
記住我
The retrospective study consisted of 195 HCC patients, including 129 males (66.2%) and 66 females (33.8%; ratio of male to female = 1.95) patients. The clinicopathological characteristics of this cohort are summarized in Table 1. The median age at diagnosis was 62 (ranging from 26 to 86), and most patients were diagnosed in the early stage (Stage I and II, n = 150, 76.9%). Ninety-eight patients (50.3%) and 80 patients (41%) had HBV and HCV infection history, which is much higher than the TCGA non-Asian cohort (5.1% and 20.1%, respectively; Supplementary Table S1). The proportion of patients with cirrhosis, alcohol, and smoking history was 39%, 34.9%, and 46.2%, respectively.
Table 1 Clinical characteristics of 195 HCC patients enrolled in the studyWe further explored the associations between the clinicopathological features and patients’ sex. Compared with female patients, significantly more male patients have drinking and smoking habits (51.2% vs. 3% and 66.7% vs. 6.1%, respectively; both P values are smaller than 0.0001). There is no difference in the age at diagnosis, stage distribution, viral infection history, and cirrhosis distribution between male and female HCC patients.
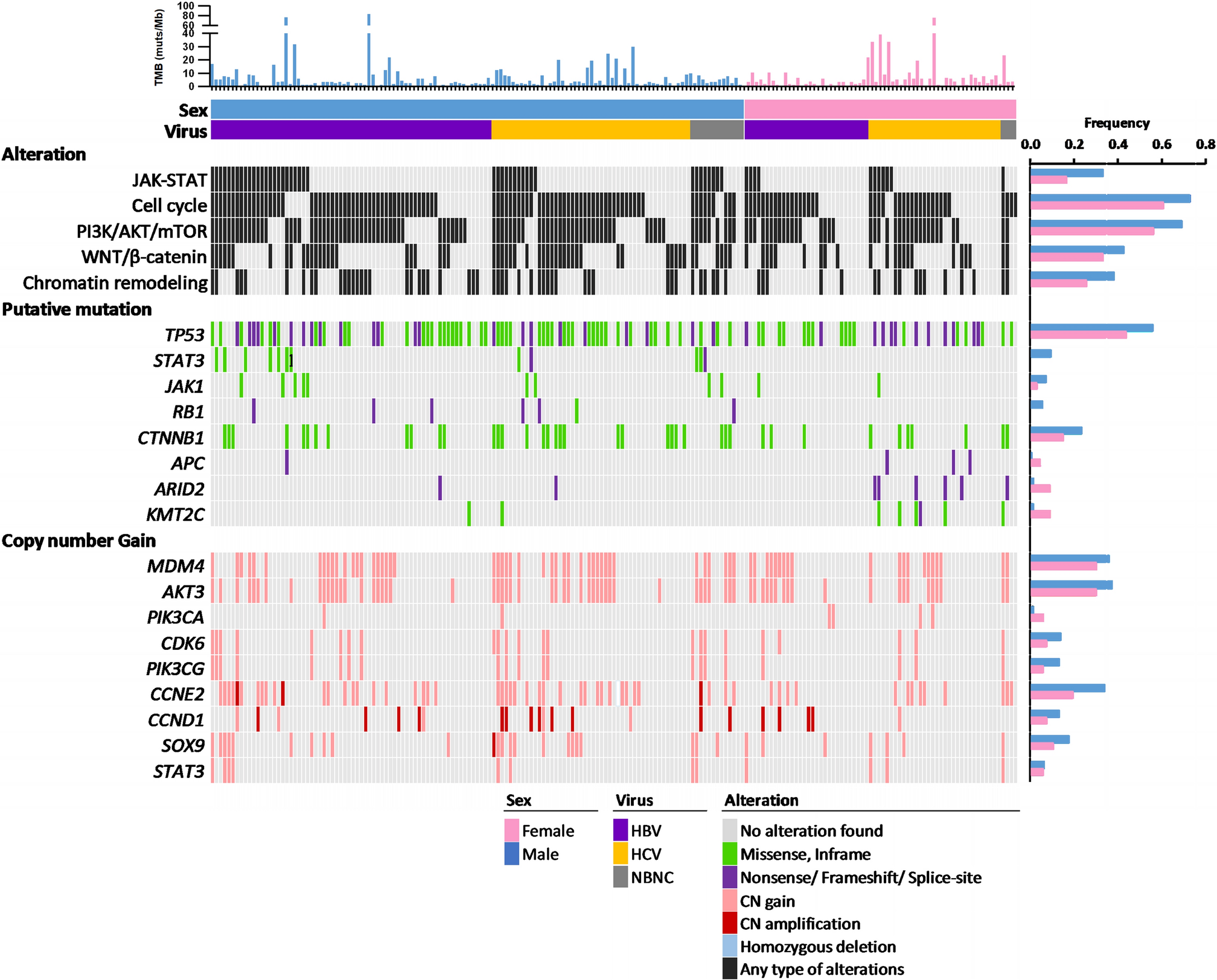
3.2 Mutational landscape in Taiwanese HCCThe extracted genomic DNA was analyzed by targeted DNA sequencing on 440 cancer-related gene coding regions. Among the 195 specimens, we identified 6,156 alterations, including 1819 mutations and 4337 CNVs (listed in Supplementary Table S2 excel file). The most frequently altered genes and signaling pathways are illustrated in Fig. 1. As expected, TP53 and CTNNB1 are the top two genes most mutated in HCC [38,39,40]. In addition, we found that ARID1A, ARID2, JAK1, and KMT2C genes are recurrently mutated in the Taiwanese HCC specimen (as shown in Supplementary Fig S1).
Fig. 1
Mutational profiles of HCC specimens according to sex in the Taiwanese population. Each column represents one patient. Genes involved in the same signaling pathways are grouped, and the mutation frequencies among males and females are shown in the right plots. Each sample’s TMB is shown in the upper panel. Colors specify different types of alteration
Among the 4337 CNVs, 4215 (97.2%) were classified as copy number gain or amplification, and 122 (2.8%) were homozygous deletion. Our results confirmed the previously well-defined recurrent CNVs in HCC, including recurrent gains on chr 1q21.1-q23.3 (encoding genes like BCL9, MCL1, NTRK1, DDR2, FCGR2B, and SDHC), chr 1q31.1-q44 (encoding genes like PTGS2, CDC73, IKBKE, BTG2, MDM4, PIK3C2B, USH2A, PARP1, FH, and AKT3), chr 8q21.3-q24.3 (encoding genes like NBN, RUNX1T1, CCNE2, UBR5, MYC, and RECQL4), and chr 17q22-25.3 (encoding genes like RNF43, BRIP1, CD79B, AXIN2, GNA13, PRKAR1A, SOX9, and RPTOR (as shown in Supplementary Fig S1).
3.3 Comparison of genomic profiles between genders in Taiwanese HCC patientsWe compared the alteration frequencies of commonly mutated genes in male and female patient subgroups to elucidate the difference in genomic alteration patterns between male and female HCC patients in Taiwan (as shown in Fig. 1). Our analysis, presented in Supplementary Fig S1–2, revealed no significant difference in TMB between the sexes or with the presence of the virus. Notably, while a substantial disparity in smoking history was observed between male and female patients, no difference in TMB was found (P = 0.4653). We also cross-referenced our findings with the TCGA HCC dataset, and similar results were observed, with no significant variations in TMB between sexes, virus presence, or smoking history, as demonstrated in Supplementary Fig S3.
Figure 1 illustrates that the prevalence of STAT3 mutations is higher in male patients compared to females (9.3% versus 0%, P = 0.0092). However, when we accounted for multiple comparisons, the difference did not maintain statistical significance (adjusted P = 0.135; Benjamini–Hochberg correction; Supplementary Table S4). We also investigated the mutation frequency of CTNNB1, a gene known for its sex-biased mutation pattern in liver hepatocellular carcinoma [24]. In the Taiwanese cohort, we observed mutation frequencies of CTNNB1 in male and female HCC patients at 23.3% and 15.2%, respectively. However, these differences did not demonstrate statistical significance after adjustment (adjusted P = 0.520; Benjamini–Hochberg, Supplementary Table S4).
When analyzing copy number variations (CNVs) as depicted in Fig. 1 and Supplementary Fig S1, we found that more male patients harbored copy number gains of the 8q22.1 encoding the CCNE2 gene, in comparison to females (34.9% vs. 19.7%; P = 0.038). However, this difference was no longer statistically significant after adjusting for multiple comparisons (adjusted P = 0.717; Benjamini–Hochberg; Supplementary Table S3). Regarding signal pathway analysis, our data indicated that male patients showed a higher likelihood of genomic alterations in the JAK–STAT (33.3% vs. 16.7%, P = 0.0139).
A previous study had reported an enrichment of sex-biased genes on the X chromosome [24]. In light of this, we sought to investigate whether there were differences in the mutational profiles of X-linked genes in HCC based on gender. A total of 20 X-linked genes were included in our panel, and the detailed analysis results are shown in Supplementary Table S4. Initially, our finding indicated that compared to male patients, more female patients with mutations in BCOR, BTK, and XIAP had P values of 0.0066, 0.0457, and 0.0376, respectively. However, when we applied a statistical adjustment for multiple comparisons to our data, the initial statistically significant difference we observed was no longer evident. Consequently, after applying stringent correction, we did not detect any statistically significant differences in the mutation patterns of these X-linked genes between males and females.
In terms of mutational signatures, we grouped and analyzed samples with a substantial number of mutations (≥ 5 mutations) based on sex and/or smoking status (Supplementary Table S5 and Fig S4). None of the female smokers met the criteria and were excluded from the analysis. Our findings revealed that the most prevalent mutational signature in the Taiwanese cohort was signature 22, which is associated with exposure to aristolochic acid. This was followed by signatures 1 (related to aging), 18 (possibly associated with damage by reactive oxygen species), 24 (associated with exposure to aflatoxin), 27 (of unknown etiology, possible sequencing artifact), and 28 (unknown etiology). As expected, the frequencies of mutation signatures associated with smoking (Signatures 4) and tobacco chewing (Signatures 29) were higher in males when compared to females. However, it is important to note that these differences did not reach statistical significance. Notably, the frequencies of signatures 15 (associated with defective DNA mismatch repair), 23 (unknown etiology), and 26 (related to defective DNA mismatch repair) were higher in smokers than non-smokers. In contrast, signature 27 (unknown etiology) was more prominent in non-smokers.
3.4 Comparison of genomic profiles between genders in the TCGA HCC datasetConsidering the limited sample size of the Taiwanese cohort, we extended our analysis to the TCGA HCC dataset to investigate the presence of sex-biased genomic alteration in subgroups stratified by ethnicity. In the TCGA dataset, we found that CTNNB1, CCNE2, and TP53 were the genes that altered significantly more in males than in females (Fig. 2a and Supplementary Table S6). When we divided the dataset into Asian and non-Asian subgroups, the sex-biased mutation profile was only observed in the non-Asian subgroup. The mutation frequencies of CTNNB1 and TP53 were significantly higher in male patients than in females (35.65% vs. 12.5% and 36.52% vs. 15%, respectively; Fig. 2b), with adjusted P values of 0.0024 and 0.004. No significant gender-based differences in mutation profiles were found in the Asian subgroup.
Fig. 2
Alteration frequencies of driver genes by sex among the TCGA dataset. a All patients; b Asian and Non-Asian subgroups
In summary, our study did not identify sex-biased genomic alterations in the Taiwanese cohort. However, we observed higher mutation frequencies in the CTNNB1 and TP53 genes, and copy number gains in the CCNE2 gene, in male patients in the TCGA dataset.
3.5 Ethnic-specific genomic alterationsMeanwhile, we uncovered an interesting aspect regarding ethnic-specific genomic alterations. Specifically, we found several hotspot mutations in JAK1 (S703I and S729C) and STAT3 (Y640F) that may show an ethnic-specific distribution. In the Taiwanese cohort, 4 and 6 out of 195 (2.0% and 3.1%, respectively) carried JAK1 p.S703I and p.S729C mutations, and 10 out of 195 (5.1%) patients harbored STAT3 p.Y640F. However, when we examined the TCGA dataset, a notable difference emerged. In the Asian subgroup, JAK1 p.S703I and p.S729C were identified in 1 (0.6%) and 2 (1.3%) out of 158 patients, but none were detected in the non-Asian subgroup (Supplementary Fig S5). Similarly, STAT3 p.Y640F was found in 2 (1.2%) out of 158 Asian HCC patients but was absent in non-Asian patients (Supplementary Fig S6). Collectively, the results implied the presence of ethnic group-specific genomic alterations, although further research is needed to confirm these findings.
3.6 Sex-specific prognostic markersTo investigate whether clinicopathological factors influence the prognosis of patients with HCC in the Taiwanese population, we retrieved survival data from the National Health Research Institutes Biobank database. The median overall survival (OS) was 80 months, with a range of 0.7 to 165 months. We compared OS based on various clinical parameters using Kaplan–Meier survival curves and log-rank tests. Supplementary Table S7 shows that our results revealed a significant difference in OS between patients with advanced-stage disease (stage III and IV) and those with early-stage disease (median OS = 35 months vs. 95 months, P = 0.0047; log-rank test). However, no significant impact on OS was found for age (P = 0.1011), viral infection (P = 0.5584), cirrhosis (P = 0.2274), alcohol consumption (P = 0.9018), and smoking (P = 0.7820). Additionally, there were no significant differences in OS between male and female patients (P = 0.7559), which aligns with previous observations [41].
Next, we explored the relationships between genomic alterations and overall survival within the Taiwanese population, specifically with respect to sex. Results are shown in Fig. 3, Supplementary S7, and detailed in Supplementary Table S8. We found that two male patients carrying KMT2C-mutated tumors had shorter OS than those with wild-type KMT2C (median OS: 12 and 80 months, respectively, P = 0.0034; Supplementary Fig. 7a–c). Additionally, a single male patient with a putative APC mutation exhibited an exceptionally short OS of 3 months, starkly contrasting patients with wild-type APC gene (median OS = 75.5 months, P < 0.0001; Supplementary Fig. 7d–f). Notably, in the TCGA Asian subgroup, we identified one male patient with a mutated KMT2C and another with a mutated APC; both had shorter OS compared to those with wild-type KMT2C or APC (Supplementary Fig. 8a–f). However, due to the limited number of patients carrying KMT2C and APC mutations, further research is warranted to draw definite conclusions.
Fig. 3
Kaplan–Meier survival analysis for HCC patients in the Taiwanese cohort. The overall survival (OS) was evaluated for all patients (a, d), male patients (b, e), and female patients (c, f) in the Taiwanese cohort. The analysis was based on the genomic status of alterations in the JAK–STAT and WNT-β-catenin pathways
Furthermore, we found that female patients with copy number gains of the STAT3 gene (n = 4) tended to have a poorer prognosis compared to those with the wild-type (WT) STAT3 gene (Supplementary Figure S7g–i and Table S8). The median OS of female patients with WT and STAT3 gains were 92.5 months and 16 months, respectively. A similar trend was seen in the TCGA Asian subgroup, where female patients with STAT3 gene copy gains (n = 7) had significantly shorter OS than females with WT STAT3 gene (Supplementary Figure S8g–i). It is noteworthy that STAT3 gain remained as an independent predictor of shorter OS after adjusting with the patient’s stage and age characteristics (Hazard ratio = 10.434, 95% CI 3.331–32.677, P < 0.001; Cox proportional hazard model; Table 2). This difference was not evident in the male subgroup or the non-Asian dataset. However, the limited number of STAT3 alteration detected in the two studied cohorts suggests that these findings should be interpreted cautiously. Similar to the findings of KMT2C and APC mutations in male HCC patients, further validation in larger cohorts is essential to confirm their clinical significance.
Table 2 The results of Cox regression analysisFrom the pathway-based point of view, we observed female patients with altered JAK–STAT or Wnt-β-catenin pathways displayed a shorter overall survival than those with non-altered signal pathways, as shown in Fig. 3a–f. The median OS of female HCC patients with a non-altered JAK–STAT signaling pathway (n = 55) was 95 months, whereas patients with an altered JAK–STAT signaling pathway (n = 11) had a median OS of 23 months (P = 0.0178; log-rank test). After adjusting for patients’ stage and age, the alteration of the JAK–STAT pathway remained an independent factor associated with shorter OS (Hazard ratio = 2.547, 95% CI 1.195–5.432, P = 0.016; Cox proportional hazard model; Table 2). Furthermore, although not reaching statistical significance, a similar trend was observed in the TCGA Asian subgroup (n = 15, P = 0.1658; Fig. 4a–c). Female patients with an altered Wnt-β-catenin pathway also displayed poor OS (median OS = 52 months) compared to those with an unaltered Wnt-β-catenin pathway (P = 0.0201; log-rank test; Fig. 3d–f). However, in the TCGA Asian subgroup, a poor prognosis was observed in patients with altered Wnt-β-catenin pathway, irrespective of gender (Fig. 4d–f), yet, the results did not reach statistical significance after adjusting for patient age and stage characteristics (Table 2).
Fig. 4
Kaplan–Meier survival analysis for HCC patients in the TCGA Asian subgroup. The overall survival (OS) was evaluated for all patients (a, d), male patients (b, e), and female patients (c, f). The analysis is based on the genomic status of alterations in the JAK–STAT and WNT-β-catenin pathways
留言 (0)