
記住我


Exercise and early mobility are key components of clinical practice guidelines for patients with critical illness, as defined in the Intensive Care Unit (ICU) Liberation bundle [1]. However, findings from multiple randomized ICU rehabilitation trials have been equivocal, demonstrating minimal impact on mortality and physical function [2,3,4,5]. A potential explanation for the lack of benefits is a non-specific exercise dose. Patients are routinely randomized to “one-size-fits-all” protocols leading to heterogeneity in the response to treatment. Dosage that accounts for the frequency and intensity of exercise is frequently overlooked or not addressed in critical care practice and research. The rehabilitation dosage delivered in large randomized controlled trials (RCTs) is rarely implemented in clinical practice [6, 7], and patients seldomly receive a targeted or individualized dose of exercise. Patients with critical COVID-19 have not been studied to determine if dosage of exercise is related to outcomes. The COVID-19 pandemic may have unintentionally altered patterns in rehabilitation practice due to periods of isolation [8]. Thus, the primary objective of this study was to examine the relationship between physical rehabilitation parameters including an approach to quantifying dosage with hospital outcomes for patients with critical COVID-19.
DesignRetrospective practice analysis for patients hospitalized from March 5, 2020, to April 15, 2021.
SettingICUs at four academic medical institutions (University of Kentucky, Cleveland Clinic, University of Michigan, and University of Southern California).
Patients3780 adults (≥ 18 years of age) admitted to ICU with primary diagnosis of COVID-19.
InterventionsWe examined the relationship between ICU-based physical rehabilitation interventions and hospital-based outcomes. Outcomes included: (1) mortality; (2) discharge disposition; and 3) physical function at or near hospital discharge measured by the Activity Measure-Post Acute Care (AM-PAC) “6-Clicks” Inpatient Mobility Short Form (6–24, 24 = greater functional independence) [9]. Physical rehabilitation parameters included time to first rehabilitation (physical [PT] or occupational [OT]) session in days, number of PT and OT sessions completed during hospital length of stay (LOS), frequency of PT and OT (# of session/hospital LOS), mobility status during first three and the last recorded (if more than 3 sessions) rehabilitation sessions. Mobility levels were quantified by the John Hopkins-Highest Level of Mobility (JH-HLM, 1–8, 1 = lying in bed; 8 = ambulating > 250 feet). The physical rehabilitation dose was quantified as the average JH-HLM score over the first three sessions (a surrogate measure of early intensity) multiplied by the rehabilitation frequency (PT + OT frequency). The dose provides information on delivery of ICU rehabilitation such that patients who achieve high mobility with daily frequency of rehabilitation receive the highest dosage, whereas patients with lower mobility levels and infrequent rehabilitation receive the lowest dose. Our method is based on our previous published studies demonstrating that the mobility levels obtained in the first 3 rehabilitation sessions predict, or at minimum, associate with patient-centered outcomes [10, 11].
Measurements and main resultsDescriptive statistics were reported as mean ± SD, median [IQR], or n (%) as appropriate. A total of 3780 patients with COVID critical illness were included. Patients were stratified into groups according to discharge disposition (in-hospital death, subacute or long-term care facility, acute rehabilitation facility, home with services, or home independent). The change in mobility level during rehabilitation as measured by JH-HLM among discharge groups were compared using a two-way ANOVA. Dose of rehabilitation between discharge disposition groups were compared using Tukey’s multiple comparison test. Univariate analyses (Spearman’s correlation) were performed to assess associations between rehabilitation parameters and functional outcomes. Multivariate linear regression was performed to analyze the association between rehabilitation dose and discharge AM-PAC scores, which defined physical function among survivors, adjusting for pre-specified covariates including age, sex, body mass index (BMI), ICU length of stay, and receipt of mechanical ventilation.
Patient demographics are described in Table 1. The cohort was a mean 64 ± 16 years old, 41% female and mean BMI of 32 ± 9 kg/m2. Mechanical ventilation was required in 46% (n = 1739), and the median hospital LOS was 12 days (IQR 7–21). A total of 2200 (58%) and 1698 (45%) patients received at least one PT and OT session, respectively. The first rehabilitation session occurred 7.5 ± 8.0 days after ICU admission. Patients received PT at a frequency of 0.22 ± 0.14 days a week and OT at a frequency of 0.18 ± 0.11 days a week, equivalent to 2.8 rehabilitation sessions per week. Mobility levels on the JH-HLM scale generally increased from the first to last session (+ 0.93 ± 2.1). The mean JH-HLM score for all sessions was 4.6 ± 1.7; this suggests a likely ability to transfer from a bed to a chair but not stand for up to one minute. The mean dose of physical rehabilitation was 1.8 ± 1.3 units.
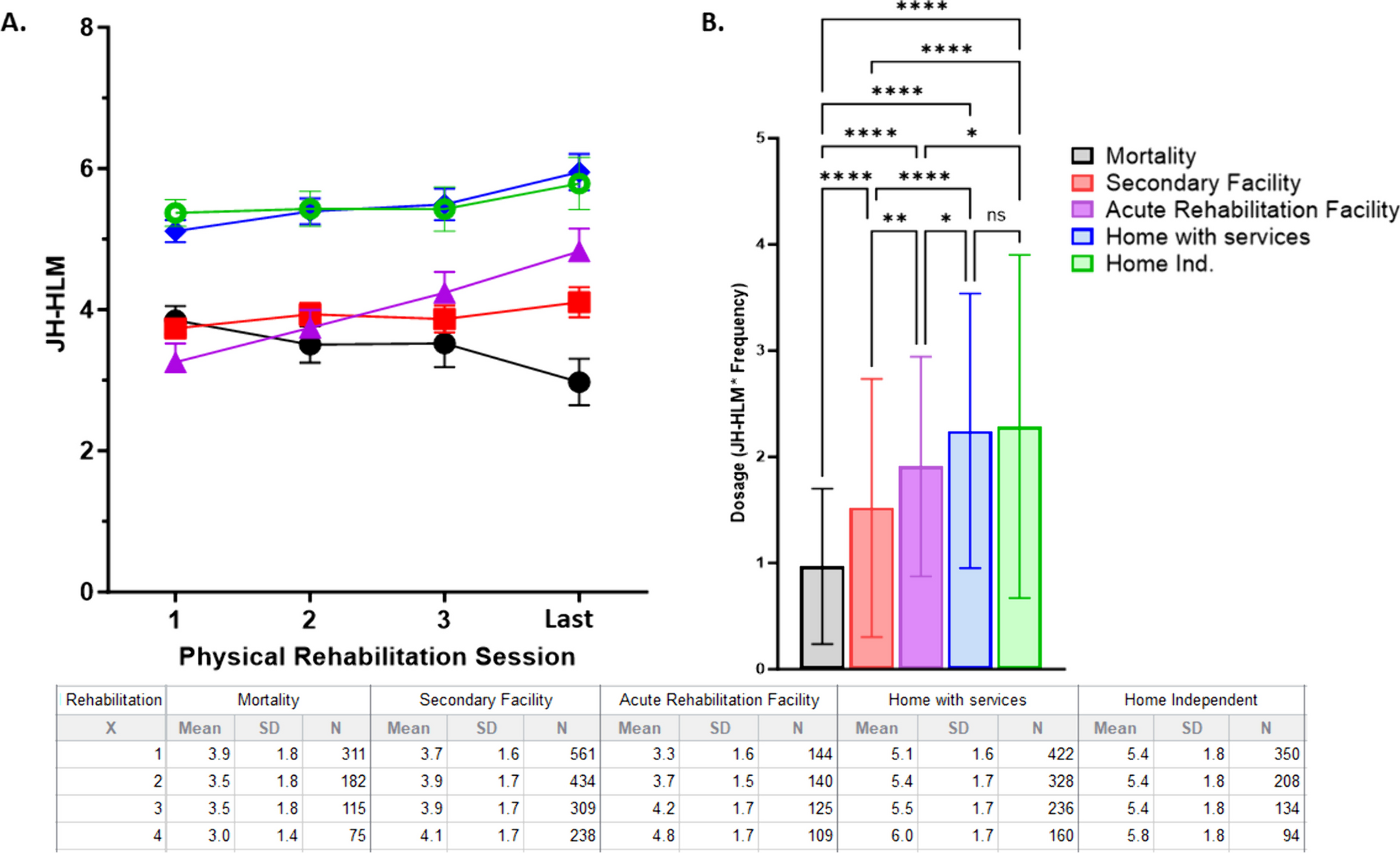
Table 1 Demographic, clinical and rehabilitation parametersPatients who died in the hospital (n = 994, 26%) were older, more likely to require mechanical ventilation, had longer durations of mechanical ventilation, less likely to receive PT or OT, and had longer ICU LOS (Table 1) compared to patients who survived to hospital discharge. Compared to survivors, those who died in the hospital had an earlier start of rehabilitation, but had lower frequencies of rehabilitation, achieved lower levels of mobility, and received a lower dose of physical rehabilitation (Table 1). Stratified by discharge disposition, patients discharged to home had the highest dose of rehabilitation (F = 69, p < 0.0001; Fig. 1).
Fig. 1
Dosage and change in mobility during physical rehabilitation grouped based on discharge disposition. A The change in mobility level measured by John Hopkins-Highest Level of Mobility (JH-HLM, 0–8) stratified by discharge disposition (black—mortality in hospital; red = secondary facilty; purple = acute rehabilitation facilty; blue = home with services; green = home without services). Two-Way ANOVA demonstrated significant difference in JH-HLM scores based on group (F = 240.8, p < 0.0001) and change over rehabilitation sessions (F = 11.13, p < 0.00) with interaction (F = 6.7, p < 0.0001). B The dosage of rehabilitation (JH-HLM average over four reported sessions multiplied by the frequency of rehabilitation) is significantly different based on discharge disposition (F = 69, p < 0.0001) with Tukey’s multiple comparison test revealing significant differences at the p < 0.0001 denoted with ****; p < 0.001 denoted with **, and * denoting p < 0.05. C (Table) provides raw data for the mobility sessions during the first 3 (1–3) sessions and the last rehabilitation (4) stratified based on the discharge destination
For 2191 patients who received PT or OT treatment and functional data were available in the EMR, the mean AM-PAC scores at discharge were 15.6 ± 5.9; suggesting a high-level of assistance is needed for bed-to-chair transfers [12]. Rehabilitation dose and physical function as measured by AM-PAC at discharge were moderately, positively associated (Spearman’s rho [r] = 0.484, p < 0.001). AM-PAC at discharge was also significantly associated with average mobility achieved in first 3 sessions (r = 0.799, p < 0.001), change in mobility from first to last session (r = 0.445, p < 0.001), and PT and OT frequency with physical function (r = 0.130, p < 0.001). Multivariate linear regression (model adjusted R2 = 0.68, p < 0.001) demonstrates the receipt of mechanical ventilation (β = − 0.86, p = 0.001), average mobility score in first three sessions (β = 2.6, p < 0.001) and physical rehabilitation dosage (β = 0.22, p = 0.001) were predictive of AM-PAC scores at discharge when controlling for age, sex, BMI, and ICU LOS.
留言 (0)