
記住我
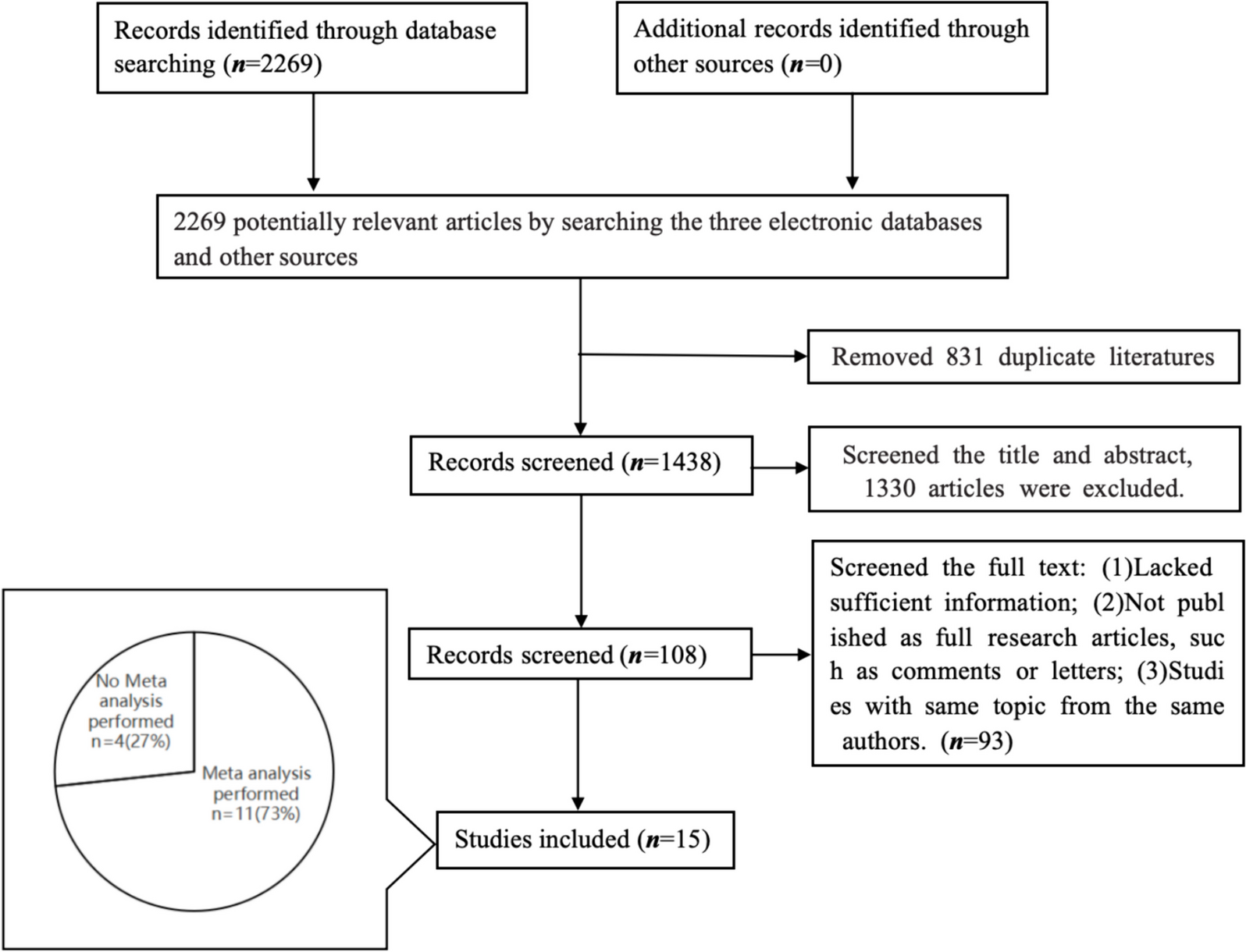
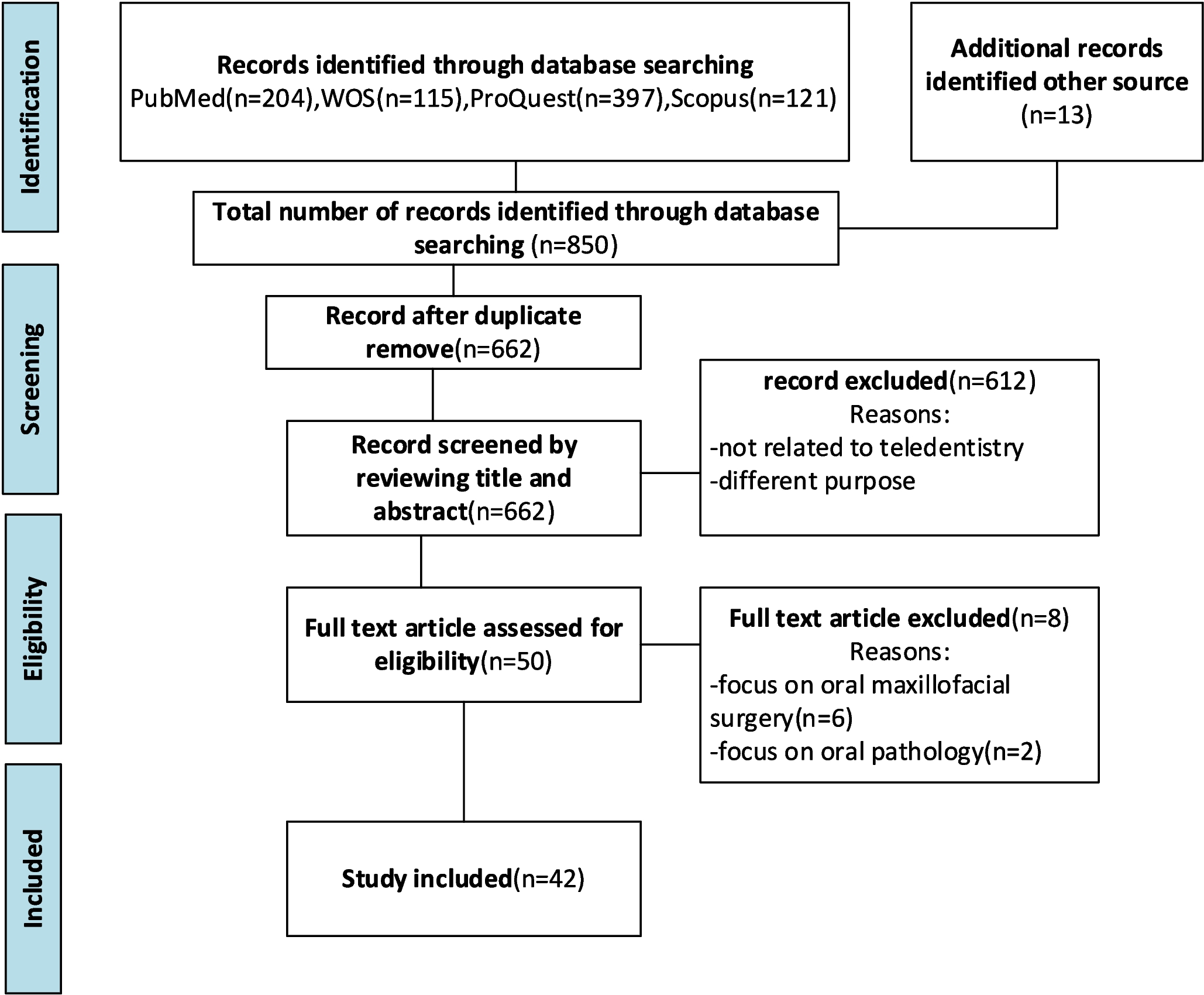
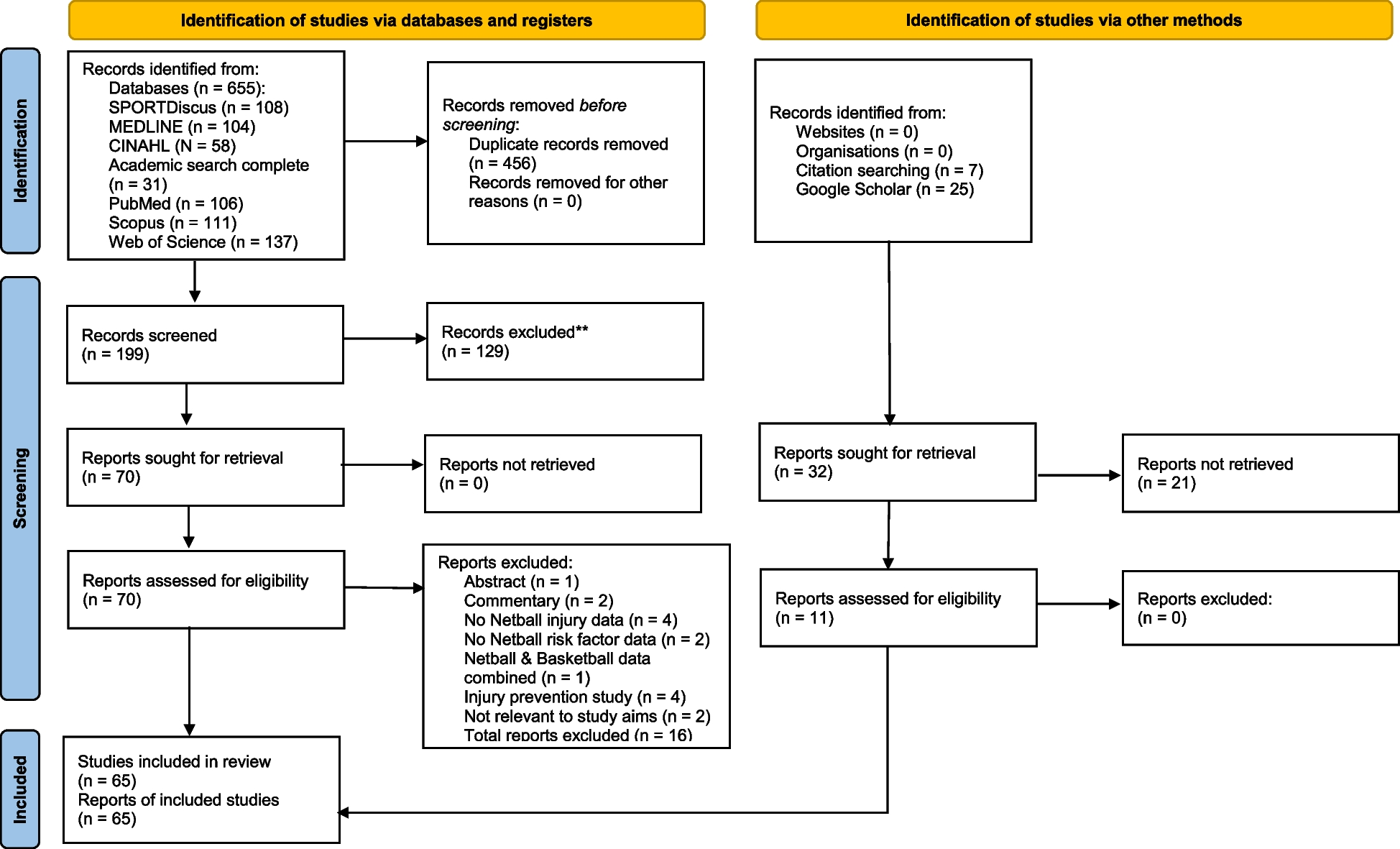
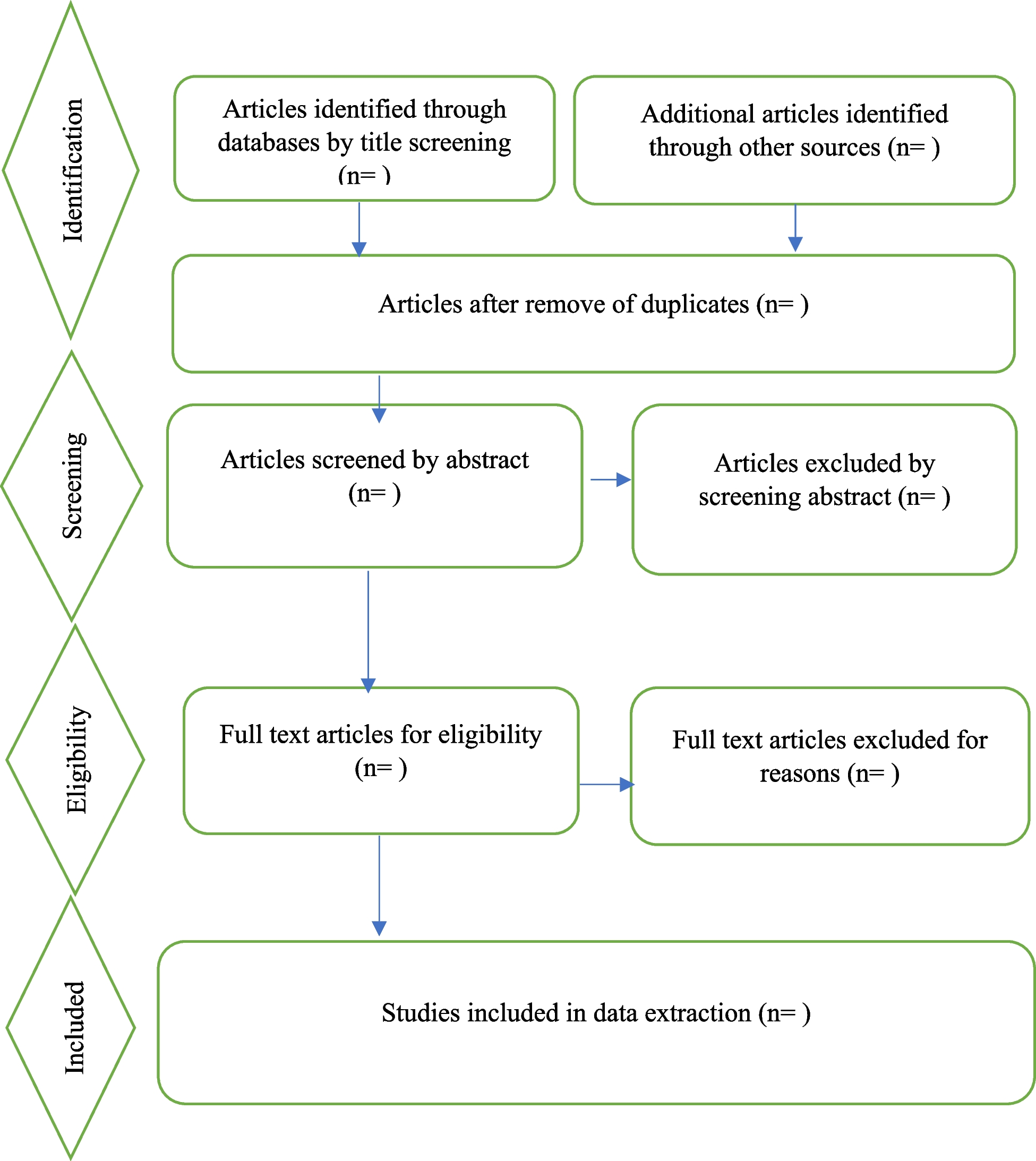

Figure 1 shows the study selection process and results based on the PRISMA 2020 flow diagram for new systematic reviews [39]. In total, 779 articles were identified. A total of 88 of these articles were removed because they were duplicates. After the titles and abstracts were screened, 77 articles were included in the next stage. Of these, 49 articles were excluded due to different reasons. As a result, 28 studies satisfied the eligibility criteria and were included in the review. Of them, 11 were RCTs, and 17 were NRCTs and NRNCTs.
Fig. 1
PRISMA flow diagram. *Records excluded by title and abstract. All the records were excluded by a human. From: Page et al. [39]. For more information, visit: http://www.prisma-statement.org/
Risk of biasMethodological evaluation was conducted in all the articles. Studies were not excluded based on low methodological quality. Tables 1 and 2 present the results of the critical appraisal.
Table 1 Assessment of methodological quality of the RCTsTable 2 Assessment of methodological quality of the NRCTs and NRNCTsThree of the 11 RCTs (27.3%) show a low risk of bias in all domains evaluated. This means that, in general, the studies present an adequate explanation regarding the entire research process (recruitment, group allocation, MBI, data extraction, statistical analysis, etc.). The greatest source of bias is the blinding of participants and researchers, where six articles (54.5%) present unclear risk and two (18.2%) high risk. Regarding random sequence generation, two papers (18.2%) present unclear risk and two (18.2%) high risk. And as for allocation concealment, two articles (18.2%) present unclear risk and only one (9.1%) high risk.
Based on the judgment of the risk of bias of the 17 NRCTs and NRNCTs, only one has a low risk in all its bias domains. The source of bias with higher risk is the missing data, where 75% of the studies have unclear risk because they do not explain how the missing data have been treated. The second source of bias is the selection of the participants. In this case, 43.7% of the studies have high risk and 31% of them have unclear risk, in most cases related to a poor description of the selection of the different cohorts of the studies.
Study characteristicsThe characteristics of the included studies are summarized in Table 3. Nine studies were published in 2021, 12 of them in 2022, and 7 in 2023. Eleven of the studies were RCTs (5 of them with active CGs), 5 NRCTs, and 12 NRNCTs. Two studies used a mixed method design, with quantitative and qualitative data. Nine studies included follow-up data, ranging from one to 6 months.
Table 3 Study characteristicsCharacteristics of the participantsThe characteristics of the participants are summarized in Table 3. The sample sizes of participants included in the 28 studies ranged from 13 to 643, with a higher percentage of women (74%). The participants included nurses, physicians, nurse assistants, physician assistants, and other health care workers (oral healthcare professionals, occupational therapists, psychologists, physiotherapists, pharmacists, technicians, and others). The largest proportion corresponds to nursing and medical staff (90%). Seven of the studies were carried out in the USA, 3 in India, 2 in Canada, 2 in China, and 1 in each of the following countries: Brazil, Indonesia, Iran, Italy, Japan, Kuwait, México, Saudi Arabia, Singapore, South Africa, Spain, Taiwan, Turkey, and the UK. The studies had been carried out in hospitals (52%), health care systems, primary care, medical centers, home-care settings, and academic health center settings.
Key themesThe key themes arose from the results of the articles (see Table 4), related to the characteristics of intervention (MBIs modalities, duration, sessions, in-person/virtual modality, trainer profile, follow-up…), the outcomes measures (standardized psychometric instruments used), and the MBIs effectiveness in the mental health areas (stress, burnout, anxiety, depression, sleep quality, resilience, mindfulness, mental well-being, fear of COVID-19, compassion, compassion satisfaction, self-compassion, loneliness, post-traumatic stress, work engagement, self-efficacy, satisfaction with life, quality of life, and empathy).
Table 4 Key themes extracted from the reviewed articlesCharacteristics of the interventionsThe characteristics of the interventions are summarized in Table 5.
Table 5 Characteristics and results of the interventionsSixteen studies focused their intervention specifically on mindfulness, understanding it as the use of different meditation strategies to achieve full awareness of the present moment. The tele-MBI carried out in the study by AlQarni et al. [45] included mindfulness of breath, movement, body sensations, emotions, thoughts, etc. Al Ozairi et al. [46] implemented a structured mindfulness meditation program adapted from the Mindfulness-Based Cognitive Therapy (MBCT), that incorporated breathing, sitting, sound, body-scan and walking meditations, and the promotion of compassion and kindness. The intervention performed in the study by Azizoddin et al. [47] was based on transcendental meditation and fundamentally consisted of the use of a repetitive mantra while the person is sitting with his/her eyes closed. The intervention carried out in the study by Franco and Christie [53] was an abbreviated adaptation for HCPs of the 8-week Mindful Self-Compassion (MSC) program developed by Neff and Germer [73]. The focus of the intervention was the development of self-compassion and included mindfulness, self-kindness, and the recognition of one’s common humanity. The 8-week Mindfulness Program, based on the foundations of the Mindfulness-Based Stress Reduction Program (MBSR), was applied by Gherardi-Donato et al. [54] and included different personal processes focused on breathing, the body, sensations, sounds, thoughts, and emotions. Hsieh et al. [55] applied a program based on gong meditation, so that the HCPs, lying on sleeping pads and covered with blankets, focused their attention on the sound of a gong with real-time adjusted rhythm. Ibrahim et al. [56] based their intervention on mindfulness breathing, a basic meditation technique focused on following the rhythm of breathing while inhaling and exhaling air. Headspace is the name of the mindfulness practice used in the study by Keng et al. [57], which includes introduction to mindfulness, mindful breathing, mindfulness of thoughts, and mindfulness of sounds, among others. Kim et al. [58, 59] applied a skill-based mindfulness program, called the Mindfulness Ambassador Program (MAP), which included mindful breathing, mindful listening, mind–body awareness, and paying attention and connecting authentically. Li et al. [61] applied a Brief Mindfulness Meditation (BMM) program, mainly focused on mindfulness breathing. Marotta et al. [63] used the MBSR [27], including mindfulness meditation, body awareness, and deepening behavior, thinking, feeling, and action. Nestor et al. [65] applied in their study a transcendental meditation technique. Osman et al. [67] analyzed the efficacy of the MBCT-4, a brief mindfulness program that includes meditations and breathing exercises. Prado et al. [69] used a mobile mindful meditation application that applies binaural beats (pure sounds, tones, and frequencies) dichotically through headphones. Thimmapuram et al. [70] evaluated the efficacy of heartfulness meditation, which includes heartfulness relaxation practice for meditation in the morning and heartfulness relaxation practice prior to sleep. The technique includes the conscious body scan and finishes by bringing our attention to the heart and the sensation of a light source emanating from it.
The other 12 studies combined mindfulness techniques with other types of interventions. Cao et al. [48] combined in their program Balint groups (meeting and support groups where they shared experiences, difficulties, emotions, thoughts, and proposed solutions) with MBSR (breathing, body scan, emotions, thoughts, loving-kindness, contemplation…). Cepeda-López et al. [49] conducted a mind-body-based intervention that included mindfulness-based stress reduction, single-focus meditation, self-regulation exercises (i.e., yoga qigong), breathing practices (i.e., diaphragmatic breathing), awareness practices, spirituality, and reframing strategies based on existential positive psychology (acceptance, letting it go…). DeTore et al. [50] included didactic information, experiential exercises, and testimonials from HCPs on resilience, mindfulness, and self-compassion in their intervention, based on cognitive-behavioral and mentalization techniques. Throughout the process, emphasis was placed on the implementation of this knowledge and skills in daily life, delving into the specific challenges that HCPs face during the COVID-19 pandemic. In the study carried out by Divya et al. [51], Sudarshan Kriya Yoga (SKY) was used, a method that combines controlled cyclical breathing and meditation, and which has its roots in traditional yoga. It includes awareness of breathing and controlled breathing with slow, normal, and fast rhythms. Fiol-DeRoque et al. [52] implemented a self-managed psychoeducational intervention focused on four fundamental areas: emotional skills, healthy lifestyle behavior, work stress and burnout, and social support, all based on cognitive-behavioral and mindfulness techniques. Mindfulness in Motion (MIM) is the name of the program developed in the research carried out by Klatt et al. [60], consisting of a mindfulness-based intervention that includes experiential mindfulness meditation and gentle yoga sessions. The Enhanced Stress-Resilience Training (ESRT) evaluated by Luton et al. [62] included mindfulness-based exercises, in addition to other techniques to deal with stress and burnout. The program carried out by Miyoshi et al. [64] combines mindfulness (sitting meditation, breathing meditation, body scan) and yoga exercises. Nourian et al. [66] used an online adaptation of the MBSR [25, 26]. The program included information on the nature of mindfulness, meditation practices, and yoga exercises. The protocol applied in the study by Pandey et al. [68] included yoga postures (Asanas), breathing regulation techniques (Pranayama), and meditation (Dhyana), which favor the achievement of a state of dissociation between oneself and disturbing thought or activities. The intervention carried out by Vajpeyee et al. [71] combined yoga sessions (which include meditation and deep breathing exercises) and music sessions (the participants could choose the type of music they preferred, and/or listen to instrumental music by Pandit VM Bhatt). Finally, Yildirim et al. [72] combined mindfulness-based breathing (focus on the breaths, on each part of the body, and on the emotions) and music therapy (light piano music as background music).
Regarding the modality of implementation, 4 interventions were carried out in-person through face-to-face sessions [53, 55, 63, 68], 20 in virtual/online format (through apps, WhatsApp, video files, audio files, reading files, tutorials, and/or phone conversations) [45, 46, 48,49,50,51,52, 54, 56,57,58,59,60,61, 64, 66, 67, 69, 70, 72], and 4 in a mixed modality [47, 62, 65, 71].
Regarding program integrity, it is worth highlighting that there is a great diversity of options. Thirteen of the interventions were conducted by expert and experienced trainers in mindfulness [47, 49, 51, 55, 58,59,60, 63, 65, 67, 70,71,72]. Five were carried out by health professionals (psychologists, psychiatrists, nurses, and doctoral level clinicians) experts in mindfulness [46, 48, 50, 52, 54]. At this point, it should be noted that, in the study by DeTore et al. [50], testimonials of HCPs about their experiences during the pandemic and their use of the skills learned in previous courses were also included. Two were developed by the researchers themselves [56, 62]. Two by the researchers together with psychologists and experienced trainers [64, 66]. And 6 of the studies do not indicate who prepared and/or carried out the intervention [45, 53, 57, 61, 68, 69].
Of all the studies, only 9 [47, 49,50,51, 53, 57,58,59, 65] included follow-u
留言 (0)