
記住我

CEUS utilizes the injection of a contrast agent (Perflutren liquid microsphere in our study) in the involved breast. The agent is carried by the lymphatic channels to the first draining lymph-node in the axilla. Thus CEUS works on the same principles as used for intra-operative identification of sentinel lymph nodes using vital blue dye or a radio-isotope. Therefore the lymph node identified in the axilla on CEUS should be considered as the sentinel node for all practical purposes.
Perflutren comprises lipid coated microspheres filled with octafluoropropane gas. When exposed to ultrasound waves, the microspheres resonate and ‘echo’ strong signals back to the ultrasound machine. the other agent that has been used for purpose of CEUS is sulphur hexafluoride gas suspended as microbubbles in a liquid. The gas trapped in microbubbles is not soluble in body fluids or water. It is removed naturally from the blood through respiration.
The pattern of contrast enhancement, intensity, speed of enhancement and also washout are well defined parameters used for characterization of liver tumors and other solid organ tumors. Generally malignant tumors and metastasis in liver exhibit the following characteristics. Hypervascular metastasis and hepatocellular carcinoma exhibit hyperenhancement during the arterial phase while some metastasis appears as hypoenhanced or demonstrate a rim like enhancement in the arterial phase. Larger malignant lesions may show a disorganized internal vasculature which becomes more visible on CEUS studies than it does on non contrast enhanced CT or MRI [5].
Although there is a significant amount of overlap in enhancing characteristics of benign and malignant lesions, it is generally found that malignant lesions demonstrate heterogeneous or peripheral hyper enhancement with centripetal filling. Further as a consequence of neo angiogenesis and intra-tumoral arterio-venous shunting malignant lesions have a rapid wash in and wash outs [6]. A homogeneous enhancement is a reliable indicator of a benign breast lump.
In our study on the utility of CEUS for assessment of nodes in clinically negative axilla of breast cancer patients, we have attempted to extrapolate the previously described contrast enhancement patterns seen in liver tumors. Our study has shown that malignant lymph nodes had a greater propensity for heterogenous enhancement compared to benign nodes (67% vs. 15%). Three out of fifteen malignant lymph nodes (20%) did not exhibit contrast uptake probably due to necrosis in the node. Benign lymph nodes had more chances of being isoenhancing with comparison to surrounding breast parenchyma compared to malignant nodes (52% vs. 14%). As far as time taken to enhance, enhancement direction (centripetal or centrifugal) and feeding vessel we could find no difference between benign and malignant lymph nodes.
CEUS with conventional ultrasonogram has better diagnostic performance than conventional ultrasonogram alone. Both quantitative and qualitative CEUS parameters have been used to distinguish benign from malignant breast masses. Luo et al. (2016) described 10 different CEUS parameters and reported 3 different malignant predictive models and 3 benign models [7]. The parameters studied were contrast enhancement, direction of contrast uptake and speed of contrast uptake [8].
Quantitative parameters in CEUS which favor a malignant diagnosis are shorter time taken by micro-bubbles to reach peak enhancement and a higher peak intensity [9]. These findings are a consequence of neo angiogenesis, arterio-venous connections and higher micro vessel density seen in malignant lesions. Although the difference is statistically significant, there is a great deal of overlap and a clear cut-off value cannot be assigned for clinical practice.
Just like most of ultrasound reporting, interpretation of CEUS images is operator dependent. In hands of experienced sonologists CEUS has potential just like MRI to provide quantitative parameters as well as functional assessment through post processing including a time intensity curve [10]. CEUS has the potential to downgrade BIRADS 4 lesions using parameters such as presence or absence of enhancement, pattern of enhancement, mass margins and shape [11]. Benign lesions are more likely to be isoenhancing and have circumscribed margins while malignant lesions will demonstrate hyper enhancement (or no enhancement in case of necrosis) and have indistinct or reticulated margins. It has been proposed that oval masses with homogeneous enhancing pattern and circumscribed margins may be spared a biopsy procedure.
As mentioned above we believe that the axillary lymph node which is the first to take up micro bubbles on CEUS should be considered as the sentinel lymph node. If the ultrasound features are suspicious a guided FNAC can be obtained from this node. This will be following the concepts and principles of intra-operative harvesting and evaluation of the sentinel node. The added advantage of our proposed technique is that a sentinel node tissue diagnosis would be available before the surgery. This will greatly aid in treatment planning as well as patient counseling. The caveat to our proposal is that in patients who have a positive for malignancy report in pre-operative CEUS guided FNAC should be treated as such. However those who have a negative for malignancy report should be treated as an equivocal report and should be managed accordingly with a conventional intra-operative sentinel node biopsy if indicated.
Sever AR et al. used a similar technique of peri-areolar intradermal injection of micro-bubble contrast agent. Breast lymphatics were visualized by sonography and followed to the axilla to identify sentinel lymph node. A guidewire was deployed at the same time under ultrasound guidance to localize the sentinel node. The next day the patient underwent standard tumor excision and sentinel node biopsy using conventional radioisotope and blue dye technique. Among the fourteen patients found to have metastasis in sentinel lymph node it was found that the sentinel node was correctly identified by the CEUS and localized with guidewire before surgery [12].
Contrast Enhanced Ultrasound evaluation can be performed within 90 s. The microbubble contrast is well tolerated with few side effects. It can be performed in patients with renal failure who cannot undergo contrast CT scan. Also it can easily be done in those with metallic implants or pacemakers when MRI is contraindicated or those who suffer from claustrophobia which can occur in CT scan or MRI machines. Thus our results show that CEUS can significantly improve the diagnostic value of ultrasound evaluation of the axilla in breast cancer patients.
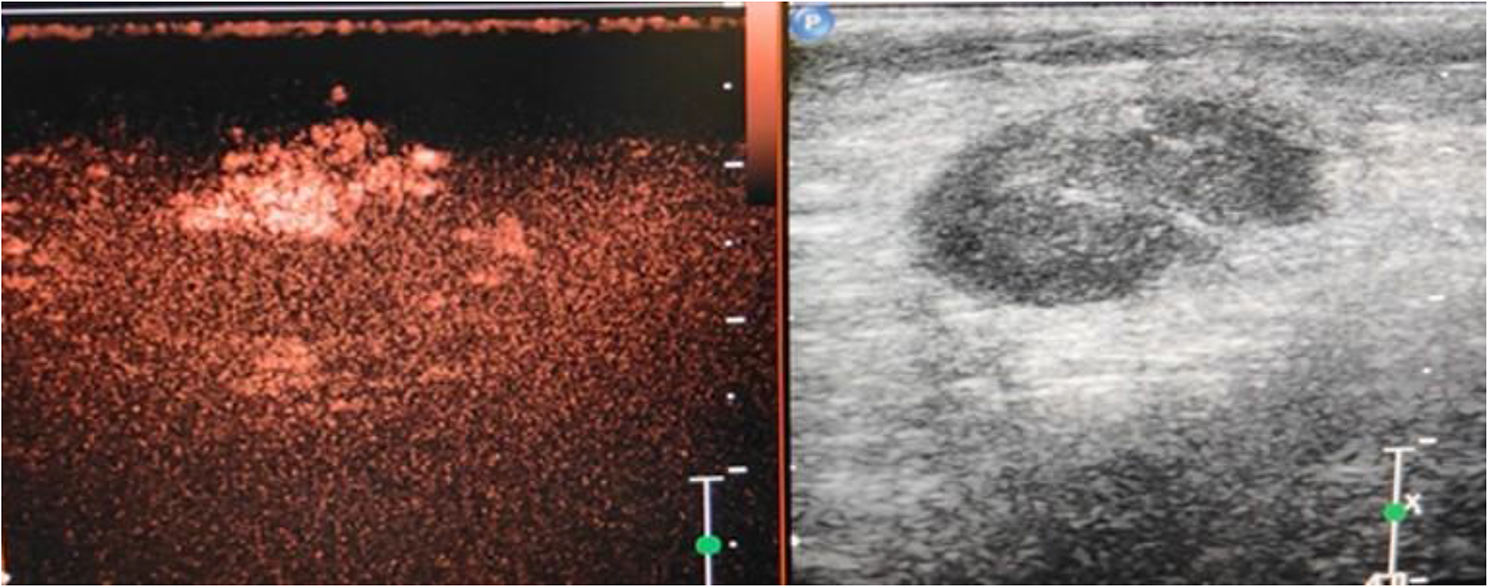
Fig. 1
Heterogenous enhancement of axillary lymph node on CEUS in a patient with a Breast Carcinoma:
Fig. 2
Homogenous enhancement of axillary lymph node on CEUS in a patient with Fibroadenoma:
留言 (0)