Study design and participants
This was a retrospective cohort study, and data of patients with stroke were extracted from the National Health and Nutrition Examination Surveys (NHANES) database in 2007–2018. The NHANES is conducted jointly by the National Center for Health Statistics (NCHS) and the Centers for Disease Control and Prevention (CDC) that aims to assess nutritional and health status of noninstitutionalized population in the United States. It includes a complex, multistage stratified probability sample on the basis of selected counties, blocks, households, and persons within households. Information was collected through interviews in participants’ homes that conducted by the NCHS well trained professionals, and extensive physical examinations conducted at mobile exam centers (MECs). For details please visit: https://www.cdc.gov/nchs/nhanes/index.htm.
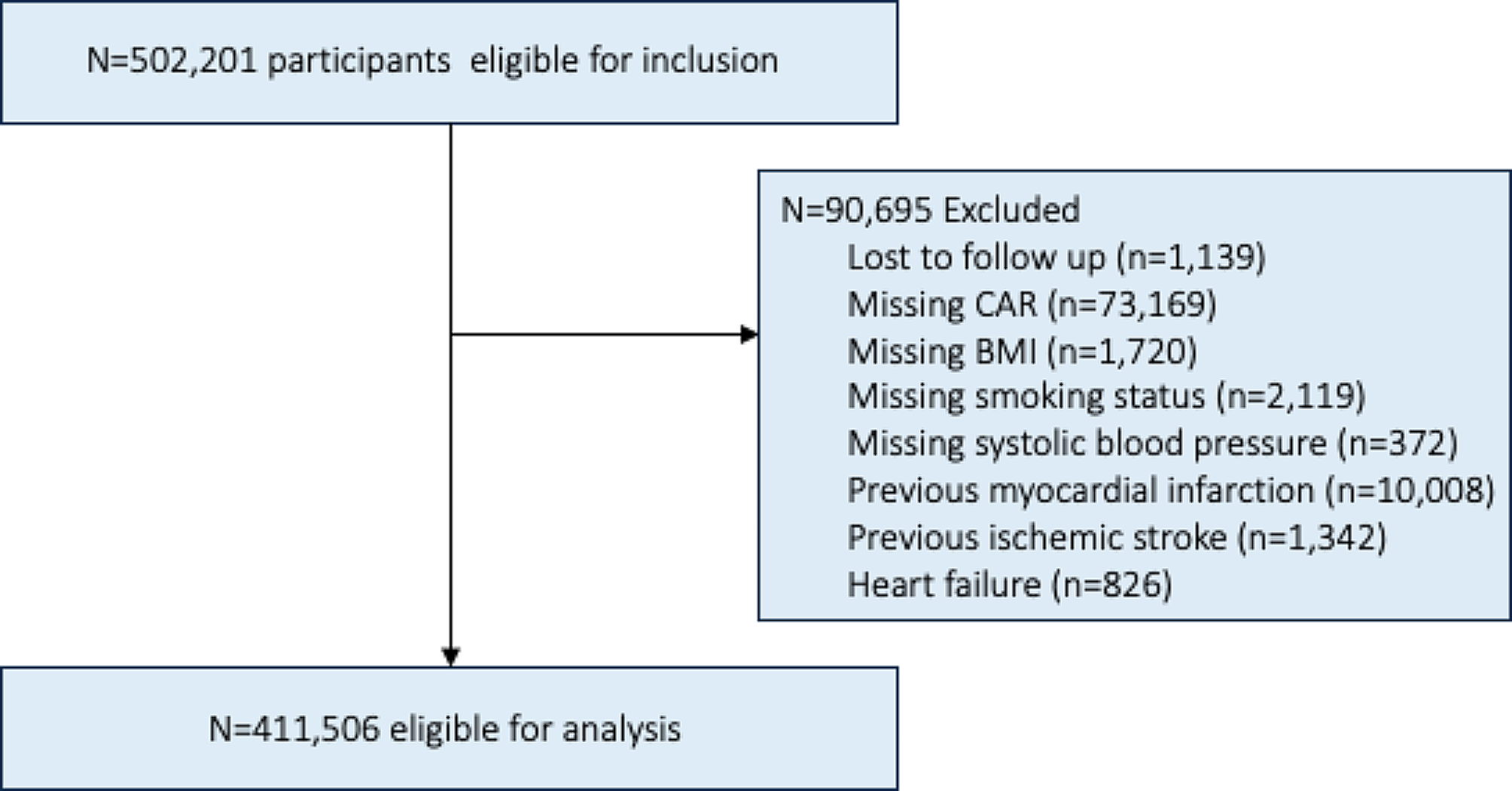
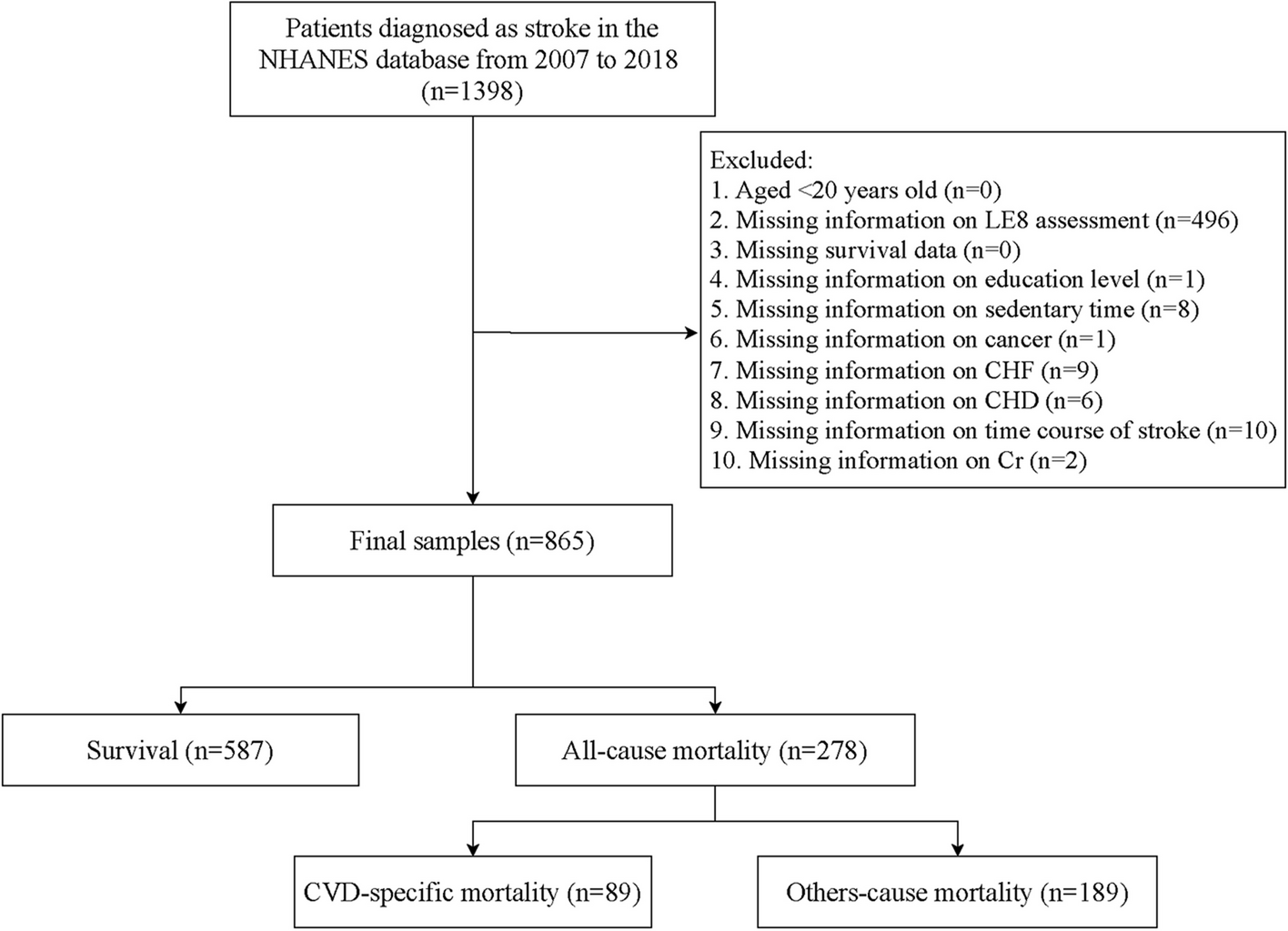
There were 1,398 individuals diagnosed as stroke in the database. The exclusion criteria were (1) aged < 20 years old, (2) missing information on LE8 assessment, (3) missing survival data, and (4) missing information on study variables including education level, sedentary time, cancer, congestive heart failure (CHF), coronary heart disease (CHD), time course of stroke and cotinine. Finally, 865 patients were eligible. The NHANES survey has been approved by the institutional review board (IRB) of the NCHS, and all the participants have provided informed consent. The requirement of ethical approval for this study was waived by the IRB of Jinling Hospital, Medical School of Nanjing University, because this database was publicly available. In addition, all study methods were performed in accordance with the relevant guidelines and regulations.
Measurement of LE8
The LE8 score is composed of four health behaviors (including diet quality, physical activity, tobacco exposure and sleep duration) as well as four health factors (BMI, non-high-density-lipoprotein cholesterol [non-HDL-C], blood glucose and blood pressure). Detailed algorithms for calculation of the LE8 scores for each of the metrics to NHANES data have been shown elsewhere [13]. Briefly, each of the eight factors was scored ranging from 0 to 100 points, and the unweighted average of these factors were used to calculate the overall LE8 score. Therefore, a higher LE8 score represents a better health condition. In the current study, we categorized the LE8 score (< 48.13, 48.13–58.75 and ≥ 58.75), health behaviors (< 43.75, 43.75–61.25 and ≥ 61.25), and health factors (< 47.50, 47.50–62.50 and ≥ 62.50) into three levels according to their tertiles respectively [7].
In addition, we calculated the contribution of each component in LE8 to reflect importance rank of these variables. To be specific, random forest models were established to analyses associations of each component in LE8 with all-cause mortality and cardio-cerebrovascular mortality respectively, and using variable importance (VIMP) method to rank the importance of these components. The VIMP calculated the difference value of error rate in models before and after inclusion of the variables. If a variable had a VIMP value < 0 represents it reduced the accuracy prediction of the model. Also, the larger the VIMP value, the greater the impact of this variable on the accuracy of the model, and the greater the importance of this variable.
Variables selection
We also extracted variables from the database as potential covariates, including age, gender, race, education level, marital status, poverty income ratio (PIR), heavy alcohol drinking, sedentary time, hypertension, dyslipidemia, DM, depression, cancer, CHF, CHD, anticoagulants, antiplatelet agents, sleep duration, time course of stroke, height, weight, BMI, waist circumference, systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), low-density-lipoprotein cholesterol (LDL-C), HDL-C, non-HDL-C, triglyceride (TG), fasting glucose, glycosylated hemoglobin (HbAlc), creatinine (Cr), estimated glomerular filtration rate (eGFR) and the Healthy Eating Index (HEI)-2015.
In the LE8 scoring algorithm, diet quality was evaluated using the HEI-2015. The NHANES collected dietary intakes of participants via two 24-h dietary recalls, and was combined with the United States Department of Agriculture (USDA) food patterns equivalents data to construct and calculate the HEI-2015 scores [14]. Information on heavy alcohol drinking (≥ 8 drinks/week) was collected by self-report questionnaires [15]. DM, dyslipidemia, and hypertension were estimated through laboratory examination, self-report, or medication history: participants with fasting blood glucose ≥ 7.0 mmol/L or HbAlc ≥ 6.5% or self-reported DM or receiving hypoglycemic therapy were considered as DM patients; dyslipidemia referred to TC ≥ 200 mg/dL (5.2 mmol/L) or TG ≥ 150 mg/dL (1.7 mmol/L) or LDL-C ≥ 130 mg/dL (3.4 mmol/L) or HDL-C ≤ 40 mg/dL (1.0 mmol/L) or self-reported hypercholesterolemia or lipid-lowering therapy; hypertension was defined as self-reported high blood pressure or SBP ≥ 130 mmHg or DBP ≥ 80 mmHg or taking hypotensive drugs [16]. In addition, cancer, stroke, depression were also assessed via the NHANES questionnaires [17].
Height, and weights were measured during the physical examination in MECs. The BMI was calculated as the weight in kilograms (kg) divided by the height in meters squared (m2). According to the World Health Organization (WHO) standard, we divided BMI into underweight (< 18.5 kg/m2), normal weight (18.5 kg/m2 ≤ BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2), and obesity (BMI ≥ 30 kg/m2). Besides, the cut-off value for high waist circumference was 88 cm for females and 102 cm for males [18]. Also, the blood samples were collected and sent to central laboratories for the determination of hematological indexes in the NHANES.
Study outcomes and follow-up duration
The study outcomes were all-cause mortality and cardio-cerebrovascular mortality. The NHANES public-use linked mortality file as of December 31, 2019, which was correlated with the NCHS with the National Death Index (NDI) through a probability matching algorithm was used to determine the mortality status of the participants (https://ftp.cdc.gov/pub/health_statistics/NCHS/datalinkage/linked_mortality/). Of which, dying from arbitrary cause was recognized as all-cause mortality, whereas dying due to “disease of heart” (I00-I09, I11, I13, I20-I51) or “cerebrovascular diseases” (I60-I69) was considered as cardio-cerebrovascular mortality. Moreover, the follow-up ended when participants died or at December 31, 2019.
Statistical analysis
Normally distributed continuous data were described using mean ± standard error (mean ± SE), and t test was used for comparation between survival group and all-cause mortality group. Categorical data were expressed as frequency and constituent ratio [N (%)], and chi-square test (χ2) was used for comparison. Due to we included information collected from two 24-h dietary recalls, special weights “dietary two-day sample weight (WTDR2D)” should be used according to the NHANES guideline. The WTDR2D weights were constructed by taking the MEC two-year cycle sample weights (WTMEC2YR), and further adjusting for (a) the additional non-response and (b) the differential allocation by day of the week for the dietary intake data collection.
Weighted univariate COX regression analyses were used to screen the covariates associated with all-cause mortality and cardio-cerebrovascular mortality respectively. Weighted univariate and multivariate COX regression analyses were employed to investigate the association of LE8 with all-cause mortality and cardio-cerebrovascular mortality in patients with stroke. Also, these relationships were assessed in subgroups of age, gender, BMI, cancer, and CHD. Model 1 was unadjusted model. Model 2 adjusted for demographic and socioeconomic factors, including age, gender, race, educational level, marital status and PIR. Model 3 additionally adjusted for selected covariates on the basis of Model 2. The evaluation indexes were hazard ratios (HRs) and 95% confidence intervals (CIs). Two-sided P < 0.05 was considered significant. Statistical analyses were performed by SAS 9.4 (SAS Institute, Cary, NC, USA) and R version 4.2.3 (Institute for Statistics and Mathematics, Vienna, Austria).


留言 (0)