
記住我


Crohn's disease (CD) comprises a group of chronic, immune-mediated diseases of the gastrointestinal tract (1). In CD, various cytokines are believed to be involved in the excessive activation of T cells in the intestinal mucosa (2,3). These inflammatory substances may affect not only the intestines but also other organs. Lymphoid tissue tends to accumulate in the spleen, consisting of a substantial number of B lymphocytes and T lymphocytes, and often enlarges during various inflammatory states, which closely correlates with immune responses (4). The spleen has a wide range of functions; for instance, it can serve as the body's larger filter of blood, produce white blood cells and antibodies, and remove microorganisms and old red blood cells (5). These different functions of the spleen predispose it to be related to many diseases, such as immunological, infectious, hematopoietic, and oncological diseases. Typically, the involvement of different diseases alters the morphology of the spleen, such as its size and margin (5,6). Although some studies have examined the correlation between disease activity and spleen size, these investigations have been limited in scope and conclusions (7,8).
Anti-TNFα therapies have been well studied in adults and have shown efficacy in both the induction and maintenance of remission (9). Anti-TNFα (infliximab [IFX]) treatment has been used for 20 years. In the ACCENT-I study, 58% of patients with CD who experienced a clinical response after the first dose of IFX were randomized, and the IFX 5-mg/kg and 10-mg/kg regimens were more effective at achieving clinical remission at week 54 than the placebo treatment (10). Although IFX is effective in patients with CD, the loss of response to IFX increases over time. A review showed that 60%–87% of patients receiving anti-TNF agents could achieve clinical remission or partial response in the induction phase, whereas less than 40% of patients maintain clinical remission at 1 year (11).
Radiomics has been found to help in assessing disease prognosis, disease activity, and diagnosis. For instance, Gao et al reported that an automated segmentation model constructed by computed tomography enterography (CTE) radiomics accurately segmented CD lesions and distinguished CD activity well (12). CTE radiomics is effective for the differential diagnosis of CD and intestinal tuberculosis; moreover, radiomics can predict surgery, postoperative anastomotic recurrence, and response to IFX during the course of CD (13–16). In summary, the use of radiomics, an emerging technology, is an effective approach for the management of CD. Radiomics can identify heterogeneity within tissues and use automated high-throughput feature extraction algorithms to convert image data into readable quantitative data (17); this transformation enables health care professionals to better comprehend the information embedded in images and apply it in clinical practice.
We used 3-dimensional (3D) slicer software to calculate radiological features of the spleen and determine whether these radiological characteristics can be used to assess disease activity and response to IFX in patients with CD. This investigation seeks to leverage imaging data to aid clinical treatment decisions.
MATERIALS AND METHODS Patient extractionAll patients diagnosed with CD between October 2020 and October 2022 were obtained from 2 hospitals from the First Affiliated Hospital of Nanchang University and Second Affiliated Hospital of Soochow University. The inclusion criteria were as follows: (i) patients diagnosed with CD based on clinical features, colonoscopy, imaging, and histological examination; (ii) patients with detailed CTE data recorded before patients received treatment with biological agents; and (iii) complete follow-up data. We excluded the following patients: (i) without a spleen, (ii) with incomplete or unavailable imaging data, (iii) patients with other spleen diseases, and (iv) patients with severe infectious diseases. For patients with missing clinical data such as perianal fistula data, we recorded the information through telephone follow-up. All patients in our study finished 4 treatments based on 5 mg/kg, and the response evaluation was completed in the fourth treatment. Finally, 113 patients from our center were randomly assigned to 2 groups at a 6:4 ratio: the training group (67 patients) and the testing group (46 patients); patients from the Second Affiliated Hospital of Soochow University were enrolled in the external group. The study flowchart is shown in Figure 1.
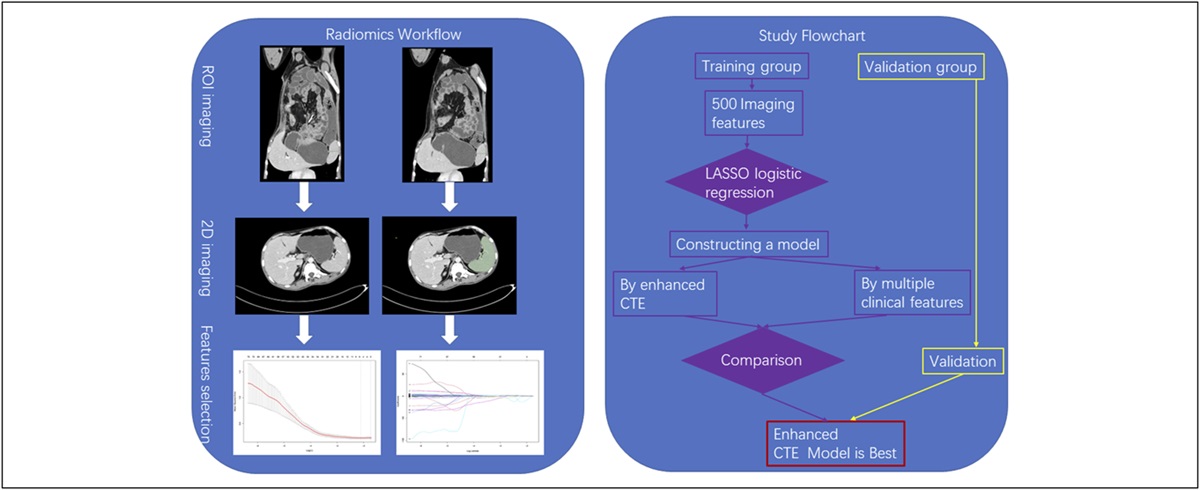
 Figure 1.:
Figure 1.: The flowchart of radiomics and the whole study.
Definitions of variablesIn our study, the following data were collected: (i) clinical characteristics, including age, sex, abdominal pain, diarrhea, bloody stools, fever, abdominal abscess, perianal abscess, intestinal fistula, and perianal fistula; (ii) CD-related features, including response to IFX, remission with IFX, mucosal healing, disease location, disease behavior, antituberculosis treatment, azathioprine treatment, Crohn's Disease Activity Index (CDAI) score, and duration of symptoms; and (iii) serum markers, including erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and T-SPOT. Patient characteristics are summarized in Table 1. Sex was recorded as male or female. Clinical features such as abdominal pain, diarrhea, bloody stools, and fever were classified as no or yes. Similarly, disease-related features such as response to IFX, remission with IFX, and mucosal healing were also divided into no or yes. T-SPOT results were recorded as negative or positive. ESR and CRP values were recorded as actual measurements. Montreal typing of CD included: based on age, A1: under 16 years old; A2: ages 16 to 40 years; and A3: over 40 years old; according to the location of the lesion: L1: end segment of ileum; L2: colon; L3: ileocolon; L4: upper gastrointestinal tract (clinically referring to the segment from the oral cavity to the duodenum); and divided by disease behavior: B1: non-narrow and nonpenetrating; B2: narrow; and B3: penetration. The response to IFX of patients with CD was the main variable observed in our study. According to the definition of clinical response, according to the update goals for IBD treatment (STRIDE II consensus), a clinical response was defined as a decrease of ≥50% in the abdominal pain score and stool frequency in patient-reported outcome 2 (PRO2), which was the short-term goal of IBD (18). In addition, for those who had no abdominal pain or diarrhea, we considered patients to have a clinical response if the CDAI was reduced by ≥100 (19,20). Therefore, in our study, we mainly assessed the clinical response according to the PRO2 score and adopted the standard of reducing the CDAI score by ≥100 for a small number of patients. Clinical remission in adult patients with CD was defined as a PRO2 abdominal pain score ≤1, a bowel frequency ≤3, or a Harvey-Bradshaw index, which are midterm goals. Endoscopic mucosal healing in patients with CD was defined as a simplified endoscopic score ≤3 for CD (18).
Table 1. - Basic information of extracted patients from First Affiliated Hospital of Nanchang University diagnosed in October 2020–August 2022 and from Second Affiliated Hospital of Soochow University in October 2020–August 2022 Variables Total Training group Testing group External testing P value Total, n (%) 175 67 (38.3) 46 (26.3) 62 (35.4) Sex, n (%) 0.721 Male 115 (65.7) 45 (67.2) 28 (60.9) 42 (67.7) Female 60 (34.3) 22 (32.8) 18 (39.1) 20 (32.3) Age, n (%) 0.534 ≤16 19 (10.9) 10 (14.9) 4 (8.7) 5 (8.1) 17–40 133 (76) 51 (76.1) 35 (76.1) 47 (75.8) ≥40 23 (13.1) 6 (9.0) 7 (15.2) 10 (16.1) Abdominal pain, n (%) 0.239 No 44 (25.1) 19 (28.4) 14 (30.4) 11 (17.7) Yes 131 (74.9) 48 (71.6) 32 (69.6) 51 (82.3) Diarrhea, n (%) 0.492 No 51 (29.1) 23 (34.3) 12 (26.1) 16 (25.8) Yes 124 (70.9) 44 (65.7) 34 (73.9) 46 (74.2) Bloody stool, n (%) 0.001 No 136 (77.7) 59 (88.1) 38 (82.6) 39 (62.9) Yes 39 (22.3) 8 (11.9) 8 (17.4) 23 (37.1) Fever, n (%) 0.736 No 139 (79.4) 55 (82.1) 35 (76.1) 49 (79.1) Yes 46 (26.3) 12 (17.9) 11 (23.9) 13 (20.9) SESCD.0 level, n (%) 0.748 2 36 (20.6) 12 (17.9) 9 (19.6) 15 (24.2) 3 82 (46.9) 35 (52.2) 22 (47.8) 25 (40.3) 4 57 (32.5) 20 (29.9) 15 (32.6) 22 (35.5) Responses, n (%) 0.654 No 70 (40) 28 (41.8) 20 (43.5) 22 (34.9) Yes 105 (60) 39 (58.2) 26 (56.5) 40 (63.4) Remission, n (%) 0.355 No 115 (65.7) 46 (68.7) 28 (60.9) 41 (66.1) Yes 60 (34.3) 21 (31.3) 18 (39.1) 21 (33.9) Mucosal healing, n (%) 0.469 No 165 (94.3) 62 (92.5) 45 (97.8) 58 (93.5) Yes 10 (5.7) 5 (7.5) 1 (2.2) 4 (6.5) Disease location, n (%) 0.059 Terminal ileum 28 (16) 7 (10.4) 9 (19.6) 12 (19.4) Colon 37 (21.1) 9 (13.4) 10 (21.7) 18 (29) Whole bowel 90 (51.4) 51 (76.1) 27 (58.7) 32 (51.6) Disease behavior, n (%) 0.284 Non-narrow and nonpenetrating 120 (68.7) 51 (76.1) 29 (63.0) 40 (64.5) Narrow 47 (26.7) 15 (22.4) 15 (32.6) 17 (27.4) Penetrating 8 (4.6) 1 (1.5) 2 (4.3) 5 (8.1) Antituberculosis, n (%) 0.307 No 149 (85.1) 59 (88.1) 36 (78.3) 54 (87.1) Yes 26 (14.9) 8 (11.9) 10 (21.7) 8 (12.9) AZA, n (%) 0.667 No 144 (82.3) 57 (85.1) 38 (82.6) 49 (79.1) Yes 31 (17.7) 10 (14.9) 8 (17.4) 13 (20.9) T-spot, n (%) 0.354 Negative 161 (92) 64 (95.5) 42 (91.3) 55 (88.7) Positive 14 (8) 3 (4.5) 4 (8.7) 7 (11.3) Abdominal abscess, n (%) 0.043 No 167 (95.4) 65 (97.0) 46 (100.0) 56 (90.3) Yes 8 (4.6) 2 (3.0) 0 (0.0) 6 (9.7) Intestinal fistula, n (%) 0.307 No 167 (95.4) 66 (98.5) 43 (93.5) 58 (93.5) Yes 8 (4.6) 1 (1.5) 3 (6.5) 4 (6.5) Perianal abscess, n (%) 0.677 No 152 (86.9) 59 (88.1) 41 (89.1) 52 (83.9) Yes 23 (13.1) 8 (11.9) 5 (10.9) 10 (11.3) Perianal fistula, n (%) 0.77 No 74 (42.3) 30 (44.8) 20 (43.5) 24 (38.7) Yes 101 (57.7) 37 (55.2) 26 (56.5) 38 (61.3) CDAI (mean ± SD) 230.24 (65.60) 227.67 (65.17) 229.06 (66.94) 241.2 (59.48) 0.296 ESR (mm/hr), M (P25, P75) 34.00 (17.00–61.00) 37.00 (13.50–61.50) 32.50 (23.25–59.25) 24 (9.5–56.4) 0.071 CRP (mg/L), M (P25, P75) 21.65 (3.73–56.30) 21.65 (5.44–55.79) 28.10 (2.41–69.38) 16.3 (5.8–56.3) 0.064 Duration of symptoms (mo), M (P25, P75) 10.00 (3.00–16.00) 13.00 (3.00–30.00) 8.00 (3.25–13.00) 5.5 (1–26) 0.157The P value was from the t test, nonparametric Wilcoxon test, or χ2 test for comparing baseline characteristics of all patients.
AZA, azathioprine; CD, Crohn's disease; CDAI, Crohn's Disease Activity Index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; T-SPOT, tuberculosis spot test; SES-CD, simplified endoscopic score for CD.
The radiomic workflow is illustrated in Figure 1. In this study, all patients underwent contrast-enhanced abdominal CTE scans that covered the entire spleen. The CTE examinations were performed using a Siemens SOMATOM Definition AS 128-slice spiral CT scanner. The CTE scan was conducted with the following parameters: 120 kV, 200 effective mAs, a collimation of 640.6 mm, a matrix of 512 × 512, a pitch of 0.8, and a gantry rotation time of 0.5 seconds. After the nonenhanced CT scan, 80–100 mL of nonionic contrast agent (370 mg I/mL, Pamir iodine, Bracco) was intravenously injected at a rate of 3.5 mL/s, followed by a saline flush (20 mL), after which a dynamic contrast-enhanced CT scan was performed. Images in the arterial phase and venous phase were obtained at 30 and 60 seconds, respectively. The slice thickness of the images was 1.0 mm. The CTE images in the arterial phase were retrieved for image feature extraction. The region of interest (ROI) for spleen lesions was semiautomatically segmented using 3D Slicer 5.0.3, and the ROI was selected on the slice with the largest spleen area. Texture extraction was performed using the radiomic tool 3D Slicer 5.0.3 to extract imaging features from 2-dimensional (2D) images of the spleen. ROI segmentation for spleen imaging was conducted by 2 clinicians with extensive experience in CT examinations. Then, the readers segmented the spleen and saved the results in the nrrd format. Then, another author used software to extract features. Furthermore, intraclass and interclass correlation coefficients were calculated to assess the consistency of the 2 readers in radiomic feature extraction.
Feature selection and radiomic signature constructionFor the feature extraction process, we first drew the ROI and downloaded the SlicerRadiomics data set. During analysis, we selected manual customization because we can determine feature classes such as firstorder, gldm, and glrlm. Then, we checked the wave-based features and resampled the voxel size to filter out some useless features. Finally, we output the data table. The LASSO algorithm was applied through the glmnet package in R software. According to this principle, we calculated the lambda (logλ = −2.15) and deleted the variables with a coefficient value of 0. The remaining variables were subsequently included in the model. A formula, which is shown in the Supplementary Digital Content (see Supplementary Material, https://links.lww.com/CTG/B97), was generated using a linear combination of selected features according to their respective least absolute shrinkage and selection operator coefficients; then, the formula was used to determine the risk score (named the radiomic score) for each patient to reflect the response to IFX in patients with CD.
Statistical analysisFor statistical analysis, patients extracted from our center were first divided into a training group and a testing group at a 6:4 ratio, whereas patients from another center were included for external validation. In addition, features were compared among the 3 groups. Differences in continuous variables were compared using the Mann-Whitney U test or independent t test, whereas comparisons of categorical variables were conducted using the χ2 test or Fisher exact test. To construct the nomogram, we simultaneously constructed a radiomic model and clinical feature model. For the model's performance and discriminative ability, we tested the Hosmer-Lemeshow goodness-of-fit test and plotted receiver operating characteristic curves to evaluate the model's classification ability. We used decision curve analysis (DCA) and a clinical impact curve (CIC) to evaluate the clinical net benefit of the predictive models. In addition, we conducted the DeLong test to calculate the significant differences in the models. All the statistical analyses were performed using R software, and the relevant software packages were obtained from the R software program website (https://cran.r-project.org/). A P value less than 0.05 was considered to indicate statistical significance for all analyses.
Our study was approved by Ethics Committee of the First Affiliated Hospital of Nanchang University ((2022)CDYFYYLK(06–025)). Informed consent was obtained from all the participants. All methods were performed in accordance with relevant guidelines and regulations.
RESULTS Basic patient informationAs shown by the flowchart (see Supplementary Figure 1, https://links.lww.com/CTG/B96), we enrolled 303 patients with CD treated with IFX as the first biological agent and excluded 128 patients based on our main aim. However, for some missing values, we imputed by performing multiple imputation, decreasing the loss of data. The detailed information is listed in Table 1. As shown in Table 1, 175 patients with CD were included. For sexual frequency, the distribution of patients with CD was mainly male. The number of patients with CD aged 17–40 years was obviously greater than that of patients with CD aged ≤16 or ≥40 years. Interestingly, more than 50% of patients with CD had abdominal pain and diarrhea. However, the frequency of bloody stool and fever was not as high as the incidence of abdominal pain. The incidence of intestinal fistula and abdominal abscess in patients with CD was very low, at less than 50%. Nevertheless, 13.1% of the patients had perianal abscess, and the percentage of patients with perianal fistula was greater (57.7%). In our study, the ratio of patients without narrow or penetrating bowel was the largest, followed by patients with narrow bowel, whereas patients with penetrating bowel were the lowest. The percentage of positive T-SPOT cells was 8%. Serological indicators such as the ESR and CRP concentration were obviously greater than the normal values. As shown by the CDAI, the mean CDAI score was 230.24, indicating that the patients with CD exhibited a moderate-to-severe activity period. Furthermore, the duration of symptoms was up to 10 months, and some patients may even experience symptoms within 3 years. In our study, the rate of clinical response after treatment with IFX was 60%, the rate of clinical remission was 34.3%, and the rate of endoscopic mucosal healing was only 5.7%.
Establishment of the nomogramAs shown in Figure 1, we performed our study according to the flowchart. Our patients were divided into training, testing, and external groups. The detailed characteristics of the patients in the training set and 2 validation sets are shown in Table 1. There were 67 patients, 46 patients, and 62 patients in the training group, testing group, and external group, respectively. Table 1 shows that the distribution was almost random, except for the number of patients with bloody stool and abdominal abscess because the P value was greater than 0.05. We used the Radiomics tool of 3D Slicer software to read the information of the 2D lesion, and we subsequently identified 500 imaging features for analysis. The interclass correlation coefficients of the readers ranged from 0.692 to 0.893, indicating favorable feature extraction reproducibility. Then, we performed least absolute shrinkage and selection operator logistic regression to identify the features, as shown in Figure 2a,b. A total of 20 features were used to construct the model. Next, we constructed a radiomic score calculation formula according to the weight coefficient of the features, which is presented in Supplementary Digital Content (see Supplementary Material 1, https://links.lww.com/CTG/B97). Finally, we determined the Akaike information criterion value of the nomogram by stepwise regression and selected the best Akaike information criterion value (Figure 2c). Furthermore, as shown in Table 2, we performed multivariate logistic regression analysis using clinical features and found that disease location, disease behavior, and duration of symptoms were associated with the response to IFX; simple terminal ileum type (L1) was associated with treatment with IFX, whereas penetrating (B3) and longer duration of symptoms were associated with poorer effects of IFX (Table 2). We subsequently constructed a nomogram plot for visualization (Figure 2d). For the interpretation of the nomogram built by CTE, each patient had several features, such as our formula, which were read by a 3D slicer; then, the radiomics score was determined according to our formula. Next, we constructed a vertical straight line and observed the risk of CD. Finally, we can diagnose CD with a concrete accuracy. Similarly, the interpretations of the nomograms were similar.
 Figure 2.:
Figure 2.: Texture feature selection was determined by LASSO logistic regression and conducted a nomogram. (a) Selection of the tuning parameter (λ) according to LASSO model through 10-fold cross-validation based on minimum criteria. Binomial deviances from the LASSO regression cross-validation procedure were plotted as a function of log (λ). The y axis indicates binomial deviances. The lower x axis indicates the log (λ). Numbers along the upper x axis represent the average number of predictors. Red dots indicate average deviance values for each model with a given λ, and vertical bars through the red dots show the upper and lower values of the deviances. The vertical black lines define the optimal values of λ, where the model provides its best fit to the data. The optimal λ value of 0.025 with log (λ) = 5.23 was selected. (b) LASSO coefficient profiles of the 850 texture features. The dotted vertical line was plotted at the value selected using 10-fold cross-validation in (a). (c) Radiomics nomogram predicts response of patients with CD in the training group. (d) Nomogram built by clinical risk factors predicts the response of patients with CD in the training group. CD, Crohn's disease; CTE, computed tomography enterography; LASSO, least absolute shrinkage and selection operator.
Table 2. - Univariate and multivariate logistic regression model for exploring the potential favorable factors of response for infliximab in patients with Crohn's disease Variable OR (univariable) OR (multivariable) age <40 — ≥40 3.97 (0.44–36.04, P = 0.220) Sex Male Female 0.80 (0.29–2.24, P = 0.671) ESR Normal — High 0.71 (0.25–2.04, P = 0.529) CRP Normal — High 1.84 (0.60–5.57, P = 0.284) Intestinal fistula No — Yes 4,242,598.95 (0.00–Inf, P = 0.992) Abdominal pain No — Yes 0.75 (0.25–2.24, P = 0.606) Perianal fistula No — Yes 1.44 (0.54–3.82, P = 0.467) Diarrhea No — Yes 0.48 (0.16–1.39, P = 0.177) Disease location L1 — L2 1.06 (0.20–3.54, P = 0.057) 0.98 (0.19–2.91, P = 0.07) L3 0.69 (0.20–2.88, P = 0.038) 0.79 (0.36–3.58, P = 0.041) Disease behavior B1 — B2-B3 0.89 (0.54–3.37, P = 0.048) 0.76 (0.34–2.97, P = 0.058) Duration of symptoms <12 — ≥12 0.22 (0.08–0.64, P = 0.005) 0.24 (0.08–0.69, P = 0.008)CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; OR, odds ratio.
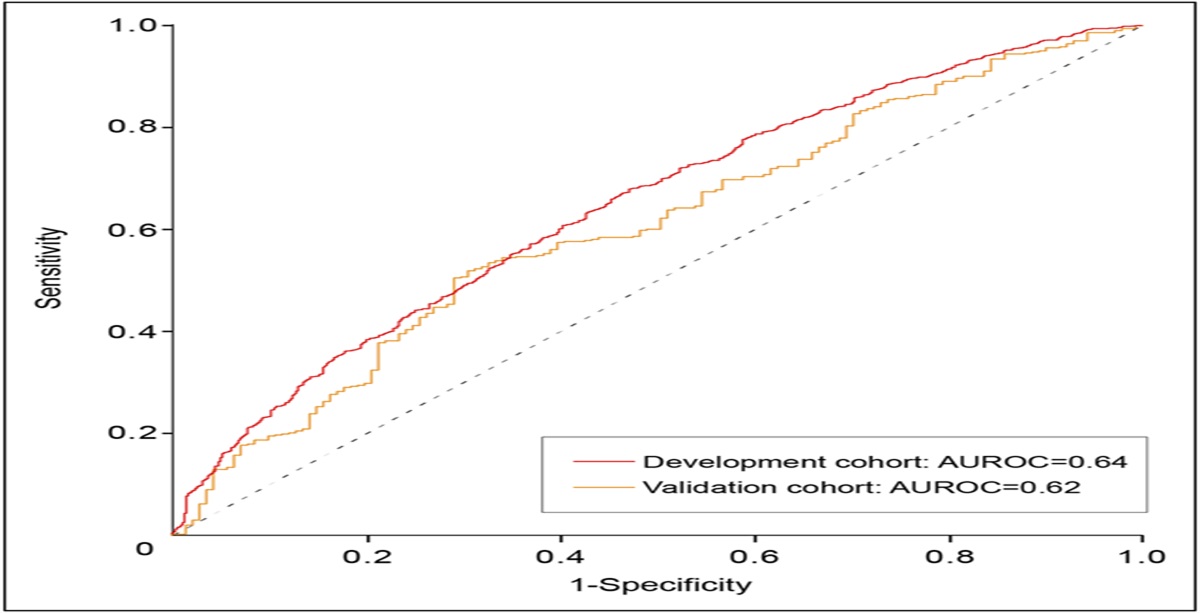
For the calibration plot, using the bootstrap validation method (n = 1,000), the nomogram model based on clinical risk factors showed good agreement with the actual values (Figure 3a); however, after validating the model in the testing group and external group, we found that the model had poorer consistency between the actual value and the predictive value (P > 0.05) (Figure 3b,c). Nevertheless, compared with the clinical risk model, both in the training group and in the 2 validation groups, our nomogram built by CTE showed good consistency between the actual value and the predictive value (P < 0.05; Figure 3d–f). Next, we compared the AUC of the receiver operating characteristic between the training set and validation set (Figure 3e,f). For both the training group and the validation group, the AUC of the nomogram built by CTE in the training group was almost the same as that in the testing group (training group, 0.909 [0.840–0.978]; testing group, 0.954 [0.889–1]; and external group, 0.902 [0.83–0.974]) (Figure 3g–i). In comparison, the nomogram built with clinical risk factors had poorer sensitivity and specificity both in the training set and in the validation set (training group, 0.712 [0.586–0.839]; testing group, 0.591 [0.412–0.770]; and external group, 0.697 [0.564–0.831], P < 0.05) (Figure 3g–i). As shown in Figure 4, DCA graphically showed that the use of the nomogram built by the CTE to predict response had remarkable predictive power (Figure 4a–c). In addition, the CICs of the nomogram indicated that the CTE model (Figure 4g–I) had more remarkable predictive power than the other models (Figure 4d–f). Finally, to investigate the clinical efficacy of our model, we analyzed the predictive value of the 2 models for clinical remission (Figure 5). Compared with that of the CTE model, the AUC of the prediction model of the nomogram built with clinical risk factors was significantly lower in the training cohort (AUC, 0.826 [0.706–0.899] vs 0.716 [0.528–0.801], P < 0.05) (Figure 5a), whereas the difference in AUC was not significantly meaningful in the validation cohort (AUC, 0.654 [0.506–0.731] vs 0.649 [0.518–0.713], P > 0.05) (
留言 (0)