
記住我



We developed our software prototype for research from scratch using several programming languages and concepts. The developing process involved medical experts and engineers from our local Department of Surgery. Demands, regarding a possible future model-based surgical documentation platform, were thus directly derived from our local experience in complex visceral surgery and surgical documentation. The entire developing process from planning to a functional proof-of-concept prototype took 12 months. The core system for storing and administering the simulated patient models was developed in an 'apache' version 2.4.52 web server environment running on a virtual machine with Ubuntu GNU/Linux server edition 22.04. A configuration with 4 Gigabyte RAM and 1 CPU Core (AMD® Ryzen 7 3700u with a clock rate of 3.2 GHz) was enough to run the application stable and reliably. 'PHP' version 8.2.13 and a 'MYSQL' database system version 8.0.35 were deployed as the application's backbone on the server side. 3D rendering of the pre- and postoperative anatomical patient states was performed using a self-written R script (R version 4.1.2) with the additional packages 'rgl' version 1.2.1 (a visualization framework using OpenGL) and 'htmlwidgets' version 8.0.35. [11,12,13] The 3D models are calculated and displayed immediately after inserting modifications via the SDM-M web interface. The exclusive use of the Hypertext Markup Language (HTML) and JavaScript on the client side achieved compatibility with all modern web browsers, allowing for using the application on any computer or handheld device. The software prototype for research comprises three core functionalities:
The first is a database system to store and edit basic anatomies (BA) upon which individual patient models can be built. Anatomical structures are integrated into a hierarchical tree topology of organ systems. For our proof of concept, we included seven functional organ classes relevant to surgery on the digestive tract: 'Arterial,' 'Venous,' 'Portal,' 'Liver,' 'Biliary,' 'Pancreatic,' and 'Intestine.' The hierarchical concept represents proven anatomical relations known from medical standard books. To simulate the anatomical structures' functional (physiological) properties, they are connected via 'natural links' similarly to 'hyperlinks' in the World Wide Web. A link leads from one structure to another in the direction of their functional conjunction. For instance, a link from an artery A to another artery B represents the physiological blood flow in that direction. Accordingly, a natural link from the ileum to the ascending colon represents the physiological direction of stool propulsion. (Fig. 1B) This concept allows for functional reasoning and the creation of even comprehensive physiological models. The anatomical hierarchy and the natural links can easily be maintained by editing parent or child structures and entering spatial information like diameters and lengths.
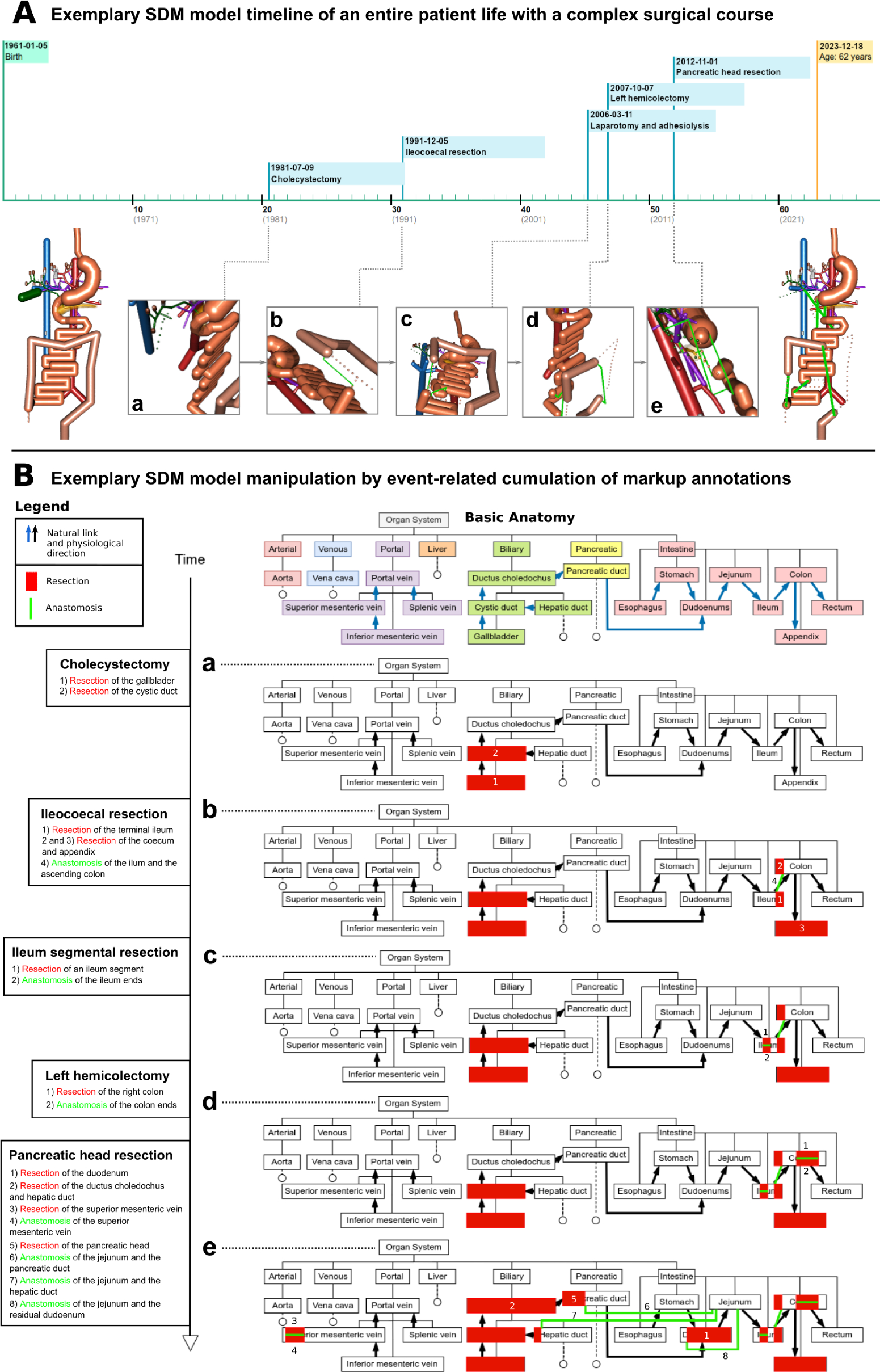
Fig. 1
A Exemplary SDM model timeline of a patient with complex surgical course, a–e Interactive 3D models of the distinct postoperative anatomy after every single surgery, the patient underwent during their life. The full surgical report and the 3D models can be opened by clicking on the respective flag along the timeline. B Exemplary SDM model manipulation of a basic anatomy (BA) – Each surgery a-e increases the cumulative surgical load of the patient. When sharing the model with other medical professionals or facilities, only the colored information in the charts must be transferred. The example shows the lifetime of the simulated patient ‘P2’ from the evaluation study
The second core function is a 3D rendering system deploying OpenGL, which creates the output directly from the database using the BA and natural links. [12] An anatomic structure thereby ’originates’ from another it is connected to by a ’natural link. Dotted lines for resections and bold green lines for reconstructions illustrate patient-individual modifications of the BA during surgical procedures.
The 3D output is seamlessly integrated into the third core functionality, which is a comprehensive solution for writing and displaying surgical notes with attached 3D annotations for a deliberate number of patients. Reports can be authored using text input for each surgical step and a special input form to annotate resections of organ parts or insert 'artificial links' in terms of reconstruction. The modifications are immediately integrated into the patient-individual anatomical model and displayed in the graphical user interface (GUI). Each simulated patient has their own 'surgical timeline' with all surgeries available in the database being pointed out as timestamp flags in the correct order. The timeline is divided into decades, allowing for a straightforward reading of a patient's age at a particular surgery. On the left side, the user sees the anatomical state of the simulated patient at birth (without any alterations of the BA), while on the right side, the current state with all resections and reconstructions in terms of the cumulated surgical load is displayed. All 3D models can be moved and turned around interactively in a 3D environment using the PC’s mouse, a track pad, or the touch display of a handheld device. The user can easily zoom into the model to investigate even small structures and alterations. (Fig. 1A) Figure 1 shows the surgical life span of one simulated patient (P2), employed in the evaluation study which is presented below. By clicking on a surgery flag along the timeline, the user can open the particular surgical report with interactive 3D models of the anatomical state before and after this surgery. The panels A/a to e in Fig. 1 show the state after each simulated surgery, accessible by clicking on the respective flag. Figure 1B shows the modeling approach behind the scenes. Based on the standard BA, each surgery causes patient-individual modifications that cumulate with each further surgery in terms of the already mentioned surgical load. Only the colorful highlighted markup information in the panels B/a to e have to be transferred to allow for model reconstruction after transfer to another medical facility. Besides surgical information about resection and reconstruction, even natural anatomical biometrics, such as the length of bowel sections, or arterial supply of organs can be annotated and used to modify the BA individually.
Design of the evaluation studyTwo primary aspects must be considered to estimate a future possible impact of a life-spanning SDM-M for surgical documentation on daily clinical workflow. On the one hand, the data has to be inserted into the model, which is, at the moment, achieved by manual annotation under every single surgical step of a classic surgical report typed or pasted into an online interface. This approach requires little effort, but should be investigated more deeply in future research, especially regarding the aspect of automated data integration.
More important in the current state is the possible improvement in information transfer of a patient's surgical course to a medical professional who did not participate in the underlying surgeries. Thus, our research question was how our approach represented by the proposed software-prototype could improve the perception and understanding of the life-spanning surgical load of individual patients. Therefore, we designed an evaluation study at our local Department of Surgery at the University Hospital Klinikum rechts der Isar in Munich.
We simulated two patient cases (P1 and P2) with similar complex but diverse surgical life-spanning courses. Both patients underwent five devised visceral surgeries with distinct modifications of the BA. (Fig. 2A) P1 underwent appendectomy, twice relaparotomy with adhesiolysis but without bowel resection, left hemicolectomy, and finally, an esophageal resection with gastric sleeve and gastroesophagostomy. P2 underwent cholecystectomy, ileocecal resection, relaparotomy with ileum segment resection, a left hemicolectomy for colon carcinoma, and a pancreatic head resection for cancer with partial resection of the superior mesenteric vein. The simulated surgeries were worked out once in a classic way using narrative surgical notes and once using our prototype software with anatomical annotations. The classic narrative surgical notes for P1 comprised 2700 words, and for P2, 2600 words. Participants for the evaluation study were surgeons and medical students in their last year before graduation from the local Department of Surgery. All participants are involved and experienced in the daily treatment of complex surgical cases. The participants were asked to elaborate and understand the two simulated cases and answer predefined questions in a personal interview with limited time. From an analysis of 2135 physician–patient contacts in our local outpatient department, we derived an average conceded time of 7 min to understand a case roughly at the first contact between patient and physician. Hence, the participants had a maximum of 7 min (420 s) to work out each case but could stop the process at any earlier time as it was comfortable for them. The cases and the approaches (classical paper-based vs. SDM-M) were switched among the subjects to reduce habituation and other confounding factors. Each participant worked out both cases (P1 and P2), one in the classic way and one digitally. (Fig. 2B) The predefined questions of the interview were always the same, but sorted in a different order for the first and second turn of the study. (Fig. 2C) After working out both cases within a maximum of 7 min and answering the standardized questions within 1 min, the participants filled out a questionnaire based on the Raw NASA-TLX (NASA Task-load Index) and the SUS (System Usability Scale). [14,15,16] Moreover, the participants commented on their daily use of modern technical devices like smartphones, tablets, PCs/laptops, and video conferencing software in their private and professional contexts. All participants signed informed consent before their inclusion in the proof-of-concept study. We deployed the statistical software R version 4.1.2 to evaluate the results. [11] Testing for statistical significance was performed using the paired Wilcoxon rank sum test, presuming a level of significance of 5%. The results are given as mean with standard deviation (± SD) or median with interquartile ranges (IQR). For the assessment of the internal consistency of the Raw NASA-TLX, Cronbach's alpha was calculated using the R package 'psych' version 2.3.9. [17, 18]
Fig. 2
Design of the evaluation study – A Surgical course of the two simulated patients P1 and P2. The surgeries are listed in the timely order of their occurrence. B Study course and case allocation. Every participant (surgeon or advanced medical student) worked out both cases. The order of the approaches was thereby switched to exclude confounding by habituation. C For both turns, the same questions were posed, however, in a different order
留言 (0)