Study participants and ethics
Twenty-three patients were enrolled from among outpatients at the Movement Disorders clinic of the Foundation IRCCS Ca’ Granda Ospedale Maggiore Policlinico of Milan, Italy. The entire sample (n = 20) included patients diagnosed with focal dystonia (n = 11; 67.9 ± 8.8) according to validated criteria, specifically cervical dystonia (n = 2), blepharospasm (n = 6), and hemispams (n = 3), and patients diagnosed with primary focal hyperidrosis (n = 9; 39.8 ± 10.6) as control group. Hyperhidrosis is a disorder characterized by excessive sweating in specific areas of the body, for example, hands’ palms, the soles of the feet or the armpits, which causes discomfort, embarrassment and may lead to serious psychological, social and occupational impairments. Exclusion criteria were generalized and secondary forms of dystonia. Demographic and clinical data, including age, educational level, disease duration and gender were collected (Table 1). The experimental procedure was approved by the local institutional review board (Foundation IRCCS Ca’ Granda Ethics Committee) and was conducted in accordance with the Declaration of Helsinki. All patients were informed of the purpose of the study and written informed consent was obtained from all participants.
Psycho-social correlates assessment
All patients underwent one evaluation of psycho-social correlates before botulinum toxin treatment (baseline) by performing the following tests: the Beck Depression Inventory II (BDI-II), the 36-Item Short Form Health Survey (SF-36), the Body Uneasiness Test (BUT), the State-Trait Anxiety Inventory (STAI) and the Visual Analogue Scale (VAS). After four weeks from botulinum toxin injection only VAS was administrated by telephone in order to assess whether BoNT therapy induced changes on psychological and social symptoms in patients diagnosed with focal dystonia.
Assessment scales
The Beck Depression Inventory II (BDI-II) (Beck et al. 1996) was performed to evaluate the presence and severity of depression. It is a self-report questionnaire consisting of 21 items ranging from 0 to 3. Higher total scores indicate more severe depressive symptoms. The cut-offs are the following: 0–3 for minimal depression; 14–19 for mild depression; 20–28 for moderate depression; 29–63 for severe depression.
The 36-Item Short Form Health Survey (SF-36) (Brazier et al. 1992) is an instrument composed of 36 questions assessing the quality of life (QoL) and the general state of health. The reference values range from 0 (total health impairment) to 100 (total well-being state). The assessed domains are: Physical Functioning (PF); Role-Physical (RP); Bodily Pain (BD); General Health (GH); Vitality (V); Social Functioning (SF); Emotional Role (ER); Mental Health (MH).
The Body Uneasiness Test (BUT) (Cuzzolaro et al. 2006) was used to evaluate body dissatisfaction index and the presence of depersonalization and derealization symptoms towards one’s body. This self-rated questionnaire includes 34 items whose scores on a Liker Scale range from 0 (never) to 5 (always). It provides several scores or index: in addition to the total scores, the Global Severity Index (GSI) identifies the degree of severity correlated to one’s body self-image. It includes 5 subscales or factors: Weight Phobia (WP); Body Image Concerns (BIC), Compulsive Self-Monitoring (CSM); Avoidance (A); Depersonalization (D).
The State Trait Anxiety Inventory (STAI) (Spielberger et al. 1970) is composed of 40 items, 20 of which assess state anxiety and trait anxiety. State anxiety refers to an emotional state at a given moment, while trait anxiety is referred to a personological characteristics. Specifically, this instrument is composed of 20 questions with scores ranging from 1 to 4 for each item (almost never, sometimes, often, always) (Spielberger 1994). The final total score varies from 20 to 80: 80 − 71 for very high level; 70 − 51 for medium-high level; 50 − 31 for medium-low level; 30 − 20 for very low level or none.
The Visual Analogue Scale (VAS) is an instrument in which 11 items were processed for the assessment of subjective variations in worry and satisfaction with body image aspects and self-distress related to disease. It consists of a line usually 100 mm in length in which 0 indicates the minimum and 10 indicates the maximum, and the patient makes a mark reflecting its own perception.
StatisticsBackground analyses
Due to the restricted sample size, baseline between-group comparisons were run via Mann-Whitney’s tests. Similarly, the association between psychological measures at T0 and the change in each VAS item (computed as the raw difference between T1 and T0 scores; VASΔ) were explored, separately for the two groups, by means of Bonferroni-corrected Spearman’s correlations.
Effects of BoNT treatment on VAS scores
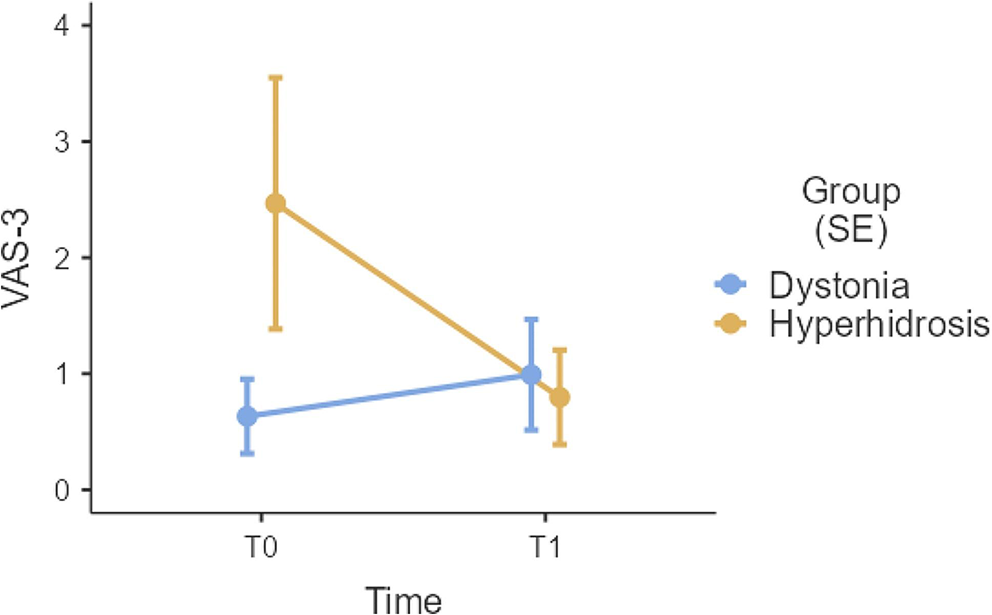
VAS − 3 and − 10 scores were reversed since, at variance with remaining ones, these items were negatively oriented.
Data distribution was then checked on raw VAS scores both by assessing skewness and kurtosis values (judged as abnormal if >|1| and >|3|, respectively [Kim 2013]) and by visually inspecting histograms and Q-Q plots. With the exception of VAS items 10 and 11, which distributed Normally, remaining ones were heavily right-skewed and overdispersed. Accordingly, linear models were employed when addressing VAS items 10 and 11, whilst generalized linear models underlying a Negative Binomial (Green 2021) distribution were employed for VAS items 1 to 9.
In order to test the effects of Time, Group and their interaction, linear/generalized linear mixed models were run separately on each VAS item by addressing Subject as the cluster, Time as the within-subject factor and Group as the between-subject factor. A random intercept was fitted within the Subject cluster. Bonferroni-corrected post-hoc comparisons were run for significant terms.
Analyses were run via IBM® SPSS® Statistics 29 (IBM Corp. 2023) and Jamovi 2.3 (The Jamovi Project 2022). Significance thresholds were Bonferroni-corrected whenever appropriate.




留言 (0)