Cabanas’ work previously demonstrated that the sentinel lymph node (SLN) is the first lymph node to receive drainage directly from a tumor [1,2,3]. This is critical information, as tumor cells typically spread in a sequential manner from peritumoral lymphatics to the SLN, and then to more distant lymph nodes. Identification and biopsy of SLNs consequently became an ideal nodal staging method for many cancers, including breast [4,5,6,7]. More recently, the ACOSOG Z11 Study comparing axillary lymph node dissection (ALND) versus SLN dissection alone in women with T1 or T2 invasive primary breast cancer, no palpable axillary adenopathy, and 1 or 2 SLNs containing metastases showed no overall survival benefit for the ALND arm, even with long term follow-up [2, 8,9,10]. The status of the SLN is therefore important in deciding whether ALND is necessary, particularly in early stages, as noted by Bianchi et al. (1994) and Veronesi et al. (2003) [11, 12], usage of which decreased ALND-related lymphedema complications in nearly half of the patients to 1-2% [4, 13].
The concept of dual mapping was first described by Morton et al. in 1992 where cutaneous lymphoscintigraphy was used to identify SLNs for biopsy [5]. While the standard for identifying SLN for biopsy is a dual tracer technique, blue dye alone is also acceptable and can be readily employed in institutions with limited access to nuclear tracer [14]. In most developing countries, including Thailand, single blue dye tracer is predominantly used [15]. There are two main sites of dye injection: peritumoral and periareolar [16]. Each have their own disadvantages on specific surgical procedures [9, 17]. One of the most crucial drawbacks of peritumoral injection is discoloration of the surgical field from blue dye staining. This issue also affects nipple-sparing mastectomy (NSM) and skin-sparing mastectomy (SSM) procedures when the blue dye is injected periareolarly. Additionally, this technique can result in prolonged periareolar tattooing, a notable concern in these surgical contexts [18, 19].
According to Sappey et al.(1874), Rouviere(1938) and Grant et al. (1953) breast lymphatics originate as a dense network that lies in the interlobular connective tissue then follow the mammary ducts centripetally to the subareolar lymphatic plexus [5]. Efferent vessels from any quadrant of the breast pass to axillary nodes (75%) and the remainder drain principally to the internal mammary chain (25%) [20, 21]. Review of anatomical and clinical considerations led to a new concept of injecting the intraparenchymal blue dye at a quadrant other than of the index lesion. In the pilot study by Bianchi et al., 30 consecutive patients with clinically node-negative breast cancer, who had positive findings on mammograms and cytology, underwent SLNB using radioguided surgery and vital blue dye mapping. Initially, each patient received either a subdermal (ID) or peritumoral (IP) injection of a radiotracer above the tumor site to localize the first draining lymph node visible on either dynamic or static planar imaging. Then, a second injection of the radiotracer was given, with the site of injection varying for each patient. In the study, group 4 received an above-lesion ID and an IP injection in the opposite quadrant, while group 5 had both above-lesion ID and peritumoral IP [11]. Both resulted in no false SLNs which support the argument that intraparenchymal injection at any site may lead to the same SLN identification rate. Conventional periareolar injections do not change based on tumor location, whether in the periareolar area or any other quadrant. By the same token, this rationale may also apply to our new conceptual proposal that blue dye injection at any quadrant, even those not containing the index lesion, or periareolar injections should provide concordant outcomes to peritumoral injections. Changing the way we do these dye injections should benefit procedures such as lumpectomies, where periareolar injections would be preferred to peritumoral injections, and in NSM and SSM where the injection site should be remote to the periareolar region and to tumor to ensure a better visualization of the surgical field.
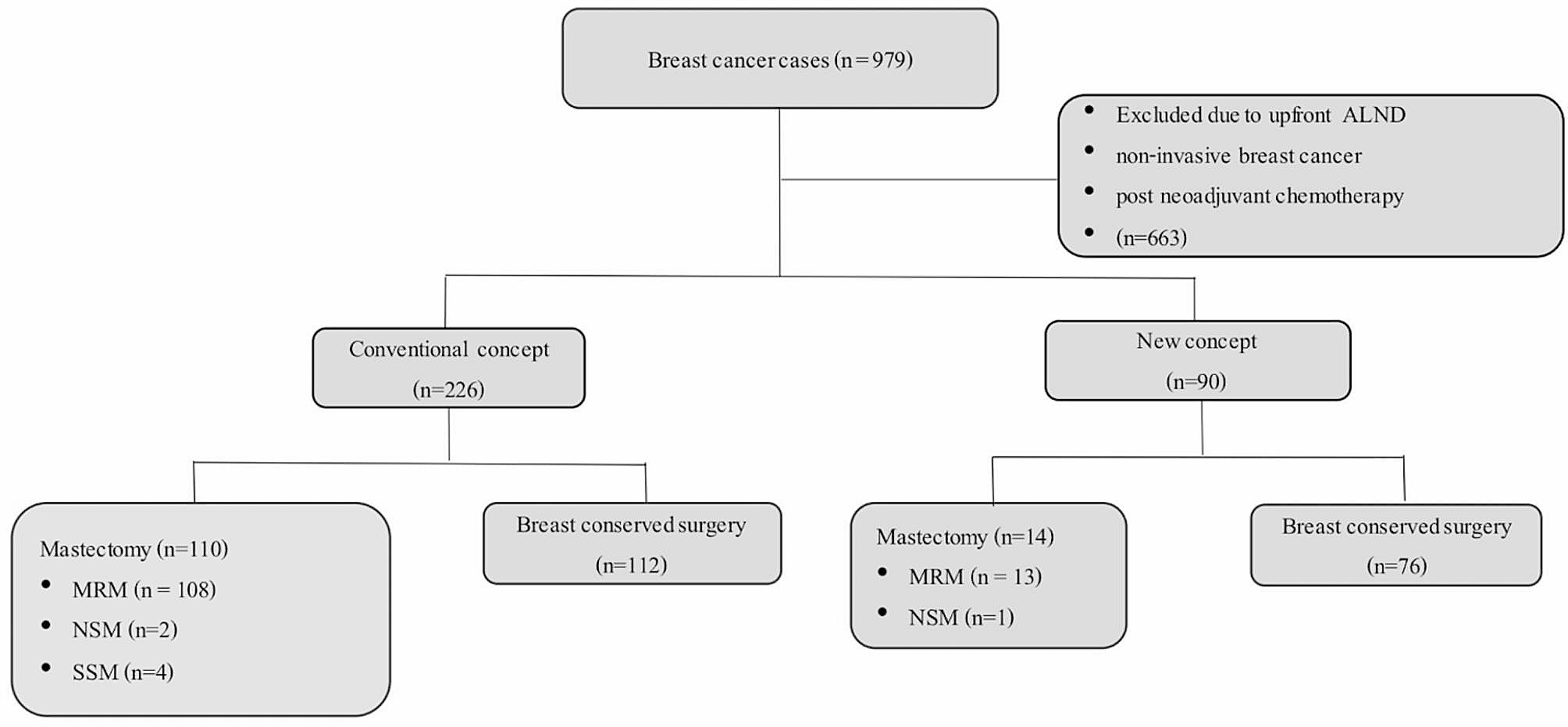
We carried out a retrospective review of patients who underwent breast conserving surgery (BCS) or mastectomy with sentinel lymph node biopsy (SLNB) over a period of 5 years to compare the rates of regional recurrence between the traditional approach and the novel injection concept. The secondary outcome was the mean distant-disease free survival duration. The mean disease-free survival, breast cancer specific survival, mortality rate and other sites of recurrence, local and systemic, and mean re-operation rate after BCS are also reported.


留言 (0)