Perioperative management is critical in reducing length of hospital stay, cost of treatment and in improving patient quality of care. The implementation of FTS in surgery was based on evidence-based medicine and has shown great success in the fields of colorectal surgery, liver surgery, and thoracic surgery [5, 12, 13]. However, little is known about its efficacy in urological surgery, particularly with regards to radical cystectomy with urinary output reconstruction. Radical cystectomy with intestinal urinary reconstruction is considered to be a major and complex operative procedure which holds the potential for significant complications and mortality [14,15,16,17]. Our study explores the benefits of FTS with three-port in comparison to CS in a cohort of Chinese patients planned for laparoscopic radical cystectomy and ileal conduit for bladder cancer.
Urinary diversion after radical cystectomy further increases its surgical complexity, especially when it involves bowel interception and reconstruction. The potential for bowel-related complications, including bowel obstruction and bowel perforation, occurs after both laparoscopic radical cystectomy + ileal conduit and in situ neobladder surgery. We analyzed that the bowel takes time to recover from normal peristalsis due to stress such as surgical reconstruction in a short period of time after surgery, and with time if its function does not recover in a short period of time, it may lead to the development of bowel obstruction. In severe cases of intestinal obstruction or perforation with acute peritonitis, timely surgical intervention is very important.
Relatively popular methods of trocar placement include the four-port and five-port methods. The four-port method is characterised by fewer surgical incisions, but it prolongs the duration of the procedure and is not conducive to postoperative recovery. The moderate exposure of the five-port approach is adequate to some extent, and the operative time is relatively short [18]. However, our original intention in using the three-port approach was to make the incision more favourable more favourable to improving the patient’s aesthetics more in line with the minimally invasive concept. Philosophy. However, there is no doubt that this approach increases the difficulty of the procedure and demands a high level of laparoscopic surgical competence. Therefore, it is recommended that only surgeons with laparoscopic surgical competence are suitable for this new approach. But compared with the conventional five-port procedure, it is not restricted by the first assistant.
The concept of three-port surgery is based on the idea that “the left hand is the best assistant”. With the help of an assistant who hold the laparoscope, the assisting hand is used to fully expose the field of vision and to collaborate in the surgery, which facilitates a smooth and less traumatic operation. At the same time, the practice of fast track concept allows patients to ventilate and feed earlier, effectively reducing the incidence of gastrointestinal complications such as intestinal obstruction. Our experience shows that the combination of three-port and rapid recovery can reduce the hospitalization time of patients and effectively reduce the incidence of bowel obstruction and other complications, bringing higher benefits to patients.
Our study found that that patients who underwent FTS with three-port had better postoperative recovery, shorter number of postoperative days and less complications. FTS with three-port can accelerate postoperative recovery while ensuring operative success. Key factors contributing towards the success of the FTS with three-port program may be attributed to thorough patient education and preoperative evaluation. Patient involvement in their treatment motivates them to cooperate with healthcare providers, thus ensuring better recovery outcomes.
Patients undergoing CS would typically be subjected to lengthy bowel preparation regimes and 3 days of prophylactic antibiotics. However, there is little evidence regarding the efficacy of this practice [19]. In contrast, a study reported a higher risk of anastomotic leakage and postoperative infections in patients who received preoperative bowel preparation [20]. Preoperative bowel preparation is thought to alter the delicate balance of intestinal flora while also damaging its protective barrier. Both of these processes accentuate the intestinal inflammatory response and induces intestinal edema. There is an increased risk of infection, which is deletrious to postoperative recovery. Furthermore, liquified bowel content increases the risk of gross contamination of the peritoneal cavity should the bowel inadvertently be perforated during the surgery.
A successful FTS program mandates a multidisciplinary team involving surgeons, anesthetists and nurses. Early enforced mobilization is a critical step in the FTS program. To achieve this successfully, patients should have adequate, portable pain control systems (such as transdermal fentanyl) and good nursing care. A carefully implemented FTS program significantly reduces physiological stress and decreases rates of postoperative complications. This in turn translates to improved patient comfort such as decreased postoperative nausea, allowing them to consume orally faster and experience a shorter overall duration of hospitalization. Early feeding, laxative use and antiemetics promote quicker return of normal gastrointestinal motility [21]. Furthermore, early postoperative oral nutrition also decreases the stress response, reduces catabolism, and combats postoperative complications such as abdominal distension or ileus [4]. The overall shorter duration of hospitalization also translates to lower healthcare costs.
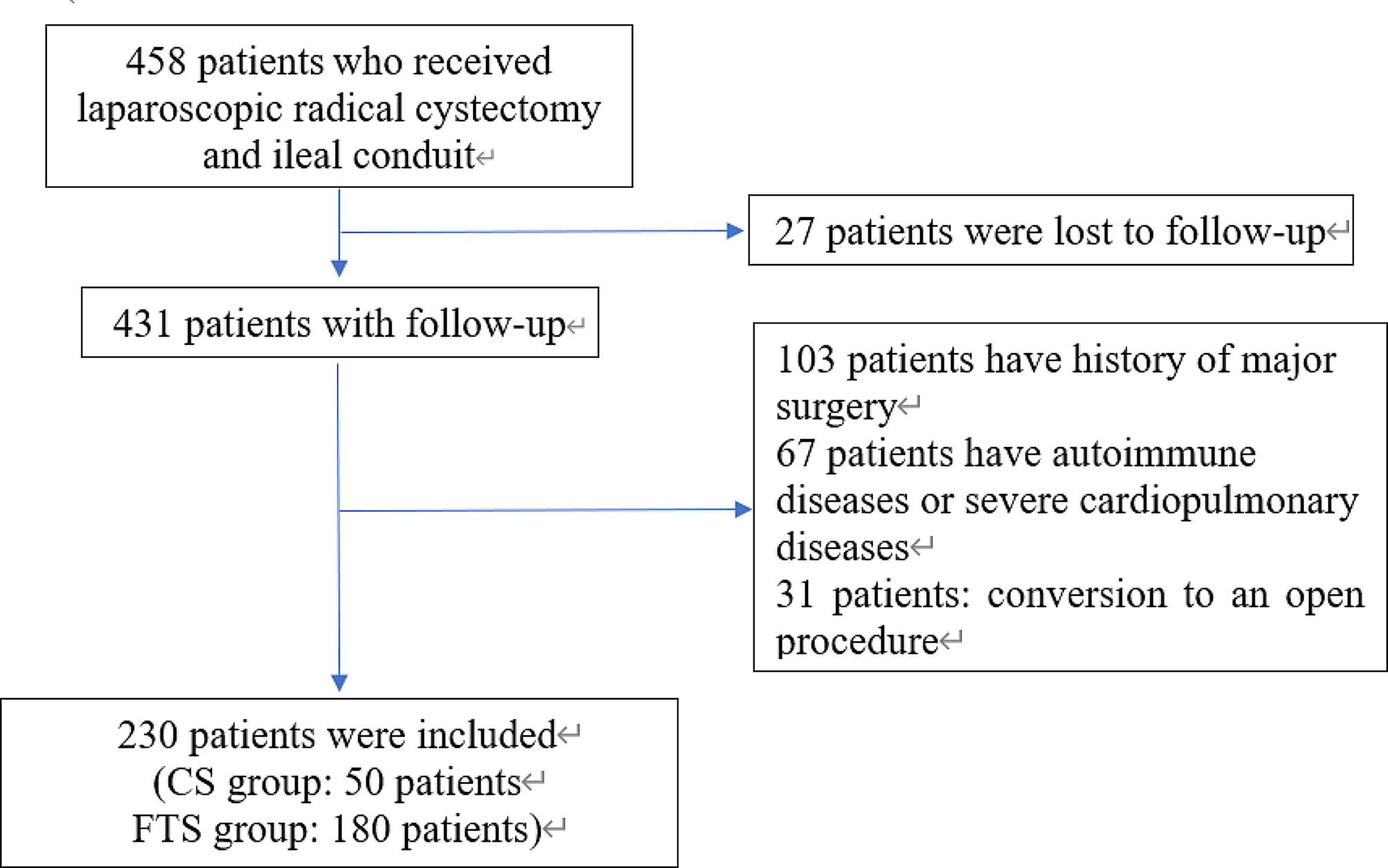
This study is limited due to its retrospective design, small samples size and short follow-up time. Larger randomized controlled trials are required to furnish better quality evidence to support the widespread use of FTS with three-port in urological surgery. Furthermore, the use of FTS with three-port should also be investigated in 3D laparoscopy and robotic laparoscopy given the increasing use of these surgical modalities. Moreover, in addition to the above, studies based on the molecular mechanisms of bladder cancer will further advance the progress of clinical research and will also be suggestive in terms of its development and surgical prognosis [22, 23].
Despite these limitations, the results of the current study have demonstrated that the FTS with three-port program can speed up recovery, lessen stress and shorten postoperative hospital stay. We conclude that the FTS with three-port program is safer and more effective than the CS program for Chinese patients undergoing laparoscopic radical cystectomy for bladder cancer.


留言 (0)