Low prognosis patients of POSEIDON groups 3 and 4 had significantly lower LBR and CLBR in multiple embryo transfer cycles [5]. However, almost all published studies being focused on CLBR of low prognosis women included both fresh and frozen embryo transfer cycles. Here, we performed the cohort study to tell the discrepancy of CLBR up to 6 cycles of frozen embryo transfer in women of POSEIDON groups 3 and 4, which is of great significance to clinical counseling before IVF as the increased utility of freeze-all strategy in modern ART practice. In our study, although the LBR of POSEIDON group 3 was lower in the first four ET cycles, while its CLBR could more or less “catch up” with the control group 1 after six ET cycles, which means that patients < 35 years with low AMH can benefit from the multiple ET cycles. However, for patients ≥ 35 years old, the disparity of the CLBR between POSEIDON group 4 and control 2 group increased with the number of FET cycles, and the last two cycles made little contribution to the CLBR for POSEIDON group 4.
Interpretation of findings
Generally, the age-related reduction of LBR is mainly caused by the decreased oocyte quality. Higher embryo aneuploidy rates in women over 35 years old resulted in a corresponding decrease in implantation rate and the increase in miscarriage rate [8]. However, for those women undergoing implantation failure in consecutive four FET cycles, age did not make means in LBR in the following 2 ET cycles, which suggested that uterine factors, including uterine local immune environment, may contribute more for repeated implantation failure (RIF) in younger women. The study of Chen et al. [9] can support the perspective as they found premature aging of the endometrium exists in young women (<35 years old) with recurrent implantation failure. Another evidence came from the data that Preimplantation Genetic Testing for Aneuploidy (PGT-A) was proved to be effect in improving LBR in advanced age patients with RIF, but not in young RIF women [10].
In fresh IVF cycle, serum AMH was a predictor for LBR, which was mainly contributed by greater oocyte yield [11]. However, the role of serum AMH on LBR in frozen embryo transfer cycle was rarely studied. According to Li et al. [12], the LBR in the first FET cycle after oocyte retrieval was positively associated with AMH. and the reason may be higher chances of good quality embryo being selectable for transfer in the first cycle. Here, the comparison of LBR between POSEIDON group 3 or group 4 and control groups also suggested that LBR was higher in the first FET cycle for those with higher AMH, but not in all FET cycles.
Based on previous study, AMH and age were both independent predictors for CLBR [13]. Aimed to exclude the interference of fresh cycles, we only enrolled FET cycles following “freeze all” cycles in the study and observed the effects of AMH and age on CLBR. From the first to the sixth FET cycle, the CLBR of POSEIDON group 3 kept rising and the disparity of CLBR between POSEIDON group 3 and control 1 group was stepdown. Finally, the CLBR of two group of women was very closed. However, the CLBR disparity between POSEIDON groups 4 and control 2 group was increased over the course of six FET treatments. The CLBR of POSEIDON group 4 was finally much lower than control 2 group and reached plateau after 5 FET cycles Thus, the negative effect of AMH on CLBR is compensated by repeated cycles in young women but augmented in advanced age of women. It should be noticed that the CLBR of control 2 group reached 88% up to six FET cycles which suggested higher AMH could compensated the adverse impact of age to a certain extent in women older than 35 years. The mechanisms may be more oocytes retrieved resulted in more chances to select euploid embryos with good morphology to transfer.
The COX regression analysis confirmed that in FET cycles, POSEIDON criteria was an independent factor positively associated with CLBR. Until now, only one large cohort study on CLBR in FET cycles was published which analyzed the CLBR within 5 years or 9 FET cycles in groups based on POSEIDON criteria [14]. The CLBR over 5 years estimated by optimistic analytical method was 0.75 (0.71–0.78) in POSEIDON group 3, almost the same as that of control group with 0.79 (0.78–0.80) and much higher than 0.41 (0.37–0.46) in POSEIDON group 4. Interestingly, although they included up to 9 cycles, all patients reached a CLBR plateau after 3.5 years or 6 FET cycles. According to the published data and our results, although women of both POSEIDON group 3 and group 4 have diminished ovarian reserve, the noticeable differences in CLBR after 6 cycles of FET between the two groups indicated female age has more significant impact on the CLBR than the ovary reserve parameter. These results were in line with Hu’s study [13]. which reported that the age did not negative affect CLBR in those ≤ 35 years, while in 36–38 years, 39–40 years and 41–42 years old group, the adjusted HR of age on cumulative live birth is 0.71 (0.58–0.88), 0.45 (0.35–0.60) and 0.27 (0.19–0.38) for respectively. The higher embryos aneuploid rate was still the greatest factor affecting pregnant outcome in advanced age of women. Luo’s [15] report confirmed that in POSEIDON 4 group undergoing PGT-A, 61.7% women failed to obtain euploid embryos, while in group of POSEIDON 3 the rate was only 18%.
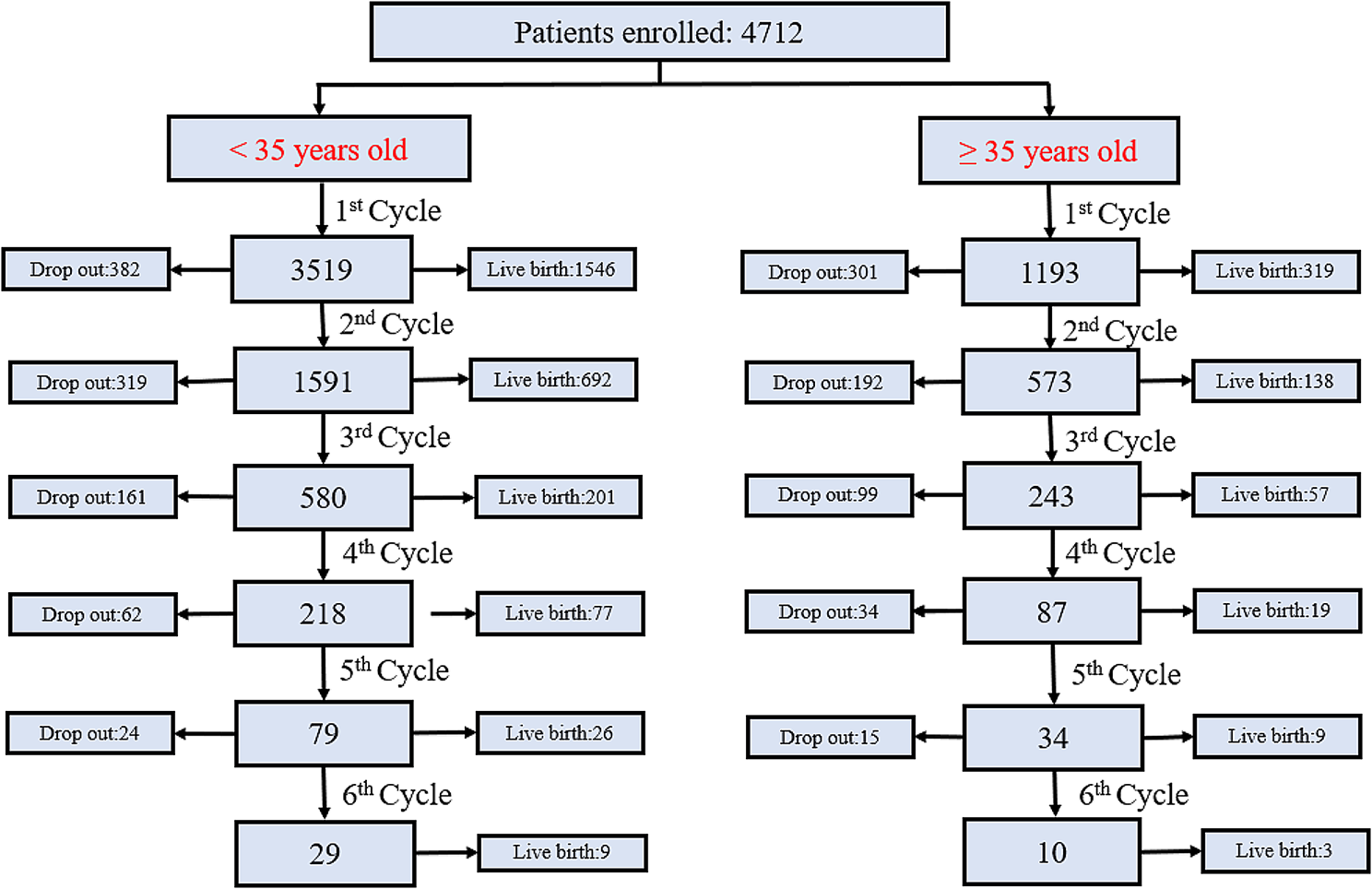
This study has some limitations. The first was the percentage of the patients who dropped out, which was also a common problem while researching cumulative outcomes. The reason for discontinuation of treatment may be physical and emotional strain, financial burden, or the lack of informative censoring from doctors. To account for this, we calculated ‘optimal’ estimates, which assumes that the cumulative live-birth rate in women who discontinue IVF had the equal chances of getting live birth to those who continue further treatments. Second, this was a single-center retrospective study and the retrospective nature of the study cannot exclude all biases resulted by uneven patients’ basic data, such as obesity, endometriosis, adenomyosis and so on. Future prospective studies in different. populations may be necessary to validate the results.
Clinical implications
The reporting of the CLBR over multiple frozen embryo transfer cycles of low prognosis patients has important clinical implications. First, we were delighted to find out that young women with low ovary reserve could benefit from extending the number of ET cycles. So, for POSEIDON group 3 patients, more efforts should be focused on increasing the number of oocytes retrieved through tailored controlled-ovarian-stimulation (COS). Therefore, novel COS strategies, such as oocyte/embryo accumulation in consecutive cycles [16] or double ovarian stimulation in the same ovarian cycle [17], have been proposed. Also, as the oocyte quantitative parameters had limited predicting value in CLBR for women younger than 35 years, those women with lower AMH may not be considered as traditional “low prognosis” in clinical practice, or they should be informed more about optimistic outcomes after consecutive ET cycles than a single cycle.
Second, for POSEIDON group 4, as the increased rate of aneuploid embryos resulted higher risk of implantation failure and miscarriages, more oocyte yield may be not enough to compensate the decrease in oocyte quality. Thus, moreover, consultation should be conducted to inform the reduction of the probability of live birth and preimplantation genetic testing for aneuploidies (PGT-A) should be recommended after 3–4 cycles of implantation failure.





留言 (0)