
記住我
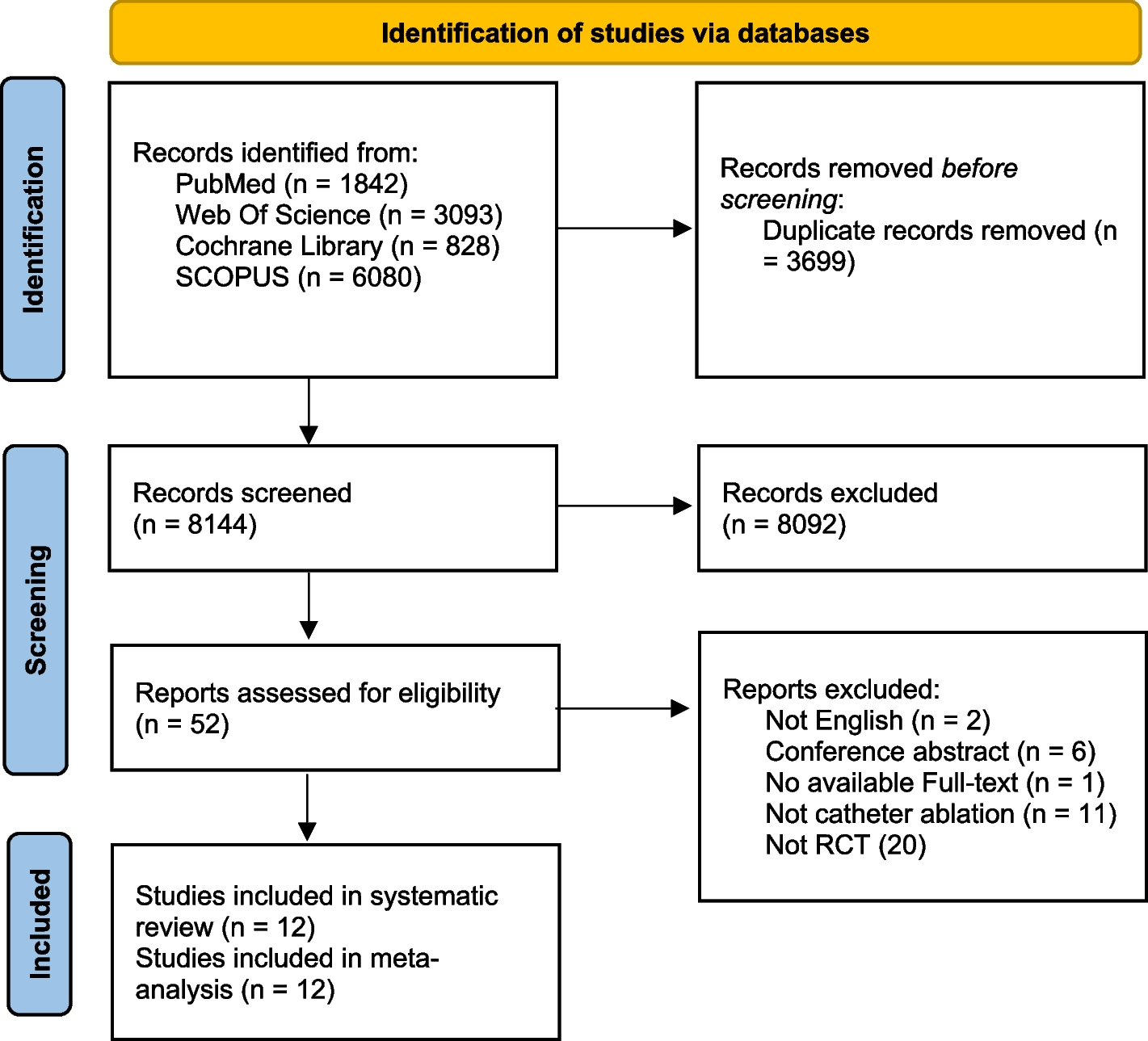
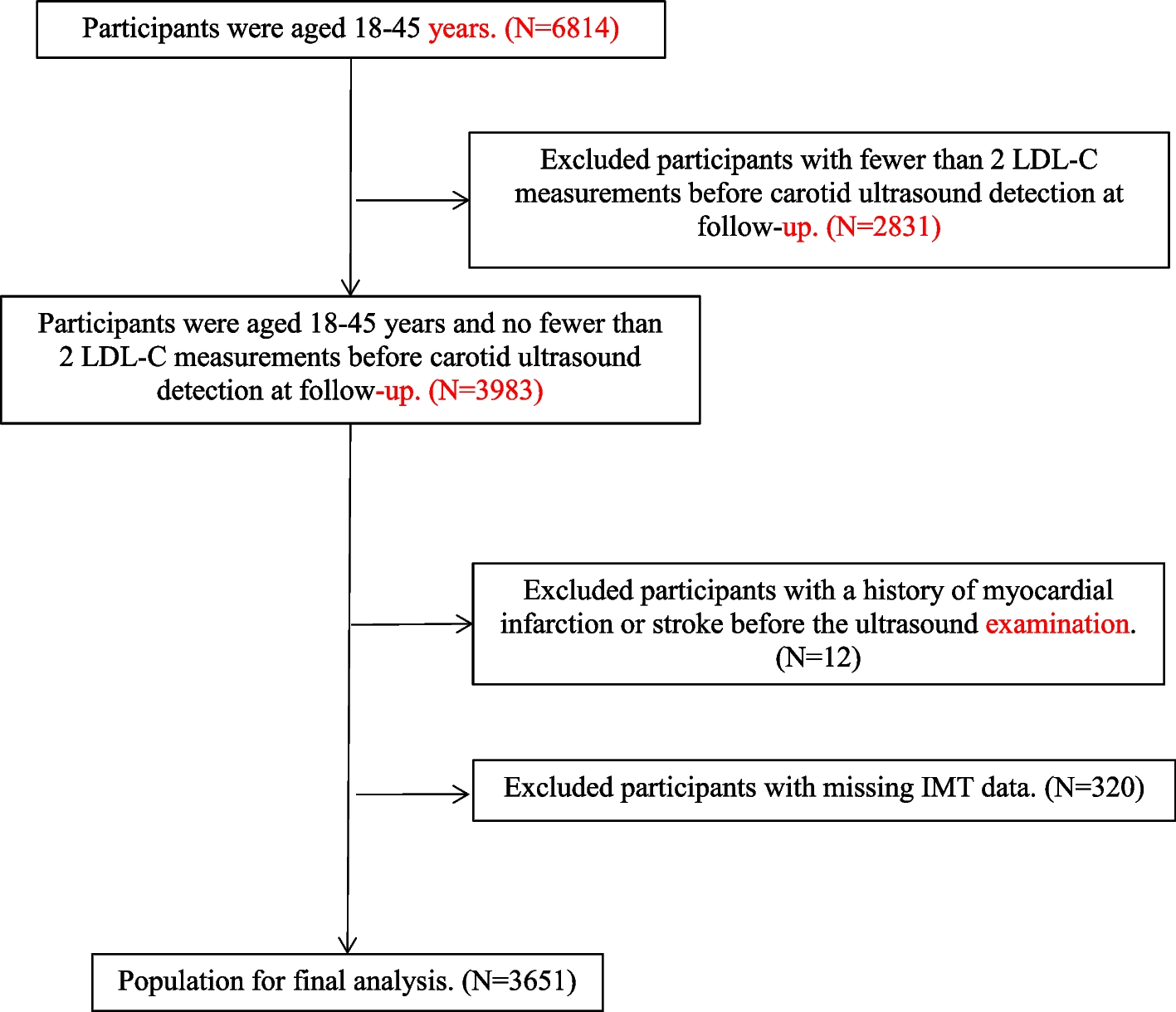

Figure 1 summarizes the screening process. We found 33 SLRs (Appendices 2 in the Data Supplement). All the included studies were published between 2013 and April 2024 in English. Overall, 22 SLRs collected their data only from Randomized Controlled Trials (RCTs), whereas 11 SLRs collected data from randomized and non-randomized studies and prospective or retrospective observational studies.
Fig. 1
Workflow for the selection of eligible studies following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria
Twenty-three studies considered elderly patients, over 65 years old. Sixteen studies included all surgical STS-risk patients. Low, low to intermediate, intermediate, and high risk were considered in 9, 2, 3, and 2 studies respectively. Figure 2 shows the evolution of the risk class of patients included in studies over time. Table 1 summarizes clinical outcomes results for TAVI compared to SAVR, whereas Table 2 summarizes complications regarding included studies.
Fig. 2
Distribution of risk classes included in studies per different years. The figure reports the number of studies including All risks of patients, high, intermediate, low to intermediate, and low risk distribution per year. *The year 2023 includes also one paper published in 2024
Clinical outcomesMortalityEarly mortalityEarly mortality is defined as mortality at 30 days or in-hospital in fourteen studies [6,7,8,9,10,11,12,13,14,15,16,17,18,19], as 3-month mortality in one study [20] and as 6-month mortality in another study [21]. Only one study did not define the time interval considered [22].
Early mortality was evaluated in eighteen out of the thirty-three studies included. Ten studies [6, 8, 9, 13, 15,16,17,18, 20, 22] found early mortality to be similar in both TAVI and SAVR groups. Five studies [10, 11, 14, 19, 21] found TAVI to be associated with lower rates of early mortality. In one study [7], early mortality for TAVI vs. SAVR was found to be lower in patients with chronic kidney disease (CDK), whereas another study [12] assessed better outcomes for TAVI vs. SAVR in women. Lastly, one study reported lower rates of early mortality for low-risk patients and similar rates for high-risk patients [23].
Late MortalityLate mortality was identified with mortality at 1 year of follow-up for most of the studies included [6, 8, 10,11,12, 15, 16, 20, 23,24,25] whereas five studies [13, 17, 18, 21, 26] considered two years. One study [19] reported late mortality for a follow-up period of 5 years. Two studies [14, 17] did not report the time interval for this outcome, and one study [22] considered more than 1 year.
Late mortality was evaluated in twenty out of the thirty-three studies included and was found to be similar between TAVI and SAVR in eleven studies [6, 8, 9, 11, 15, 17, 18, 20, 22,23,24,25,26]. One study [12] reported lower mortality rates for TAVI in medium-risk women. Two studies [10, 16] found TAVI to be associated with lower mortality overall, considering low surgical-risk patients. Four studies [13, 14, 19, 21] favoured SAVR over TAVI, all three including patients with all surgical risks. One study [23] found mortality to be lower for TAVI in patients with high surgical risk and similar to SAVR for low surgical risk patients.
All-Cause mortalityEleven studies evaluated all-cause mortality; four [24, 27,28,29] found that it was similar between TAVI and SAVR, whereas two studies [30, 31] reported a lower rate for TAVI in the first year and similar rates in the second year of follow-up. Two studies favored SAVR [32, 33], and one study [34] reported a lower mortality for TAVI in the first follow-up year, which becomes equal to SAVR in the second year until it worsens between years two and five.
Cardiac mortalityCardiac mortality was specifically evaluated in six out of the thirty-three studies included. Four [18, 24, 27, 35] studies found cardiac mortality to be similar between TAVI and SAVR. Two studies [29, 36] favored SAVR over TAVI and one [30] reported a lower rate for TAVI in the first year and similar rates in the second year of follow-up. One study [34] reported similar rates in the first year of follow-up, higher rates in the second year for TAVI, and similar rates until year five of follow-up.
Stroke and transient ischemic attacks (TIA)Twenty-four studies out of the thirty-three selected evaluated the risk of stroke. Sixteen studies [6, 8, 11, 13,14,15,16, 22, 24, 26,27,28,29, 34, 36,37,38] found the hazard for stroke to be similar between TAVI and SAVR. Two studies [9, 18] found TAVI to have a higher rate of stroke than SAVR, with the first study considering only high-risk surgical patients and the second one including patients with all risk classes. Four studies [21,
留言 (0)