Data source
This study is a pre-specified secondary analysis of ICU-RESUS, a parallel, hybrid, stepped-wedge, cluster randomized trial (ClinicalTrials.gov Identifier: NCT02837497) conducted in 18 United States (US) pediatric ICUs and pediatric cardiac ICUs across 10 clinical sites from October 1, 2016 to March 31, 2021. The ICU-RESUS trial analyzed the effectiveness of a physiology-focused cardiac arrest quality improvement bundle, including point-of-care training and cardiac arrest debriefing, on improving rates of survival to hospital discharge with a favorable neurologic outcome among pediatric IHCA patients. The methods and primary results have been previously published [12, 13]. The institutional review board at the University of Utah (Data Coordinating Center) and each clinical site approved the study with waiver of informed consent. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline (Supplemental Table 1) when writing our report [14].
Study population
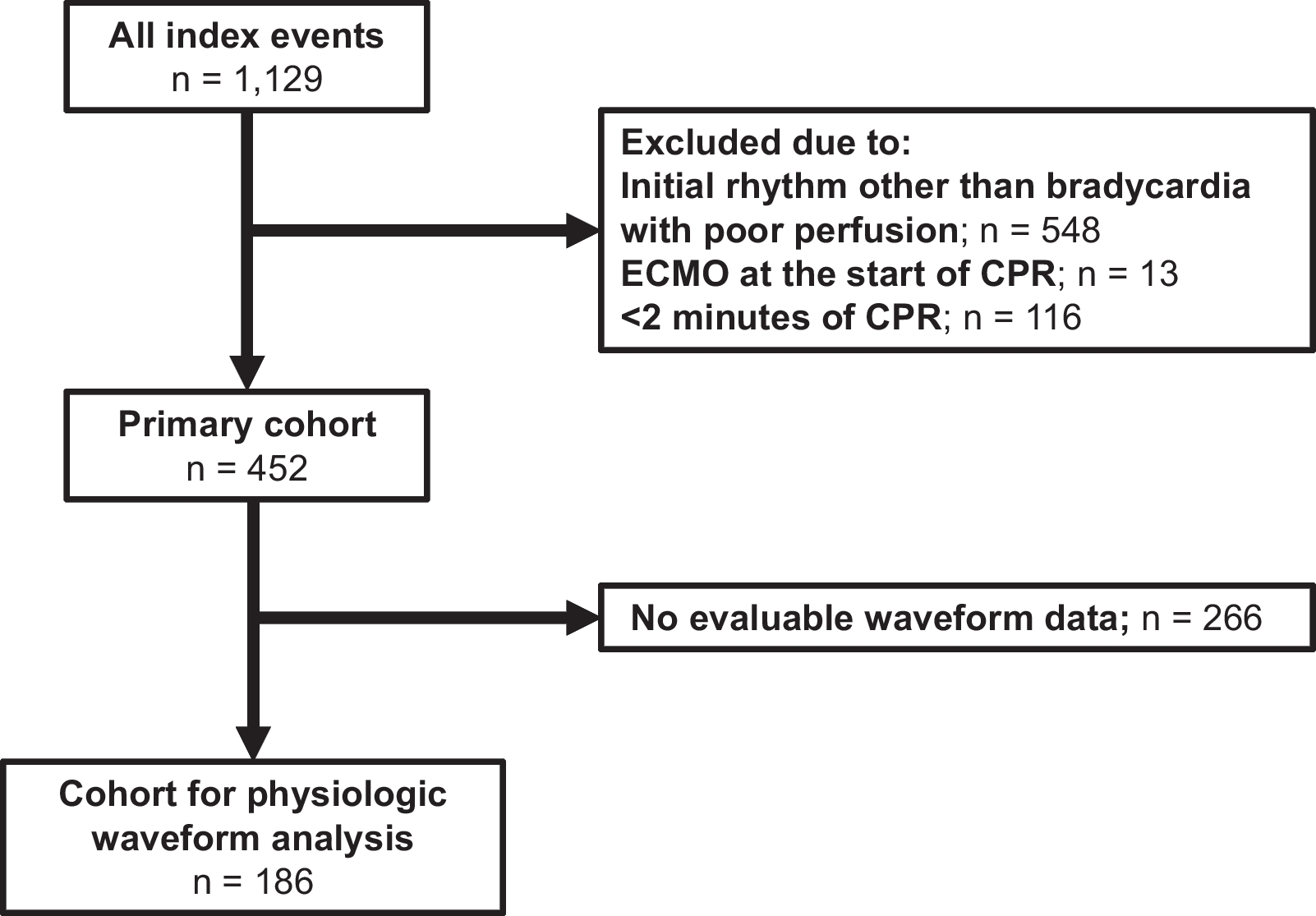
ICU-RESUS included index pediatric IHCA events occurring in children ≥ 37 weeks’ corrected gestational age and < 19 years of age who received chest compressions of any duration. Events were excluded if, prior to the arrest: (1) goals of care limited aggressive ICU therapies; (2) the patient was brain dead; or (3) the patient had an out-of-hospital cardiac arrest associated with the current hospitalization. For this secondary study, all included cases received chest compressions lasting ≥ 2 min and had an initial rhythm of bradycardia with poor perfusion documented by the clinical team. Two min was selected to exclude arrests with durations briefer than the window for our primary exposure. Patients were not required to receive epinephrine to be included. Patients receiving extracorporeal membrane oxygenation at the start of CPR were excluded. For inclusion in the subgroup analysis for the incidence and time course of the development of pulselessness based on invasive blood pressure (BP) waveform data, patients were required to have evaluable intra-arrest arterial BP waveforms.
Data collection and study variables
Utstein-style data were collected at each study site by trained research coordinators, including patient demographics, pre-arrest characteristics, and event characteristics [15]. Baseline Pediatric Cerebral Performance Category (PCPC) scores and Functional Status Scale (FSS) scores were determined based on the subject’s status prior to the event leading to the current hospitalization [16, 17]. For subjects born during the current hospitalization or that had been hospitalized longer than 90 days at the time of the arrest, baseline PCPC and FSS were assessed based on the subject’s status prior to the decompensation associated with the cardiac arrest. Determination of initial CPR rhythm was based on the clinical team’s documentation. The vasoactive-inotropic score (VIS) was calculated 2 h prior to cardiac arrest [18, 19]. The Pediatric Risk of Mortality (PRISM) III score was determined 2–6 h prior to cardiac arrest [17]. For children with invasive arterial catheters in place, physiologic waveforms were collected for up to the first 10 min of CPR, de-identified, and transmitted to investigators at the Children’s Hospital of Philadelphia [20].
Association between early epinephrine and outcomes
The primary exposure was “early” bolus-dose epinephrine, which was defined as epinephrine administration during the first 2 min of CPR. Epinephrine given within the first 2 min of CPR was selected a priori because the American Heart Association’s Get With The Guidelines—Resuscitation (GWTG-R) registry data indicate: (1) median time to epinephrine during pediatric IHCA is 1–2 min; and (2) children who develop subsequent pulselessness during CPR for an initial rhythm of bradycardia with poor perfusion do so at a median of 3 min [6, 8, 9]. By choosing epinephrine administration within 2 min as the primary exposure, we aimed to limit the number of events in the cohort with subjects who were already pulseless at the time they received epinephrine. The group that did not receive early bolus-dose epinephrine included events during which: (1) no epinephrine was administered or (2) the first dose of epinephrine was administered > 2 min after the start of CPR. The primary outcome was survival to hospital discharge with a favorable neurologic outcome, which was defined as a PCPC score of 1 (normal), 2 (mild disability), 3 (moderate disability), or no change from baseline. Exploratory outcomes included survival to hospital discharge, an alternative definition of survival to hospital discharge with a favorable neurologic outcome (defined as a PCPC score of 1, 2, or no change from baseline), and, among survivors, FSS score, PCPC at discharge, new morbidity (defined as an increase in FSS of 3 or greater from baseline to hospital discharge), and change from baseline FSS.
Patient and event characteristics were summarized according to whether early epinephrine was given. Frequencies and percentages were reported for categorical variables and medians and quartiles for continuous variables. Associations of summarized variables with early epinephrine were examined using Fisher’s exact test for categorical variables and the Wilcoxon rank-sum test for continuous variables. Patient and event characteristics and outcomes were also summarized based on CPR duration, comparing those events excluded due to CPR duration < 2 min to those with a CPR duration ≥ 2 min.
The associations between early epinephrine and outcomes were further investigated with Poisson regression with robust error estimates for binary outcomes and with ordinary linear regression for continuous outcomes. Covariates were selected a priori based on hypothesized or previously demonstrated associations with both administration of early epinephrine and the primary outcome. These included illness category (medical cardiac, medical non-cardiac, surgical cardiac, surgical non-cardiac, trauma), PRISM III score, VIS 2 h prior to CPR, presence of an epinephrine infusion at the start of CPR, hypotension as an immediate cause of the arrest, and respiratory decompensation as an immediate cause of the arrest [21,22,23]. Each of these covariates were individually included in the Poisson and linear regression models. Subgroup analyses using the same co-variates were conducted for: (1) patients with hypotension (and not respiratory decompensation) as an immediate cause of their arrest; (2) patients with respiratory decompensation (and not hypotension) as an immediate cause of their arrest; (3) patients with a cardiac illness category; and (4) neonates, as we hypothesized that epinephrine administration practices and response may differ in these subgroups.
Invasive blood pressure waveform analyses
Investigators at the Children’s Hospital of Philadelphia (KG, RMS, RWM) reviewed arterial BP waveforms from the first 10 min of CPR as previously described [12, 20]. For the present study, the CPR rhythm during each interruption in chest compressions was evaluated and classified. Among the sub-group with invasive BP monitoring, CPR rhythm during interruptions was defined as ‘pulseless’ when there was either no deflection in the arterial waveform indicating a native beat or there was a native beat with a systolic BP (SBP) below the threshold at which a clinician would be expected to feel a pulse (i.e., pulseless electrical activity). These thresholds were set at SBP < 40 mmHg for infants (< 1 year of age) and < 50 mmHg for children ≥ 1 year of age [7, 11, 12, 20]. The CPR rhythm was classified as “non-pulseless” (i.e., bradycardia with poor perfusion) if during the interruption there was an arterial waveform deflection with SBP above the threshold for pulselessness. Due to the brevity of some interruptions, heart rate was unable to be calculated and therefore was not considered in characterizing CPR rhythms during chest compression interruptions. Each 30-s CPR epoch was classified as: (1) ongoing CPR for bradycardia with poor perfusion; (2) ongoing CPR for a pulseless rhythm; (3) ROSC; (4) transition to extracorporeal support; or (5) death. A stacked band plot was generated to visualize the CPR rhythms/outcomes of the cohort over the first 10 min of CPR. A sensitivity analysis was performed with events divided into those that received early epinephrine and those that did not.
Association between subsequent pulselessness and outcomes
The primary exposure for this subgroup analysis of patients with invasive BP monitoring was the development of subsequent pulselessness during CPR initially provided for bradycardia with poor perfusion. Events were divided into three groups: (1) those with an initial rhythm of bradycardia with poor perfusion who did not develop pulselessness during the first 10 min of the CPR event; (2) those who did develop pulselessness; and (3) those who developed pulselessness and subsequently had at least one return to bradycardia with poor perfusion. The primary outcome for this analysis was sustained ROSC. Exploratory outcomes included survival to hospital discharge and survival to hospital discharge with a favorable neurologic outcome. Associations were measured using Fisher’s exact test for categorical variables and Kruskal–Wallis test for continuous variables. A sensitivity analysis was performed with events categorized by early epinephrine status.
All analyses were performed using SAS 9.4 (SAS Institute; Cary, NC). Reported p-values were based on a two-sided alternative and considered significant if less than 0.05.



留言 (0)