
記住我
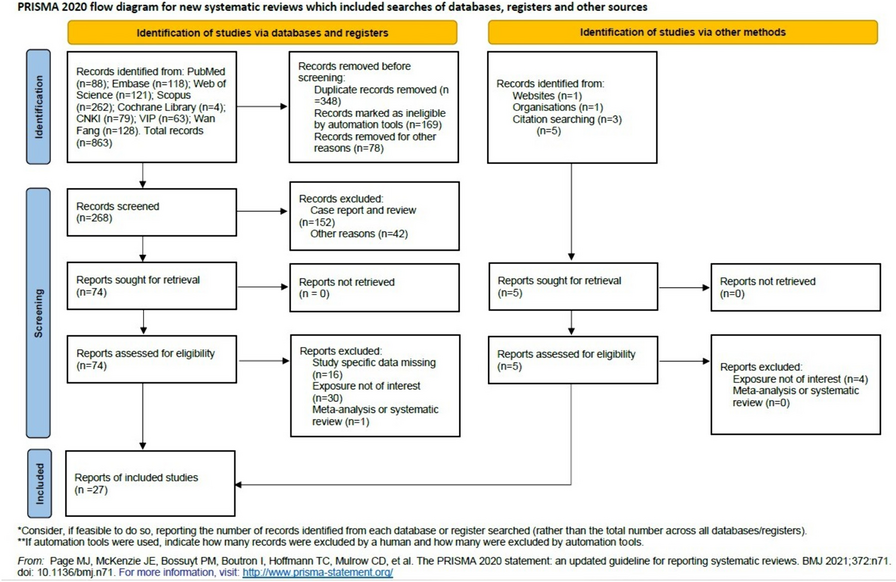
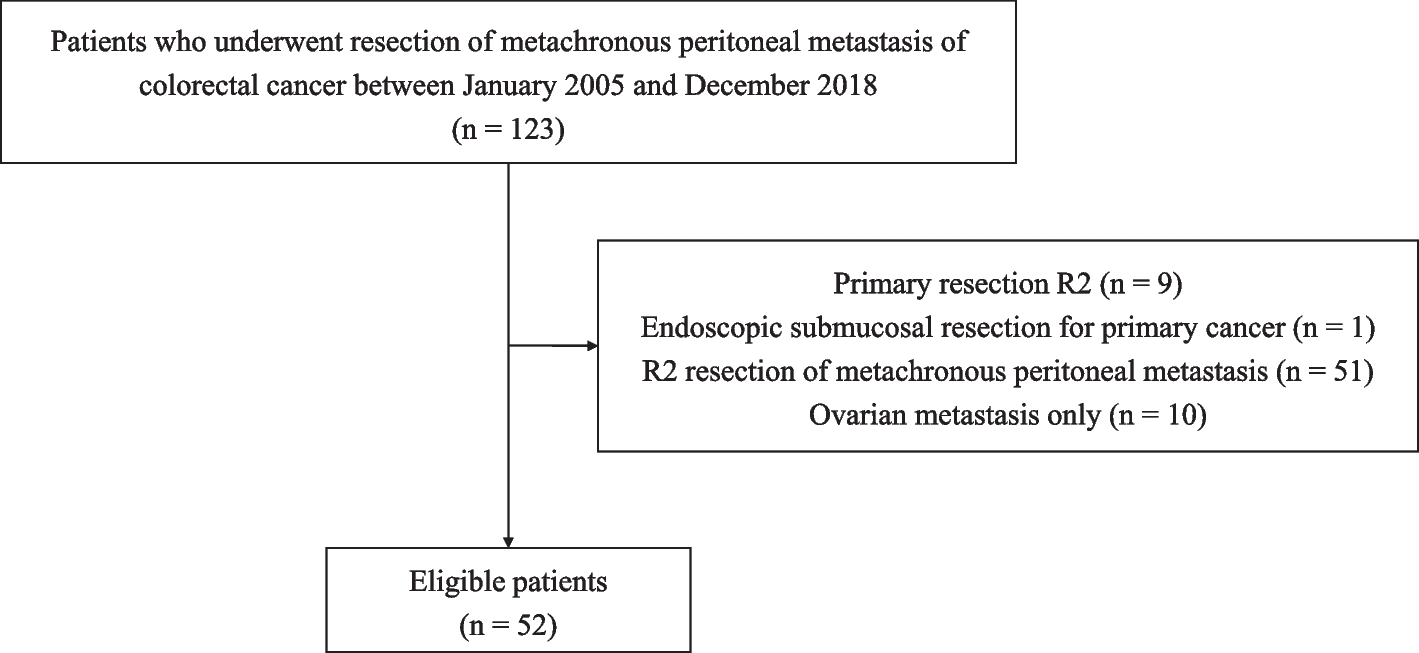

The initial search yielded 868 records, of which 348 duplicates were excluded. Following the review of titles, abstracts, and full-text articles, 27 potentially relevant studies were evaluated. Subsequently, after applying the inclusion criteria, a total of 24 studies [12, 14, 17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38] published in English and 3 studies [39,40,41] published in Chinese were included. Figure 1 illustrates the selection process, displaying the numbers of included and excluded studies. All titles, abstracts, and full texts underwent dual and independent review by the authors.
Fig. 1
The Flowchart of the Study
Study characteristicThis meta-analysis incorporated 27 studies focusing on the treatment of spinal tumors using TES surgery. There were 1135 patients (430 in the en-bloc resection group and 705 in the debulking group). Among those included studies, 22 studies [14, 17,18,19, 21, 22, 24,25,26, 28,29,30,31,32,33,34,35,36,37,38, 40, 41] reported primary spinal tumors, while 5 studies [12, 20, 23, 27, 39] focused on the spinal metastases. The main basic characteristics of the included literature were shown in Table 1.
Table 1 Basic characteristics of the included literatureThe bias risk assessment results of the included studiesIn the retrospective analysis, the NOS scale was employed to assess bias risk. Most of the included studies fulfilled the quality assessment criteria, with 20 studies collectively achieving scores ≥ 6, suggesting a low bias risk. Nonetheless, six articles scored below 6 overall, indicating a high risk of bias. Detailed information can be found in Table 2.
Table 2 Results of quality assessment using Newcastle–Ottawa scale for cohort studiesMeta-analysis resultsRecurrence rateA total of 25 studies, including references [12, 17,18,19,20,21,22,23,24, 26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41], provided data on recurrence rate. The analysis revealed no significant heterogeneity (P = 0.39, I2 = 0%), indicating a consistent pattern among the studies. Consequently, a fixed effect model was employed to assess the data. The findings demonstrated that patients who underwent en-bloc resection had a significantly lower recurrence rate compared to those who underwent debulking surgery (OR = 0.19, 95%CI: 0.13–0.28, P < 0.00001, as shown in Fig. 2). Furthermore, subgroup analysis indicated that en-bloc resection is particularly effective in reducing recurrence rate for both primary spinal tumors and spinal metastases (respectively; P < 0.00001 and P < 0.00001).
Fig. 2
A forest plot of recurrence rate
Mortality rateA total of 11 studies, referenced as [12, 18, 21,22,23, 27, 29, 33, 35, 38, 39], provided data on mortality rate. The analysis revealed no significant heterogeneity among the studies (P = 0.82, I2 = 0%). Therefore, a fixed effect model was applied to analyze the data. The results indicated that patients who underwent en-bloc resection had a significantly lower mortality rate compared to those who underwent debulking surgery (OR = 0.11, 95%CI: 0.06–0.22, P < 0.00001, as shown in Fig. 3). Furthermore, our subgroup analysis highlighted that en-bloc resection was associated with reduced mortality rate for both primary spinal tumors and spinal metastases (respectively; P < 0.00001 and P < 0.00001).
Fig. 3
A forest plot of mortality rate
Postoperative metastasis rateA total of 7 studies, referenced as [18, 21, 23, 33, 35, 38, 40], provided data on postoperative metastasis rate. The analysis revealed no significant heterogeneity among the studies (P = 0.93, I2 = 0%). Consequently, a fixed effect model was utilized for the analysis. The meta-analysis results indicated that patients who underwent en-bloc resection had a lower postoperative metastasis rate compared to those who underwent debulking surgery (OR = 0.30, 95%CI: 0.14–0.64, P = 0.002, as shown in Fig. 4). Subgroup analysis further revealed that en-bloc resection was associated with a lower postoperative metastasis rate for primary spinal tumors; however, when considering metastatic tumors specifically, en-bloc resection did not demonstrate superiority over debulking surgery in reducing postoperative metastasis rate (respectively; P = 0.007 and P = 0.11).
Fig. 4
A forest plot of postoperative metastasis rate
Recurrence-free survivalA total of 9 studies, referenced as [18, 20, 25, 26, 28, 29, 35, 37, 38], provided data on RFS. The analysis revealed no significant heterogeneity among the studies (P = 0.36, I2 = 9%). Consequently, a fixed effects model was utilized for the analysis. The meta-analysis results indicated that patients who underwent en-bloc resection had a higher RFS compared to those who underwent debulking surgery (HR = 0.37, 95%CI: 0.17–0.80, P = 0.01, as shown in Fig. 5). Subgroup analysis further revealed that en-bloc resection was associated with a higher RFS for primary spinal tumors; however, when considering metastatic tumors specifically, en-bloc resection did not demonstrate superiority over debulking surgery in reducing RFS (respectively; P = 0.02 and P = 0.24).
Fig. 5 Overall survival
Overall survivalA total of 10 studies, referenced as [12, 14, 20, 23, 25, 27, 33, 35, 38, 39], provided data on the OS of patients undergoing en-bloc resection for spinal tumors. The analysis revealed no significant heterogeneity among the studies (P = 0.94, I2 = 0%), leading to the utilization of a fixed-effect model for the analysis. The pooled analysis indicated a clear superiority in OS for patients who underwent en-bloc resection (HR = 0.45, 95%CI: 0.32–0.62, P < 0.00001, as shown in Fig. 6), suggesting that en-bloc resection was more effective than debulking surgery in improving overall survival. Furthermore, a subgroup analysis was conducted which demonstrated that en-bloc resection resulted in higher OS for both primary spinal tumors and spinal metastases (respectively; P = 0.007 and P < 0.0001).
Fig. 6 1-year RFS and 5-year RFS
1-year RFS and 5-year RFSA total of 10 studies [18, 20, 23, 25, 26, 28, 29, 35, 37, 38
留言 (0)