Several studies have explored the electrophysiological characteristics of PVCs with successful ablation sites in the RCC and the right–left sub-valvular interleaflet triangle [6,7,8]. However, the electrophysiological characteristics and catheter ablation of PVCs originating from SSLV have not yet been fully characterized. There were three major findings for SSLV-PVCs in this study. First, SPs were recorded not only in PVCs with narrow QRS duration, but also in PVCs with wide QRS duration. Second, PVCs showed narrow QRS duration in five (13.5%) of 37 patients and the SP-V interval during PVCs was significant longer than that during sinus rhythm. Third, the mapping points and number of RFCA applications needed to terminate the PVCs were increased in PVC without SPs at the earliest activation site.
In this study, SPs were observed in five patients with PVCs showing a narrow QRS complex and in seven patients with PVCs showing a wide QRS complex. SPs were not observed in 25 patients with PVCs showing a wide QRS complex. Chen et al. reported that sharp, high-frequency and presystolic potentials were observed in PVCs originating from proximal left anterior fascicle (LAF), which presented narrow QRS duration and could be successfully ablated from the RCC [6]. Hachiya et al. reported that an isolated spiky prepotential could be observed at the successful ablation site for PVCs with a wide QRS duration, which could be successfully ablated from the RCC and a dead-end tract (DET) was a plausible explanation for these discrete prepotentials [5]. In our study, SPs could be recorded on successful ablation sites for PVCs originating from the SSLV. Although we did not confirm whether these low amplitude and high-frequency potentials represent the activation of the myocardium or His-Purkinje system in the SSLV, it is important to understand if SPs would be a sufficient indicator for successful ablation of PVCs with different QRS durations [9].
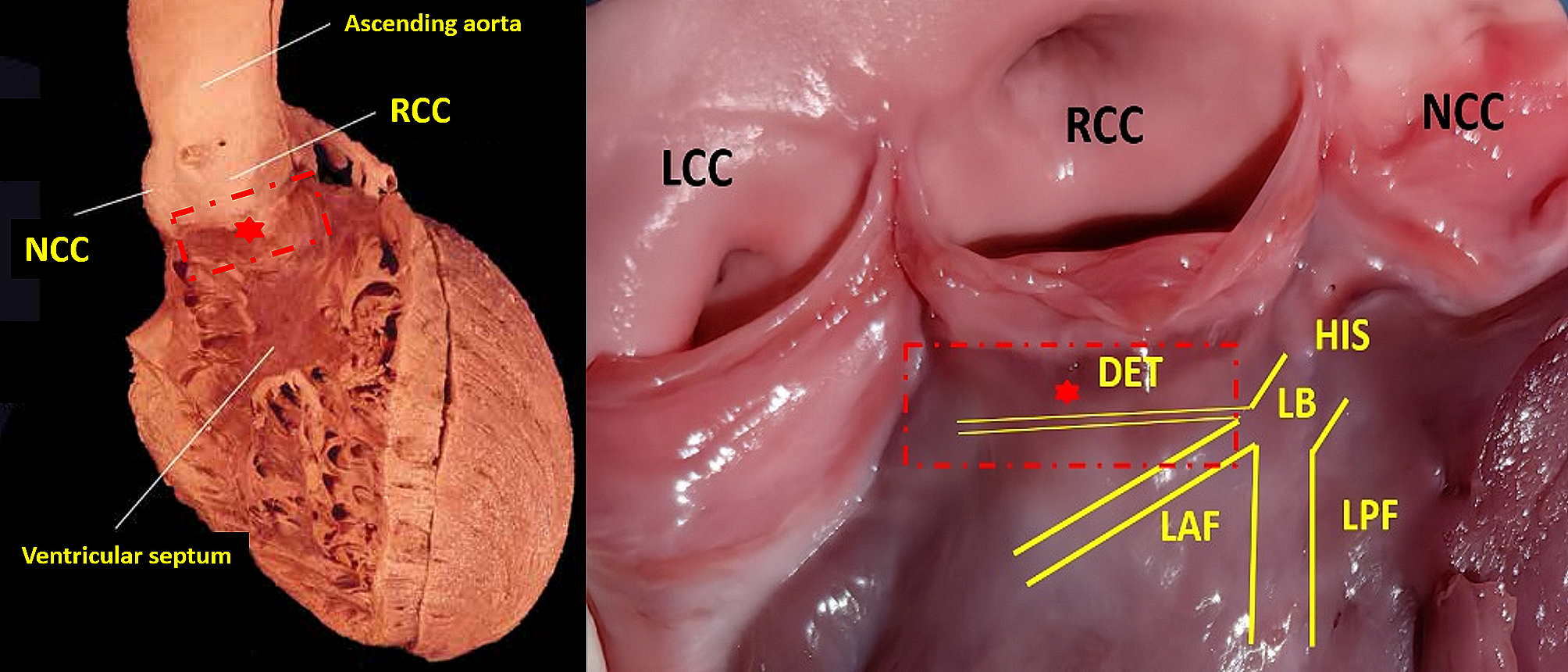
In our patients with PVCs showing a narrow QRS complex, SPs occurring slightly before the ventricular electrogram with an isoelectric line were recorded at the SSLV. The route of the DET and the proximal LAF lies within the anatomical structure of the SSLV [10,11,12]. Furthermore, the characteristics of these recorded potentials seem to be qualitatively similar to those of the His-Purkinje origin. Therefore, the LAF or DET might have been sites of origin for the ectopic arrhythmia foci in our study. Previous studies have reported that SPs in the SSLV represent the proximal LAF and that the SP-V interval in sinus rhythm is equal to the SP-V interval of PVCs at the earliest activation site for PVCs originating from LAF [6, 13]. Jinglin Z et al. reported that SPs in the SSLV represent the activation of DET, with the SP-V interval in sinus rhythm showing no difference from the SP-V interval of PVCs at the earliest activation site [3]. In our study, the SP-V interval in sinus rhythm was significantly shorter than that of PVCs at the earliest activation site. We deduced that the ectopic focus was only electrically connected the distal LBB or the proximal LAF, having no electrical connection with the ventricular myocardium. Premature contraction activates the His-Purkinje system and ventricular myocardium by reverse conduction to the distal LBB or proximal LAF, resulting in a shorter SP-V interval in sinus rhythm at the earliest activation site than that of the PVCs (Fig. 3). Therefore, DET, instead of the proximal LAF, seemed to be the true origin of these PVCs.
In the patients without SPs recorded in the earliest activation site for PVCs mapping, the PVC morphologies presented a wide QRS duration. More mapping areas were needed than those for the patients with SPs recorded in the SSLV to identify an arrhythmogenic focal source. Accordingly, the adjacent anatomic area of mapping included the LCC, RVOT, and GCV in many patients without SPs recorded [14, 15]. Furthermore, SPs were observed in seven patients with PVCs showing a wide QRS complex in our study. In contrast to the PVCs without SPs recorded in the earliest activation site, it is easy to achieve the successful elimination of PVCs. We speculated that the Purkinje fibers might be the real source of the ectopic activity, which is not electrically connected the distal LBB or the proximal LAF but rather to the ventricular myocardium of the SSLV. In this situation, PVCs presented wide QRS durations and were easily eliminated with RF applications. Certainly, further basic research is needed for better understanding of the real origin of such SPs. Furthermore, high density mapping catheter is very important to collect a greater amount of data for SPs. However, high density mapping catheter manipulation is more easily than catheter ablation in resulting in mechanically induced PVCs and mechanical suppression of clinical PVCs. In the near future, it is hoped that high density mapping will enter clinical prime time for PVCs mapping and ablation.
Study limitations
First, the SP, seemingly originating from the conduction system, was only recorded at the SSLV. However, there is no direct evidence indicating that the SPs represent DET, the proximal LAF, or myocardium. Additional studies are necessary to elucidate this mechanism. Second, this study did not include unsuccessful cases. Regarding the unsuccessful cases, we found that no SP was observed in the SSLV. Third, it was the small number of population and a single center non-randomized analysis. Further population-based data are required to clarify the actual prevalence of SPs in the SSLV.


留言 (0)