
記住我
Our study was conducted on patients with IBD who were split into two treatment groups, IFX and ADA, in a prospective, parallel, randomized manner. The study assessed trough concentrations of IFX and ADA, sTREM-1 level, CRP levels, CDAI, and DAI score. Trough concentrations of IFX and ADA were assessed after 14 weeks of starting treatments. Then Patients were further followed up for 2 months. Follow-ups were performed via scheduled hospital visits and phone calls for all enrolled patients.
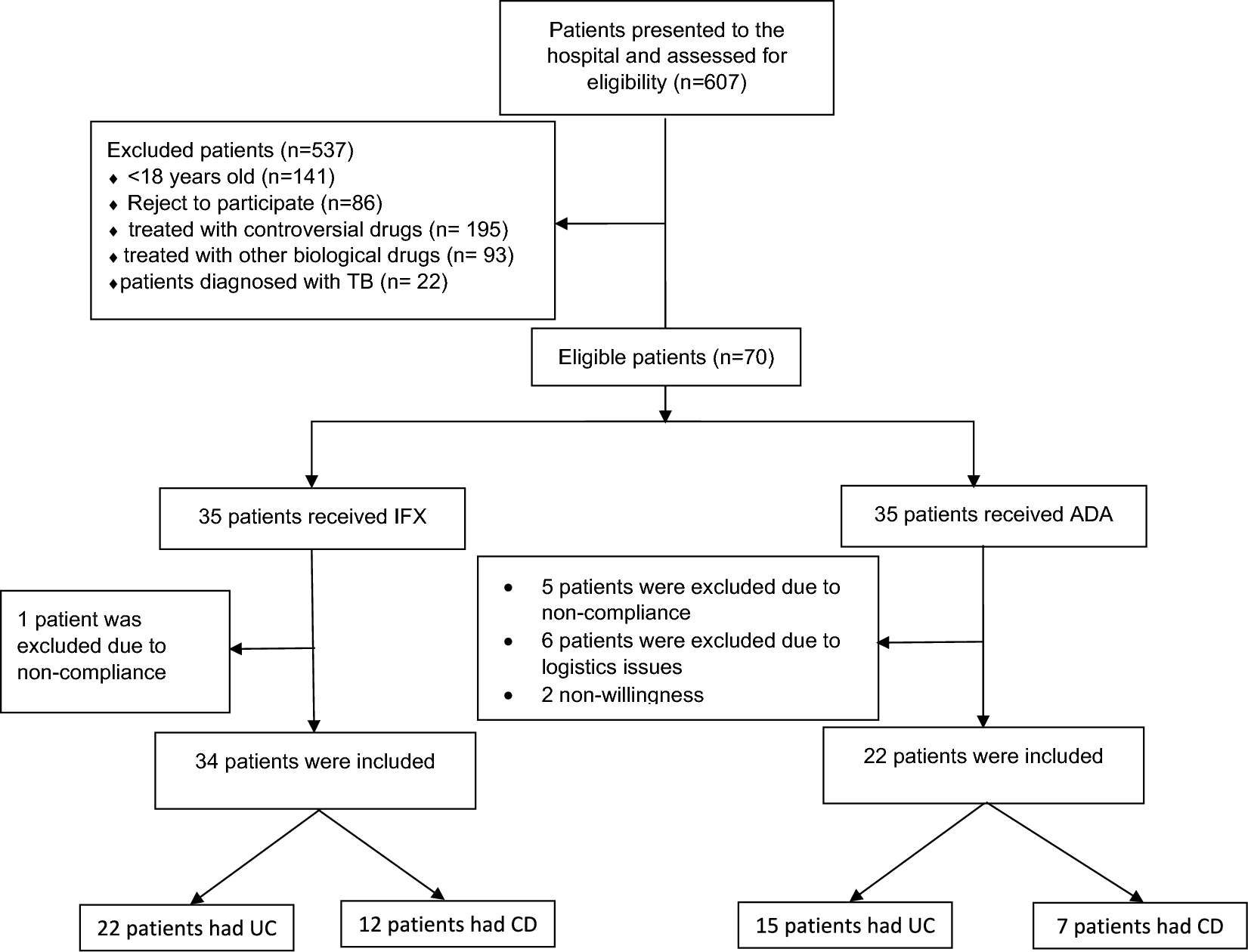
Study population and eligibilityAll patients with IBD were selected from the Outpatient Clinic at Ain Shams University Hospitals in Cairo, Egypt, and were evaluated for eligibility. The criteria for inclusion and exclusion can be found in Table 1. Six hundred and seven patients presented to the clinic. Eligible patients were randomly assigned based on the appointment number.
Table 1 Inclusion and exclusion criteriaAll eligible patients were asked to provide a written informed consent for participation in the study. Figure 1 is a flow diagram for the patients included in the study.
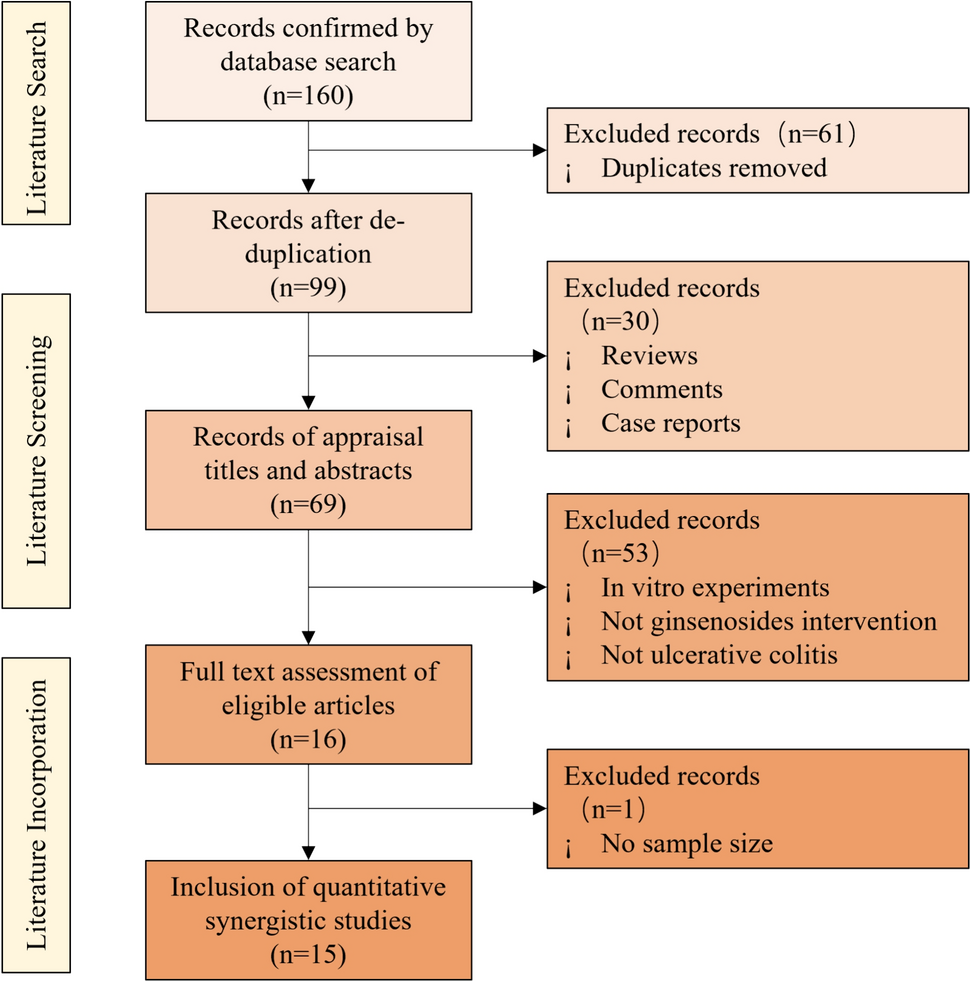
Fig. 1
Flow diagram for the IBD patients included in the study. UC ulcerative colitis, CD Crohn’s disease, TB Tuberculosis
InterventionThe loading dose of ADA (Humira®, AbbVie pharmaceuticals, North Chicago, USA) is 160 mg subcutaneously, given either as 4 injections of 40 mg on the first day or as 2 injections of 40 mg daily for 2 consecutive days, followed by a dose of 80 mg subcutaneously 2 weeks later. The maintenance dose is 40 mg subcutaneously every 2 weeks.
For IFX (Remicade®, Janssen Biotech pharmaceuticals, Horsham Township, Pennsylvania, USA), the loading dose is 5 mg/kg intravenously at 0, 2, and 6 weeks, with a maintenance dose of 5 mg/kg intravenously every 2 months.
In patients previously treated with biologic drugs there were washout periods of 4 weeks in the case of IFX and 5 weeks in the case of ADA or golimumab (Han et al. 2020).
ComplianceDuring the trial, a clinical pharmacist monitored compliance by ensuring patients received their scheduled doses at each visit. In addition, two phone calls were made to follow up with the patients. A colonoscopy was performed at baseline and week 14, using Olympus® CF-H180, Japan, to assess the patient’s condition in both treatment groups.
Assessment planBaseline assessments included patient history and current symptoms, CRP levels, CDAI, DAI, and colonoscopy. At week 14, CRP, CDAI, DAI, and colonoscopy were reassessed for all patients. sTREM-1 and trough concentration levels of IFX and ADA were also assessed at week 14. Patients were further followed up for 2 months for any side effects.
Primary endpointAssessment of efficacy was performed according to; trough concentrations of IFX and ADA, CRP, CDAI score, DAI score, and serum TREM-1 for all included patients.
Determination of trough concentrations of the biologic drugs (infliximab and adalimumab) and level of soluble triggering receptor expressed on myeloid cells-1 in the serumAfter 14 weeks of treatment with either IFX or ADA regimens, blood samples (5 ml) were collected before the next dose (trough concentration). Serum trough concentration of IFX and ADA were measured using ELISA kits (RIDASCREEN® IFX Monitoring, R-Biopharm AG®, Darmstadt, Germany, and RIDASCREEN® ADA Monitoring, R-Biopharm AG®, Darmstadt, Germany, respectively). The serum TREM-1 was measured using the Human Triggering Receptor Expressed on Myeloid Cells-1 ELISA Kit (Bioassay Technology Laboratory, Shanghai, China). ELISA kits were used according to the manufacturer’s rules.
Determination of efficacy by crohn’s disease activity indexPatients diagnosed with moderate to severe active CD underwent treatment with either IFX or ADA and were assessed for effectiveness using the CDAI. Clinical response (CR) was evaluated based on CR-70 and CR-100 criteria, signifying a decrease of at least 70 points and 100 points, respectively in CDAI scores from the initial assessment (Han et al. 2020).
Determination of efficacy by mayo score/disease activity indexThe CR was determined by a decrease of at least 3 points and 30% from the initial Mayo score, as well as a decrease of at least 1 point in the rectal bleeding sub-score or reaching an absolute rectal bleeding sub-score of 0 or 1 (Kamat et al. 2019).
Secondary endpointAny adverse effect was recorded during the follow-up visits or calls for the included patients in both regimens as summarized in Table 2.
Table 2 Side effects in IFX and ADA treatment groupsStatistical analysis and sample sizeStatistical analysis was conducted using the Statistical Package of Social Sciences (SPSS) software version 20. A normality test was carried out for continuous variables. If the data was normally distributed, paired samples t tests were used to compare the mean and standard deviation before and after treatments. Unpaired t tests were used for comparisons between groups. Otherwise, non-parametric data was compared using the Mann–Whitney U test and the Wilcoxon signed-rank test. For non-parametric data, patient demographics and baseline characteristics were described using descriptive statistics. Continuous variables were presented as means ± SD, while categorical variables were presented as frequencies and percentages. The Chi-square test was used to compare responses between the two treatment groups for categorical data. The level of significance was considered significant when P values < 0.05.
Ethical considerationsThe trial had no impact on the patient’s treatment or follow-up.
Trial statusThis study followed the ethical guidelines outlined in the Declaration of Helsinki and the obtained approval from the Faculty of Medicine at Ain Shams University Hospitals, and Damanhur University—Faculty of Pharmacy—Research Ethics Committee with an ethical approval number FMASU R175/2023 and 923PP68M, respectively. The study is registered on ClinicalTrials.gov with the identifier NCT05291039. Participants in the study provided informed consent to participate. (First Posted: March 22, 2022). Visit the study page at: https://clinicaltrials.gov/study/NCT05291039. Patients’ inclusion began in December 2021 and ended in March 2023.
留言 (0)