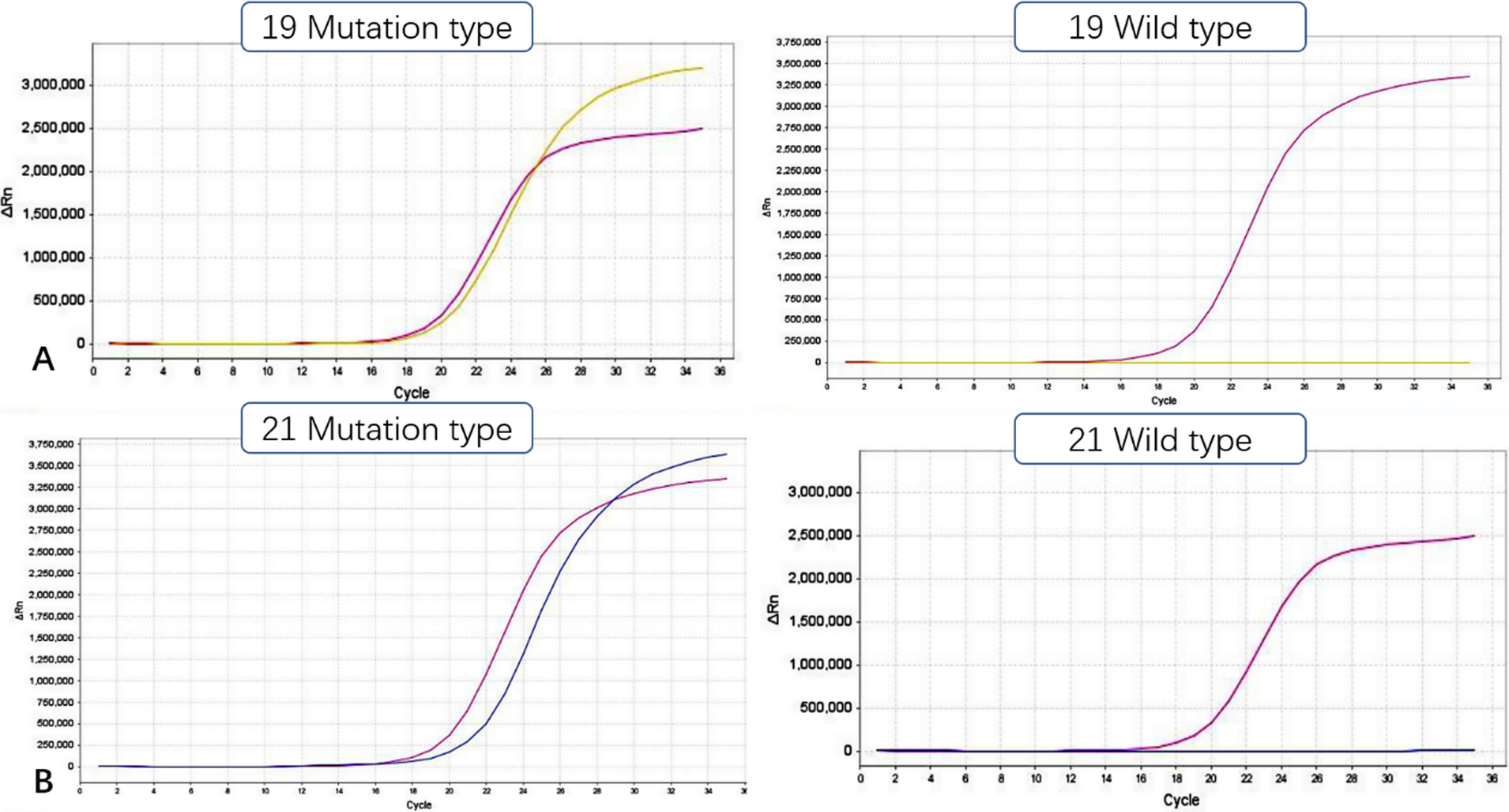
EGFR serves as a transmembrane receptor primarily situated on the cell surface and is frequently overexpressed in patients with non-small cell lung cancer (NSCLC), thereby facilitating tumor cell proliferation and metastasis [15, 16]. Importantly, EGFR mutations predominantly occur in exons 19 and 21 (L858R, L861Q), significantly impacting tumor sensitivity to EGFR-TKI therapy [17,18,19,20,21,22]. Patients with elevated EGFR expression levels typically demonstrate increased responsiveness to targeted drugs [23]. Geographically, EGFR mutation rates vary, with approximately 10% in Western countries and up to 50% in Asian populations. In China, the overall mutation rate among NSCLC patients is approximately 30% [24, 25]. Furthermore, mutation rates are notably higher among non-smokers, females, and patients with glandular carcinoma [17]. Specifically, mutation rates are approximately 50% in lung adenocarcinoma, 60–70% in non-smoking lung cancer, and around 10% in squamous cell carcinoma (SCC) patients [24, 25]. In our study involving 176 NSCLC patients, exon 19 exhibited an EGFR mutation rate of 23.86%, while exon 21 had a mutation rate of 12.50%. Subgroup analyses revealed varying mutation rates based on age (< 60 years: 53.85% vs. ≥ 60 years: 29.03%), gender (male: 23.81% vs. female: 47.83%), presence of pleural invasion (no invasion: 40.54% vs. invasion: 6.9%), and vessel invasion (no invasion: 39.73% vs. invasion: 20%). Thus, EGFR mutation rates are influenced by factors such as sex, age, pleural invasion, and vessel invasion. Although a correlation between tumor location and EGFR mutation was observed, further investigation is warranted due to the limited number of tumor specimens from the right lobe of the lung.
The relation between tumor biomarkers and EGFR mutation has been elucidated in previous studies. The expression level of various pathological types of tumor biomarkers exhibit significant difference before and after the treatment, enabling dynamic measurement of tumor recurrence and metastasis [26]. EGFR mutations can lead to abnormal activation of EGFR, resulting in abnormal activation of Akt and STAT3/5 downstream of the EGFR signaling pathway, thereby significantly inhibiting apoptosis induction [27, 28]. Abnormal activation of EGFR signaling can also lead to abnormal activation of different pathways, resulting in the synthesis and activation of relevant transcription factors, thereby enhancing cell proliferation. CEA functions as an adhesion protein whose expression is regulated by the activation and modulation of EGFR signaling, potentially explaining the upregulation of CEA following EGFR mutation [29]. Research has shown a higher EGFR mutation rate in patients with elevated serum CEA levels [30]. Additionally, as demonstrated in this study, the percentage of EGFR mutation was positively correlated with serum CEA levels (> 6.5 ng/mL, P = 0.004), consistent with previous findings [31].
This study represents the first investigation into the association between TAP and EGFR mutation in NSCLC. When stratifying by gender, male patients exhibited EGFR mutation rates of 13.3% (8/60) and 50% (12/24) when TAP ≤ 228 µm2 and > 228 µm2 (P = 0.001), respectively. For females, EGFR mutation rates were 10.0% (5/50) and 92.9% (39/42) (P = 0.000) under the same TAP conditions. Notably, TAP levels are elevated in cancer patients, particularly in those at advanced stages and grades, but prior studies did not specifically investigate its association with EGFR mutation in advanced NSCLC. Our findings reveal a positive correlation between increased TAP and EGFR mutation, although the underlying mechanism remains unclear.
Through univariate and multivariate analyses, we assessed the predictive significance of CEA and TAP for EGFR mutation. Elevated CEA or TAP levels were associated with a higher likelihood of EGFR mutation. This corroborates previous research, such as Shoji et al., who reported that higher CEA levels independently predict EGFR mutation (OR: 4.70, P = 0.036). Additionally, our study explored the diagnostic utility of elevated CEA (> 6.5 ng/mL) in predicting EGFR mutation, yielding an AUC of 0.668 (95% CI 0.585–0.750, P = 0.000), with sensitivity and specificity of 31.3% and 80.0%, respectively, consistent with prior findings. Concerning TAP, the AUC was 0.833, with sensitivity and specificity of 79.7% and 87.0%, respectively, in females, surpassing those in males (AUC: 0.897; sensitivity: 88.6%; specificity: 93.8%).
In this study, we aimed to explore the association between TAP level and EGFR mutation in NSCLC. It was found that NSCLC patients with higher TAP levels exhibited a higher EGFR mutation rate. Moreover, TAP could effectively distinguish patients with EGFR mutation. For female patients in advanced NSCLC stages, TAP could potentially facilitate the diagnosis of mutation status in cases where tissue biopsy is not feasible. These findings require validation through studies with larger sample sizes, particularly focusing on tumors in the middle lobe of the lung. Additionally, further research is needed to elucidate the mechanisms underlying the impact of TAP and CEA levels on EGFR mutation.
We propose a positive association between TAP expression levels and EGFR mutation status in NSCLC patients. Within a defined range, an escalation in TAP expression correlates with an increased rate of EGFR mutation positivity. In instances where sample size for EGFR mutation testing is limited or samples are unavailable, assessing TAP levels can offer a straightforward and convenient screening approach. Consequently, NSCLC patients exhibiting elevated TAP levels may benefit from EGFR-TKI therapy, presenting a more pronounced clinical response and enhanced quality of life.

留言 (0)