
記住我




This cross-sectional study was carried out at the Reproductive Medical Center of the First Affiliated Hospital of Kunming Medical University from March 2016 to April 2023. Patients who received ART treatments during the study period were potentially eligible. The antral follicle count (AFC) was determined by transvaginal ultrasonography examinations on days 2–4 of an unstimulated menstrual cycle. Blood samples also collected on days 2–4 of the menstrual cycle for analysis on the same day were used to measure the serum levels of AMH concentration and markers of thyroid function. The demographic and clinical data of the patients who underwent intrauterine insemination, in vitro fertilization and embryo transfer (IVF-ET), or intracytoplasmic sperm injection (ICSI) were recorded in a database.
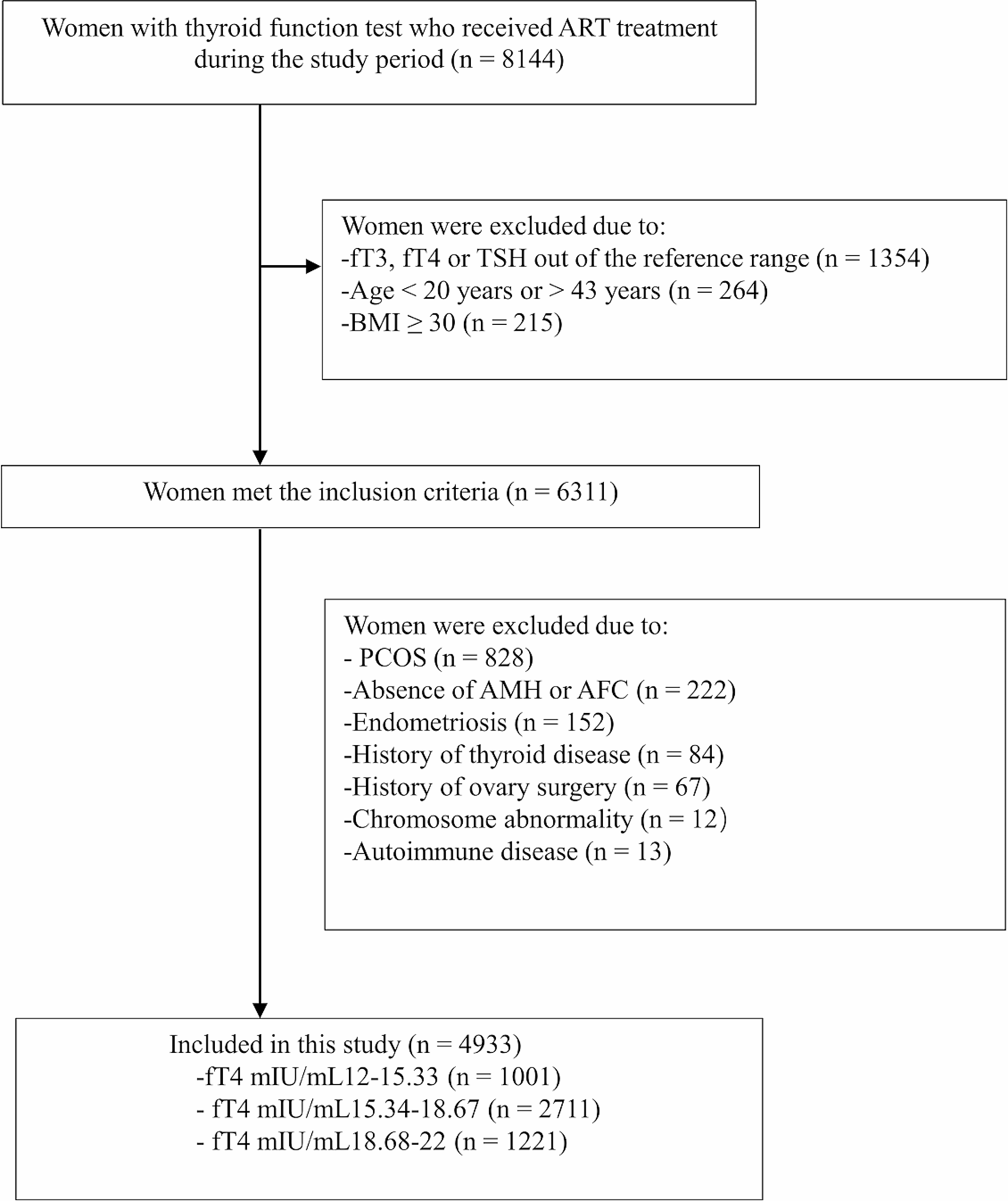
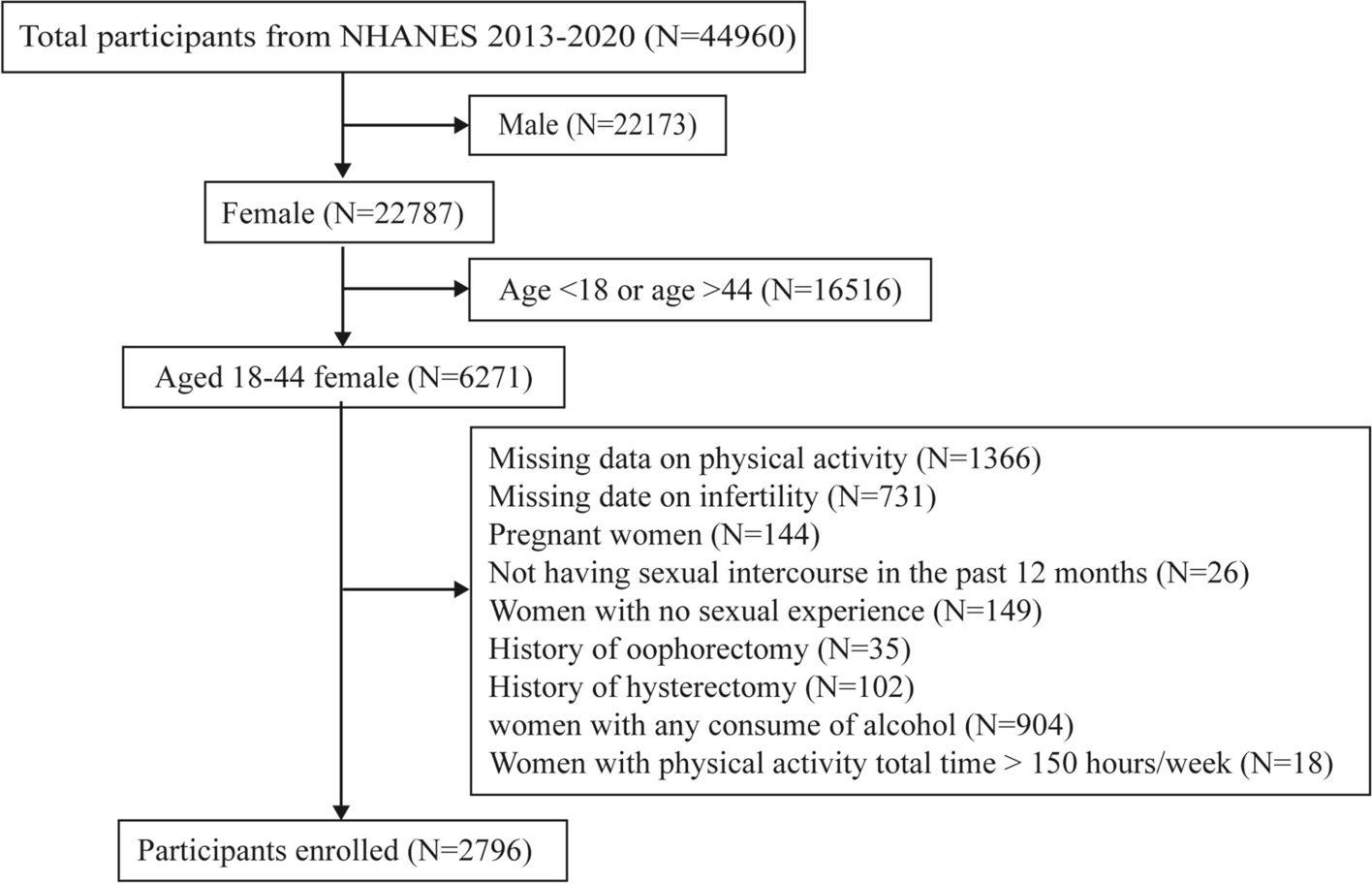
The inclusion criteria for participants were as follows: (1) female patients aged 20–43 years; (2) a body mass index (BMI) less than 30 kg/m2; (3) treatment with IVF/ICSI; and (4) normal concentrations of free triiodothyronine (fT3), fT4, and serum thyrotropin (TSH). The exclusion criteria were women who were diagnosed with (1) polycystic ovarian syndrome, (2) endometriosis, (3) overt thyroid dysfunction or those who had (4) a history of thyroid disease (treated or not), (5) a history of ovarian surgery or ovarian tumor, (6) chromosomal abnormality. Finally, the data of 4933 women were included in the data analysis (Fig. 1).
Fig. 1
Flowchart of the participant selection in this study
TAI: thyroid autoimmunity; ART: assisted reproductive technology; PCOS: polycystic ovarian syndrome; AMH: anti-Müllerian hormone; AFC: antral follicle count
The patients were divided into three groups based on normal fT4 concentration tertiles in women: the low-normal tertile (12.00–15.33 pmol/L), middle-normal tertile (15.34–18.67 pmol/L), and high-normal tertile (18.68–22.00 pmol/L) [13]. The differences in AMH concentration and the risk of DOR, defined as an AMH concentration < 1.1 ng/mL [14,15,16], between the fT4 concentration tertile groups were analyzed. The AFC was compared between the three fT4 concentration groups.Last, the number of aspirated oocytes, which reflects the ovarian reserve and the response to ovarian stimulation, was also compared between the three fT4 concentration groups.
The primary outcomes of this study were the AMH concentration and the risk of DOR. The secondary outcomes were the AFC and the number of aspirated oocytes.
Measurement of the AMH concentrationSerum AMH concentrations were measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Kangrun Biotech, Guangzhou, China) and a plate reader (EXL808; BioTek Instruments, Shanghai, China). The linear range of the kit is 0.07–18 ng/ml, r ≥ 0.9900, the minimum detection limit ≤ 0.06 ng/mL. and the intra- and inter-assay coefficients of variation (CVs) were ≤ 15% and ≤ 8%, respectively.
Measurement of thyroid functionWe measured serum fT3, fT4, TSH, thyroperoxidase antibody (TPO-Ab), and thyroglobulin antibody (Tg-Ab) concentrations using ELISAs and a Cobas E601 analyzer (Roche), as described previously [17]. We used the manufacturer-recommended reference ranges as follows: 0.27–4.20 µIU/mL for TSH, 3.1–6.8 pmol/L for fT3, 12–22 pmol/L for fT4, < 115.0 IU/mL for Tg-Ab, and < 34 IU/mL for TPO-Ab. The ranges of intra-assay CVs were 1.1–3.0% for TSH, 1.3–6.5% for fT3, 1.6–5.0% for fT4, 1.8–2.1% for Tg-Ab, and 2.8–4.8% for TPO-Ab. The ranges of inter-assay CVs were 3.2–7.2% for TSH, 1.6–7.2% for fT3, 1.9–6.3% for fT4, 4.6–5.1% for Tg-Ab, and 3.5–6.1% for TPO-Ab. TPO-Ab concentrations ≥ 34 IU/mL and Tg-Ab concentrations ≥ 115 IU/mL were considered positive. Thyroid autoimmunity (TAI) was diagnosed when the patient tested positive for TPO-Ab or Tg-Ab.
Measurement of the AFCWe evaluated the ovarian AFCs on days 2–4 of an unstimulated menstrual cycle. First, transvaginal ultrasound was performed jointly by two well-trained reproductive endocrinologists to estimate the number of follicles. The AFC for each patient was then calculated as the sum of antral follicles (2–9 mm in diameter) in both ovaries in the early follicular phase.
Ovarian stimulation and oocyte aspirationThe number of aspirated oocytes is one of the indexes uesd to evaluate ovarian reserve function, and the number of aspirated oocytes obtained varies with different ovarian stimulation protocols. Therefore, it is necessary to adjust the effects of different ovarian stimulation protocols when assessing oavrian reserve function. The patients were treated with different ovarian stimulation protocols, including long-term gonadotropin-releasing hormone (GnRH) agonist (long protocol, n = 2189), GnRH antagonist (antagonist protocol, n = 1828), the mild stimulation protocol (n = 491), and other protocols (n = 366) according to their conditions. The details of the therapeutic regimens of different stimulation protocols are described in previous studies [18, 19]. Recombinant human chorionic gonadotropin (HCG; 250 mg, Ovidrel; Serono) was administered when two leading follicles reached an average diameter of 18 mm. Oocytes were then retrieved transvaginally 34–36 h after HCG administration by using a single lumen needle attached to a syringe to aspirate the follicles under transvaginal ultrasound guidance. Finally, the oocytes were placed in a culture dish and confirmed under a stereomicroscope.
Statistical analysisThe demographic and clinical data of the patients in the three fT4 concentration groups were compared using a one-way analysis of variance for normally distributed continuous variables, the Kruskal–Wallis H test for non-normally distributed continuous variables, and Pearson’s chi-square test for categorical variables. Multivariable generalized linear models with linear (AMH concentration as the dependent variable), logit (the risk of DOR as the dependent variable), and Poisson (the AFC and the number of aspirated oocytes as the dependent variables) links were used to analyze the associations between fT4 concentrations and ovarian reserve markers. The models were adjusted for women’s age, BMI, TSH concentration, infertility type, infertility diagnosis, infertility duration, and TAI positivity when analyzing the AMH concentration, risk of DOR, and AFC. To reduce skewness, AMH concentrations were subjected to log10 transformation before performing regression analyses, as described previously [20, 21]. The models were further adjusted for the ovulation stimulation protocol, gonadotropin dose, and gonadotropin duration when analyzing the number of aspirated oocytes.
To investigate the potential effect of the patient’s age on the associations between the fT4 concentration tertiles and ovarian reserve, we performed a regression analysis stratified by age (< 35 or ≥ 35 years) using a generalized linear model. The associations of fT4 concentrations with the AMH concentration, risk of DOR, AFC, and number of aspirated oocytes were also analyzed using a general additive model (GAM) and smooth curve fitting. Confounding factors were adjusted in all of the abovementioned analyses. All of the statistical tests were two-sided, and a p value < 0.05 was considered statistically significant. SPSS 26.0 (SPSS, IBM Inc., Chicago, IL USA), EmpowerStats 4.1 (X&Y Solutions Inc., Boston, MA, USA), and R 4.3.1 (packages mgcv and ggplot2, the R Foundation) were used for data analysis.
留言 (0)