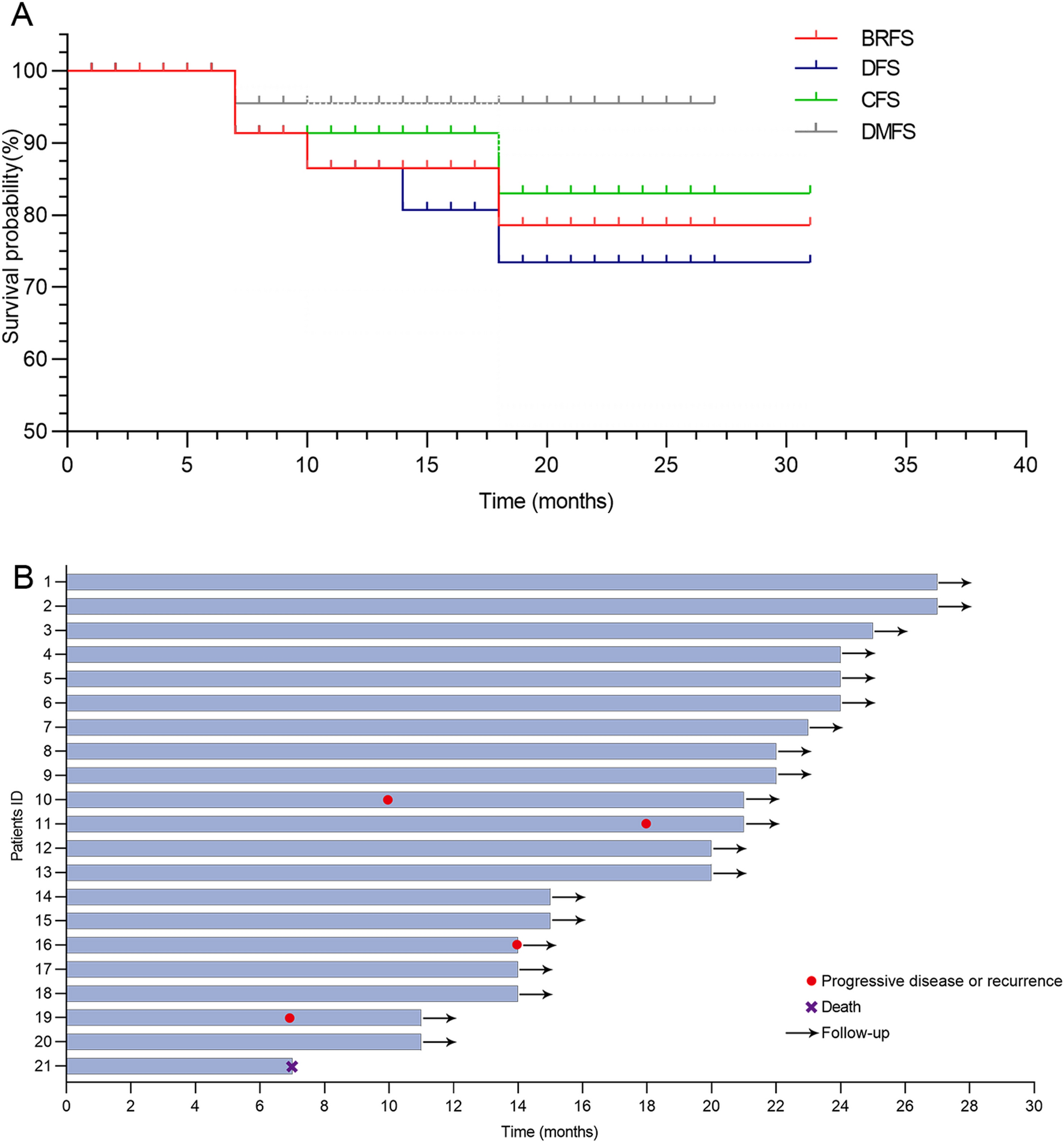
To our knowledge, this is the first study to evaluate the application of tislelizumab-based combination regimen in bladder-sparing strategies against HR-NMIBC. Overall, the combination regimen of tislelizumab plus BCG with or without chemotherapy yields promising clinical outcomes with 1-year BRFS rate of 86.50%, 2-year BRFS rate of 78.64%, 2-year CFS rate of 83.00%, and 2-year DFS of 73.39%. In addition, the safety profile of this regimen is tolerable and manageable. This regimen may be considered a clinically active non-surgical treatment option in this difficult-to-treat population.
HR-NMIBC is a difficult-to-treat disease with few approved therapeutic options and its management is one of the most challenging issues in the urological community [2]. TURBT followed by intravesical instillations with BCG is recommended by guidelines from European Association of Urology and American Society of Urologic Oncology for HR-NMIBC patients who have strong desire for bladder-sparing treatments or have comorbidities that preclude them from RC [16, 17]. However there are several contemporary problems with the use of BCG, such as high recurrence rates of 80% for patients who receive BCG, up to 45% of patients develop MIBC within 5 years, and ongoing BCG shortages in many countries raise concerns [18]. An accumulating body of evidence suggests that in the era of immunotherapy, high tumor mutational burden (TMB), DNA damage-response mutations, the presence of genomic instability, and high PD-L1 expression make bladder cancer suitable for immunotherapy [19]. The spotlight on immunotherapeutic strategies for bladder cancer is intensifying. In the KEYNOTE-057 trial, pembrolizumab monotherapy has shown promising results in the treatment of high-risk BCG-unresponsive NMIBC, with a complete response rate (CR) of 41% at 3 months after a median follow-up 36.4 months [7]. Consequently, pembrolizumab has received approval for the treatment of BCG-unresponsive NMIBC patients. Another study similarly reported a favorable CR rate of 41.7% at 6 months with atezolizumab monotherapy in BCG-unresponsive NMIBC patients [20].
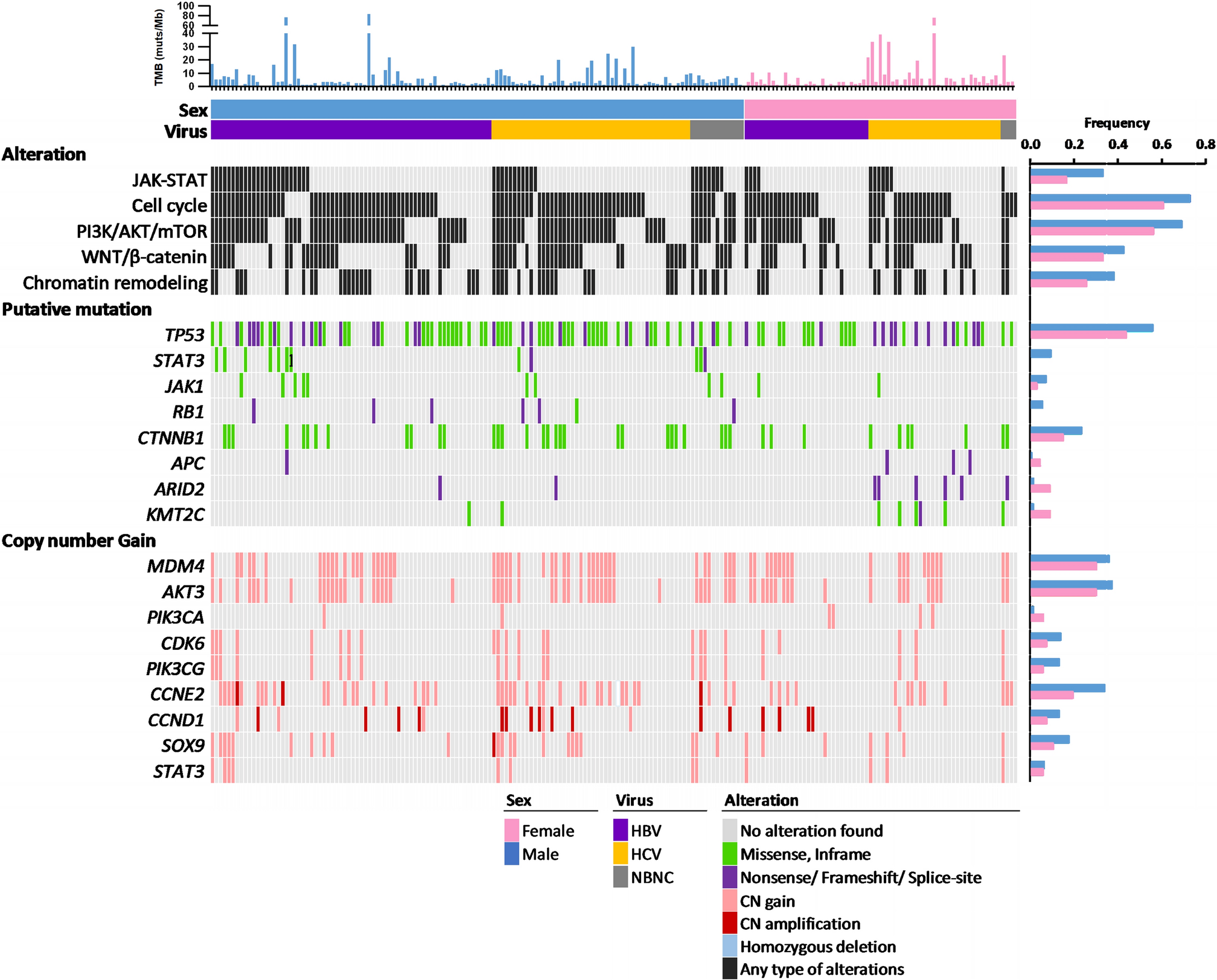
Studies have shown that PD-L1 and PD-1 expression is associated with BCG immune-resistance [10, 21]. BCG instillation seems to induce the expression of PD-L1 in tumor and inflammatory cells through the induction of CD8+ T cells, which are the major responsible for IFN-γ (which is associated to a BCG-unresponsive state) production [22]. Pierconti et al. found that PD-L1 expression in tumor cells and in immune cells was higher in BCG-unresponsive bladder cancer patients than in BCG-responders, suggesting BCG itself could enhance PD-1 and PD-L1 [23]. This provides the grounds for trials that are testing anti-PD-1 or anti-PD-L1 antibodies in association with BCG as front-line therapy in NMIBC in BCG-naïve patients or in patients not reaching a CR after BCG induction [10, 21]. Inman et al. conducted a Phase 1b/2 study investigating the use of atezolizumab with or without BCG instillation in HR-NMIBC, and found a monotherapy CR rate of 33.3%, while the combination group achieved a CR rate of 42% [24]. Our study similarly supports this conclusion, indicating that the addition of immunotherapeutic agents to conventional treatment modalities can yield effective outcomes, reducing recurrence and progression. In our study, we observed a promising inhibition of disease progression and recurrence, with 1-year BRFS rate of 86.50%, a 2-year BRFS rate of 78.64%, and a 2-year DFS of 73.39%, which underscored the potential benefits of utilizing immunotherapeutic in the management of HR-NMIBC. Furthermore, for stage T1 patients, GC chemotherapy was performed to enhance the management of disease metastasis and recurrence. Chu et al. have revealed that patients with pathologic features of high grade T1 disease harbored more TP53, ERBB2/Her2, and RB1 mutations and a genomic profile more similar to T2 tumors than NMIBC, suggesting an increased risk of infiltration and metastasis [25]; Meanwhile, NCCN guidelines show that chemotherapy given after TURBT may prevent tumor cell implantation and recurrence in select subgroups of patients [26]. In addition, studies are demonstrating promising outcomes with single or combination chemotherapy agents (such as sequential intravesical gemcitabine and docetaxel, gemcitabine bladder instillation) in the treatment of HR-NMIBC, which has been shown to confer approximately 2-year BRFS of 57% [27] 2-year DFS of 30–40% [18, 28], and 2-year CFS of 79–86% [27, 29]. In comparison, our study shows improved results, particularly with numerically higher rate for 2-year BRFS (78.64%) and 2-year DFS (73.39%); additionally, our study stabilizes 2-year CFS at 83%. However, it is important to note that the majority of the aforementioned evaluations of chemotherapy treatment for HR-NMIBC stem from smaller series studies and retrospective analyses, necessitating careful consideration when extrapolating these findings.
Overall, compared with the above studies, the results in our study demonstrated the potential efficacy of this combination therapy of tislelizumab and BCG with or without chemotherapy, with a notable 76.2% of patients achieving disease stability, accompanied by a marked inhibition of recurrence. Notably, key outcome measures such as BRFS, CFS, and DFS reached a plateau with a prolonged “tail” approximately 2 years post-treatment initiation. In particular, is the behavior of DMFS, which not only entered a stable phase earlier than other parameters but has also consistently maintained this stable status. Although OS remains the gold standard for assessing oncological efficacy, the observation period for mature OS outcomes is often protracted [30]. Studies indicate that for bladder cancer patients undergoing platinum-based adjuvant chemotherapy, DMFS may serve as a potentially crucial surrogate endpoint for OS [31]. These findings in our study collectively emphasize the potential viability of the combination strategy involving tislelizumab and BCG with or without chemotherapy in HR-NMIBC, offering additional choices in the spectrum of treatment options for this patient cohort.
It is critical to consider the safety profile when patients receive potentially effective drug combination regimens. Overall, the tislelizumab combination regimen is generally well tolerated and manageable in our study. The TRAEs of any grade in our study was 66.67%, with grade ≥ 3 TRAEs occurring in 9.52%. Notably, the incidence of grade ≥ 3 TRAEs is lower than observed in other PD-1 studies, such as the Keynote 057 study (13%) and the SWOG S1605 study (approximately 17%) [7, 20]. The increased incidence of AEs is associated with chemotherapy-related factors such as nausea, vomiting, and renal dysfunction. Throughout the course of patient treatment, a multidisciplinary team (MDT) managed adverse reactions comprehensively, which included specialists from oncology, hematology, nephrology, gastroenterology, etc. Early detection and timely intervention by the MDT ensured patient safety.
Certain limitations of our study should be acknowledged. Firstly, our study is limited by its retrospective nature, hence, there exists a potential selection bias. Secondly, the sample size of this study was relatively small. Future studies should include a larger sample size, and randomized clinical studies should be conducted. Thirdly, there is a lack of long-term follow-up results. Long-term follow-up is needed to understand the long-term prognosis of patients. Finally, there is no uniform treatment protocol in our study, but some patients with a strong desire to preserve their bladder may intolerant to cisplatin-based chemotherapy based on clinical reality. There is a need to extend the sample size to classify patients into subgroups (with or without chemotherapy) in order to validate these preliminary findings and to better explore the optimal treatment options.

留言 (0)