young patients.
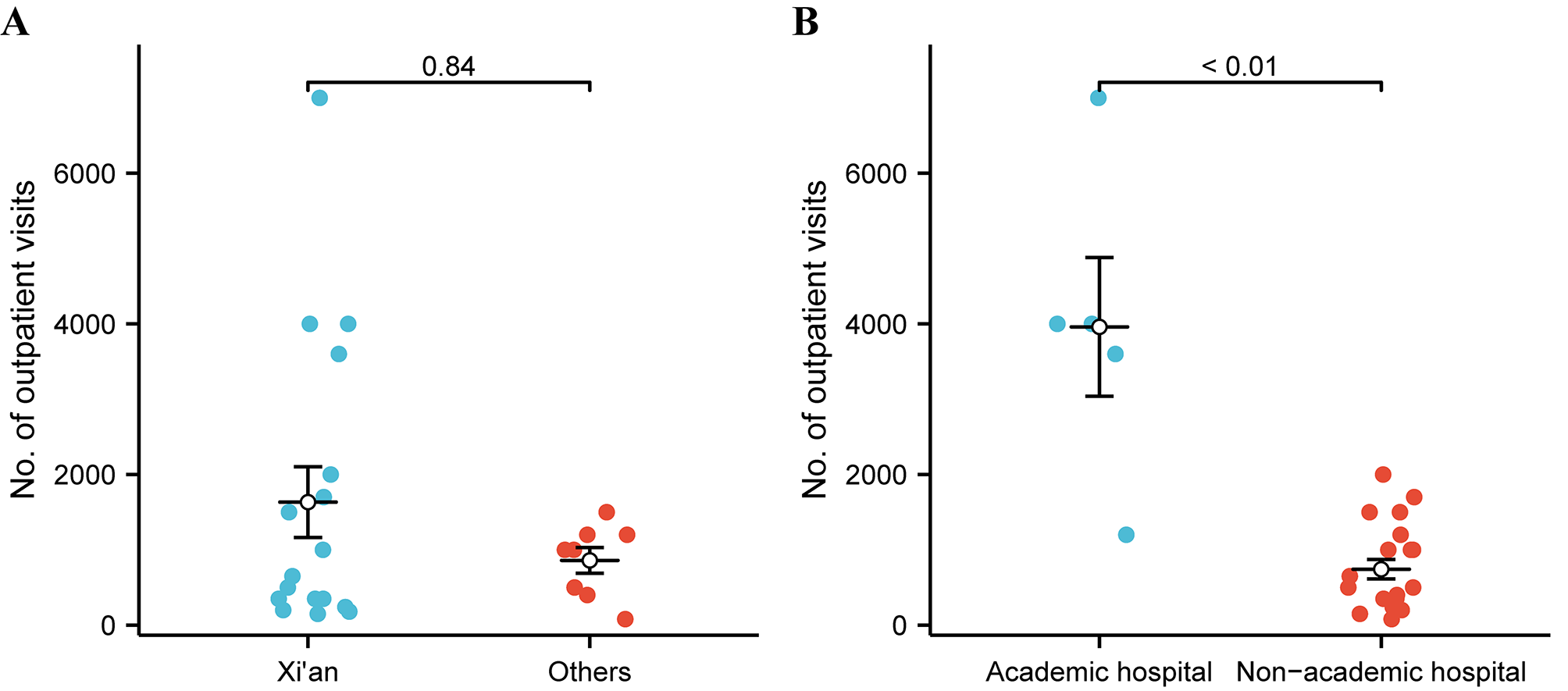
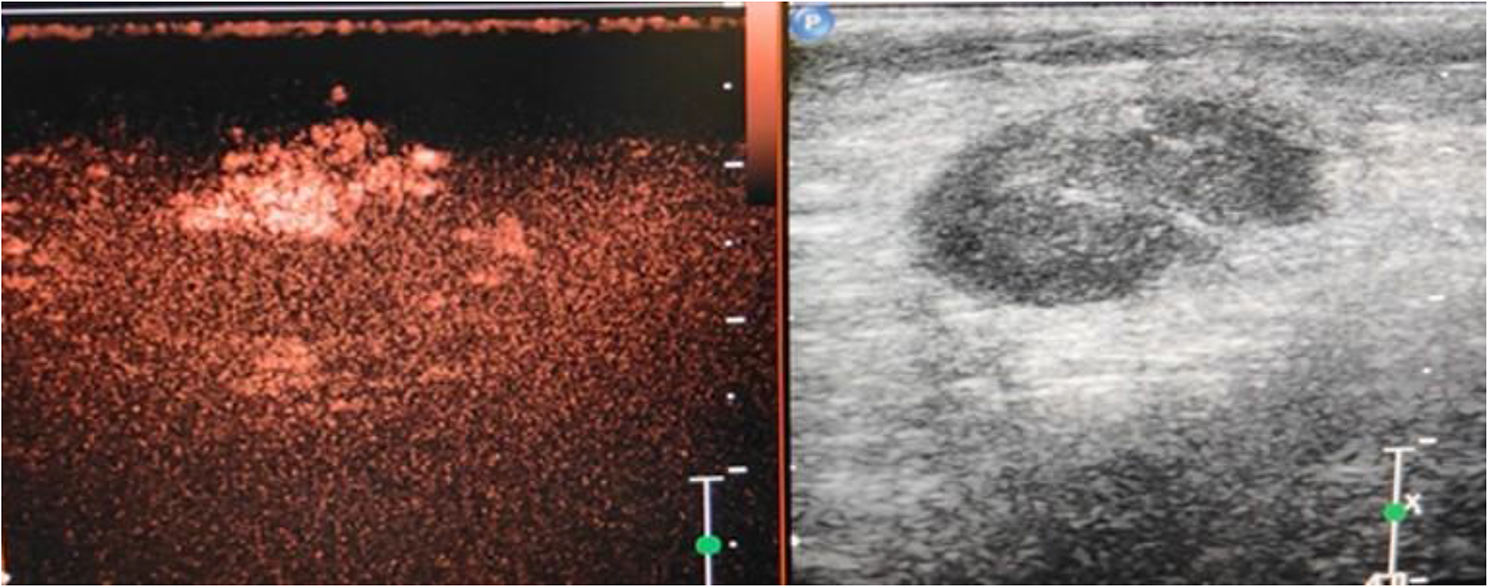
For outpatient visits, people tend to choose academic hospitals. This preference can be attributed to the fact that academic hospitals have specialized clinics, more specialized doctors, and better medical expertise. In outpatient examinations, breast ultrasound is more commonly used than mammography. This is likely due to the characteristics of Chinese women’s breasts, patient acceptance, and promotional efforts. Chinese women generally have smaller and denser breasts compared to white women [17]. Ultrasound is a proper method for screening women with dense breasts [18]. Moreover, the non-radiation and non-painful nature of ultrasound makes it more acceptable to patients. Compared with patients with breast cancer in Europe and the United States, Chinese patients have distinct features, we need more evidence to suppose the strategies of screening for Chinese women.
The survey results indicate that Shaanxi has achieved or even surpassed the national average level in breast-conserving surgery, neoadjuvant and adjuvant therapy, and sentinel lymph node biopsy, as demonstrated by some multicenter studies [6, 7, 9, 19]. We hypothesize that these advancements may be associated with the evolution of breast cancer treatment concepts, the implementation of standardized guidelines, the circulating reports from the Breast Cancer Special Committee, the proactive engagement of academic teams and the change in health care policy. Additionally, easy access to international sources for communication, information exchange at different stages, and the adoption of cutting-edge technology could also contribute to these improvements. However, there are still disparities in the data regarding treatments between different countries.
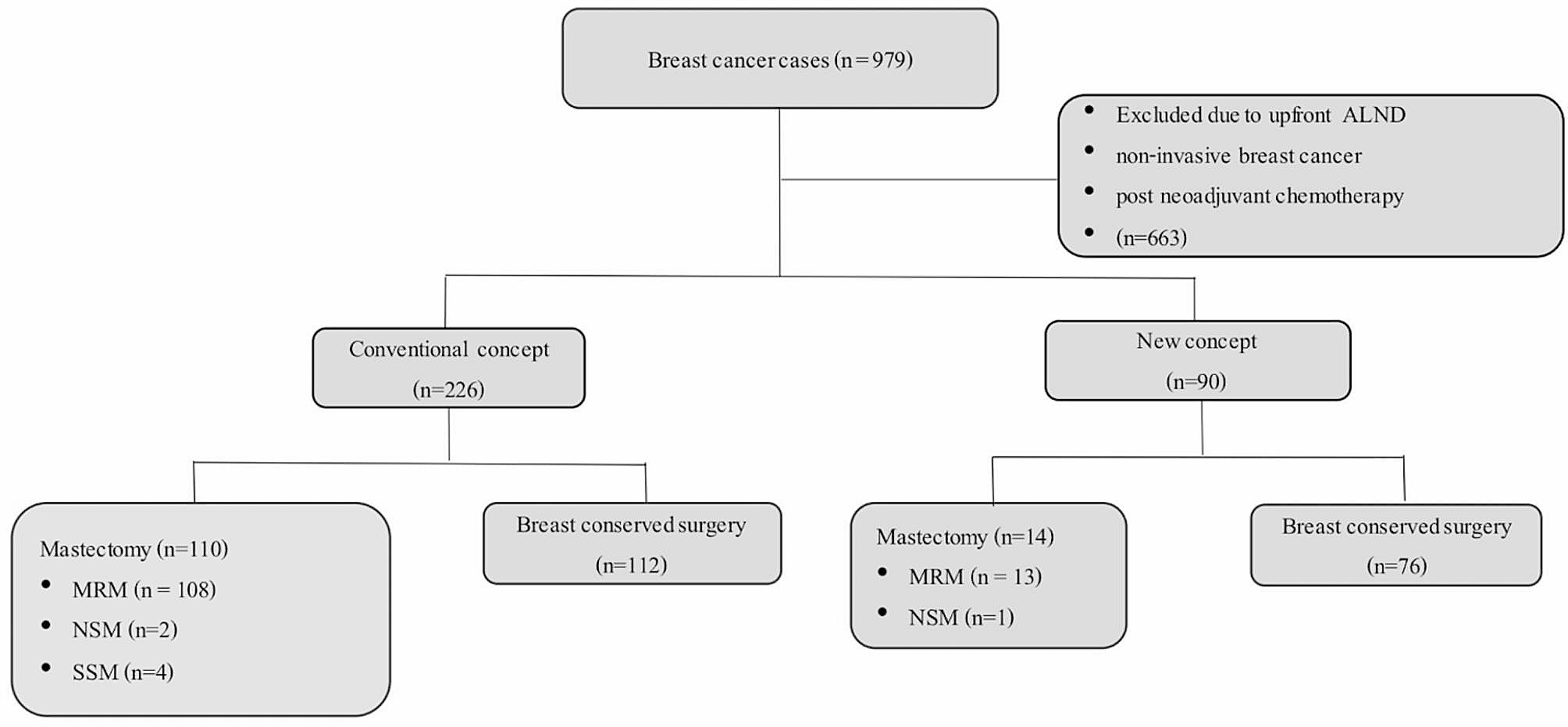
Numerous clinical trials and meta-analyses [20,21,22,23,24,25] have confirmed that breast conserving therapy (BCT) and mastectomy have similar survival outcomes. However, our survey showed that the breast conservation rate in Shaanxi is 23.3%, reaching the national average [9], which is still different from that of foreign countries (America: 60%, Europe: 80%) [26, 27]. We suggest that this is related to the late diagnosis of breast cancer patients in China (Shaanxi) and the uneven level of patient awareness and treatment. Patients in China are relatively conservative in their choice of breast conservation surgery was related to fear of recurrence, avoidance of further treatment and belief in an overall healthy image [28,29,30]. Meanwhile, the choice of BCT is also associated with the hospital providers [28]. Training techniques and surgeon specialization allow physicians to offer women personalized treatment options [31]. Our survey indicates that doctors favor 2 cm margins. In China, intraoperative frozen section analysis is common for breast-conserving surgery. Many hospitals use selective sampling of the nipple, medial, lateral, and distal sections, or suspicious areas identified by the surgeon. This method offers minimal tissue sampling and quick results but may miss some margin statuses. Therefore, doctors prefer wider margins and multi-point intraoperative sampling with pathological examination to ensure negative margins, enhancing surgical safety and patient outcomes. However, as awareness of breast-conserving surgery and the desire for better cosmetic results grow, the trend is shifting towards smaller surgical margins.
According to our survey, 60% (15/25) hospitals routinely performed axillary SLNB for more than 50% of patients with cN0 disease. Larger hospitals commonly conduct SLNB for cN0 patients, akin to the findings of a 2017 cross-sectional study in China [6]. However, the implementation of SLNB in smaller hospitals and non-metropolitan areas still faces challenges. However, it is not widely used compared to in developed countries (China:43.4% [32], Dutch: 93% [33], United States: 91.4% [34]).
Despite substantial high-quality evidence and authoritative guidelines supporting the omission of ALND, most surgeons in China, regardless of hospital type, region, remain cautious about omitting ALND in patients with low axillary SLN burden. This is likely due to the lower rate of breast-conserving surgery and pathologic modalities. This differs from the decreasing trend of ALND rate observed in foreign countries [35]. In the ACSOG Z0011 study [36], which included patients undergoing breast-conserving surgery with 1–2 positive sentinel nodes, the 10-year overall survival (OS) and disease-free survival (DFS) between the SLNB-only and ALND group showed no significant difference. Similarly, in the AMAROS trial and the OTOASOR trial [37, 38], involving patients with sentinel node metastases, individuals were randomized to receive either ALND or axillary radiotherapy. After 10 and 8 years of follow-up respectively, no difference was observed in axillary recurrence or survival. The St. Gallen Consensus Guidelines recommend that ALND can be exempted for patients treated by breast-conserving surgery and radiotherapy, or mastectomy and axillary radiotherapy, with 1–2 positive SLN [39]. The 2024 edition of the Breast Cancer Diagnosis and Treatment Guidelines by the China Anti-Cancer Association also recommends that for patients with 1–2 positive SLNs, axillary lymph node dissection (ALND) can be conditionally and safely replaced [40]. The latest conclusions from the SENOMAC study further confirm that for clinically node-negative T1 to T3 breast cancer patients with 1–2 positive sentinel nodes, either undergoing breast-conserving surgery or mastectomy, most of whom receive nodal radiotherapy, the five-year disease-free survival rate is similar between SLNB-only and ALND group [41]. Given the existing medical landscape and guidelines, it is crucial for China to explore its own path in addressing axillary lymph node dissection.
Our survey also demonstrated that, compared to another multicenter study in China [8], a smaller percentage of hospitals in Shaanxi conducted breast reconstruction compared to hospitals nationwide (56% vs. 87.3%). The observed discrepancy in the adoption of breast reconstruction surgery in Shaanxi province, compared to the more developed northeastern region, may be partly attributed to the limited economic development in the region. Patients in Shaanxi tend to have lower awareness and willingness to undergo breast reconstruction surgery. Additionally, hospitals in the area started offering this procedure later, and there is a scarcity of breast surgeons with plastic surgery expertise. These factors contribute to the slower adoption of breast reconstruction surgery in Shaanxi. Furthermore, fewer hospitals in Shaanxi province performed autologous breast reconstruction compared to the national average, which might be associated with the longer learning curve and patient recovery times for this technique. There is also a notable polarization in breast reconstruction awareness and rates within Shaanxi. Breast reconstruction is more frequently performed in Xi’an compared to other parts of the province. While a limited number of other regions also offer breast reconstruction surgery, they often rely on guidance from hospitals in the Xi’an area. The lower availability of breast reconstruction surgery in surrounding areas may be due to hospital limitations and doctors’ safety concerns. As a result, it is essential to actively promote training and breast reconstruction to address these disparities.
This study provides a comprehensive reflection of the current status of breast cancer diagnosis and treatment in Shaanxi, and includes outpatient treatment information. Aim to promote standardized diagnosis and treatment of breast cancer, and explore treatment strategies suitable for the Chinese region to improve the survival quality of patients.
There are some limitations in this study. Firstly, the 25 hospitals surveyed in this study are mainly 3 A hospitals, and there is a lack of data from grassroots hospitals, which may result in an overestimation of the overall healthcare level in Shaanxi. Additionally, the study did not investigate the survival rates of breast cancer or the prevalence of promising surgical techniques such as laparoscopic surgery. Moreover, the study only provided a general assessment of diagnosis and treatment, without investigating controversial topics in various fields.


留言 (0)