
記住我


Dysphagia is a common symptom found in up to 16% of the population (1) and generally requires further evaluation to exclude structural disease (such as stricture, eosinophilic esophagitis, or malignancy). Yet, 29% of patients with dysphagia symptoms will have a normal upper endoscopy consistent with nonobstructive dysphagia (NOD) (2). At the index endoscopy, empiric esophageal dilation (EED) for NOD can be performed as a diagnostic and therapeutic maneuver targeting occult strictures that may improve with dilation. Visual size estimation by endoscopists is known to be imprecise (3), and it has been observed that abnormal barium esophagram findings can occur in up to 39.5% of cases after normal endoscopies (4). This practice remains controversial secondary to safety concerns and lack of efficacy data. Causes for NOD can include missed stenosis or esophageal dysmotility. In addition, little data exist about patient characteristics that may help guide patient selection for EED or of the coexistence of esophageal motility disorders in this population (5,6). Using 2 cohorts, we aimed to retrospectively examine the safety of large-caliber dilation and prevalence of esophageal motility disorders and prospectively examine symptomatic improvement in 2 large tertiary centers.
METHODS Participants and procedureEED is routinely offered to patients with dysphagia among a subgroup of clinicians practicing at the 2 anchoring tertiary referral hospitals in an academic hospital system. We evaluated 2 separate cohorts: (i) a larger retrospective cross-sectional analysis for assessment of real-world safety of EED in NOD, prevalence of tissue disruption defined as any mucosal break found after dilation or as noted by the endoscopists (as a measure of dilation efficacy, extrapolating from eosinophilic esophagitis literature (7)), and prevalence of concomitant motility disorders by high-resolution esophageal manometry (HREM) and (ii) a prospective observational cohort for assessment of EED efficacy and duration of symptom improvement after empiric dilation.
The retrospective cohort included adult (≥18-year-old) patients with dysphagia who underwent upper endoscopy and EED between January 2015 and April 2018 at 2 tertiary referral hospitals in (the United States) Boston, MA: Massachusetts General Hospital and Brigham and Women's Hospital. Patients in the retrospective arm were identified using the Research Patient Data Registry, along with data from clinical encounters, radiology, procedures, laboratory tests, medications, inpatient stays, operative reports, and billing records (8). We retrieved all patients who underwent EED (defined as any esophageal dilation for dysphagia in patients without a visible stricture or condition predisposing for obstructive dysphagia, as noted below) and had at least 3-month follow-up to ensure the validity of safety outcomes. We excluded patients dilated for obstructive dysphagia (such as eosinophilic esophagitis, previous esophageal or laryngeal surgery or radiation, endoscopically apparent strictures, or malignancy). Demographic, clinical, endoscopic, and manometric data were also obtained through manual chart review.
The prospective cohort was an observational unblinded single-arm cohort study that enrolled patients with NOD who consented for EED from 2018 to 2020. Otherwise, the inclusion and exclusion criteria were identical to the retrospective arm. If the endoscopists determined that no abnormality was present on upper endoscopy to explain symptoms, patients underwent empiric dilation. Dilator type and size were left to endoscopists' discretion, although mostly EEDs were performed with a single 60-Fr (20-mm) Maloney or Savary (bougie) dilator passed through the entire esophagus. Questionnaires assessing symptomatic response were administered at baseline (before EED) in person and through e-mail at 1, 3, and 6 months after dilation.
Primary variables of interestFor both the retrospective and prospective arms of the study, we evaluated demographic factors including age, sex, race/ethnicity, and relevant comorbidities that were believed to be associated with increased risk of esophageal dysphagia including history of anxiety, depression, pain syndrome (defined as fibromyalgia, migraine headache, musculoskeletal pain, etc), or use of neuromodulators (antidepressants, antipsychotics, and other central nervous system–targeted medications). We also collected data on the dilator size and any additional testing performed including HREM. As the normal esophageal diameter is at least 20 mm (with people becoming symptomatic when approaching a 13-mm diameter) (9), tissue disruption (presence of a tear after dilation) suggests successful treatment of a more subtle narrowing not noted during initial endoscopic evaluation.
OutcomesIn the retrospective arm, we explored the proportion of procedures with observed tissue disruption, adverse events (AEs), and postprocedure HREM diagnoses. Among those who also underwent HREM, we noted presence of Chicago V3.0 diagnoses that could be associated with dysphagia such as achalasia, esophagogastric junction outflow obstruction, distal esophageal spasm, and hypercontractile esophagus. These disorders were collectively defined as esophageal hypermotility disorders. We classified manometry diagnoses according to Chicago classification V3.0 as this was the most recent iteration available at data collection (before release of Chicago V4.0).
In the prospective arm, we used the National Institutes of Health Patient-Reported Outcomes Measurement Information System (PROMIS) gastrointestinal (GI) disrupted swallowing subscale to measure dysphagia (10). Patients self-reported dysphagia symptom frequency, severity, and impaction on a Likert 5-point scale: Possible answers were 0—never, 1—rarely, 2—sometimes, 3—often, and 4—always. A composite score is calculated as the sum of all responses, with a range from 0 to 28 where a higher score reflects being more symptomatic. Composite scores were then transformed into a T-score metric calibrated to the US population with a mean of 50 and SD of 10. We defined minimal clinical important difference as a 0.5-SD improvement as suggested by Norman et al (11), which is consistent with the minimal clinical important difference found for the other PROMIS GI subscales (12).
Our primary outcome was the total T-score improvement after EED. Secondary exploratory outcomes included comparing improvement in patients with vs without tissue disruption on the total T-score and the raw frequency score of the subcomponents. Recruitment occurred from 2018 through 2020 (terminated because of the COVID-19 pandemic's impact on endoscopy referral patterns).
This study was approved by our institutional review board (retrospective arm protocol number 2022P001266 approved on May 22, 2022, and prospective arm protocol number 2018P002327 approved on October 31, 2018).
Statistical analysisData were normally distributed, and we have summarized mean values and SDs for continuous variables and calculated proportions for categorical variables. We used t tests to compare continuous variables and χ2 statistics to compare categorical variables for baseline demographics, medical comorbidities, and outcomes of the retrospective cohort. In the prospective cohort, the primary quantitative endpoint, the PROMIS disrupted swallowing T-score, was analyzed in a mixed-model repeated-measures analysis with unstructured within-person covariance among the repeated assessments. Adjusted means for the T-scores at each study time point (1 month, 3 months, and 6 months after EED) were estimated by linear contrasts. A group-level random effect was considered, but zero variance was estimated. The mixed model accounted for missing data when participants withdraw. Statistical significance was defined by a 2-sided P-value of 0.05.
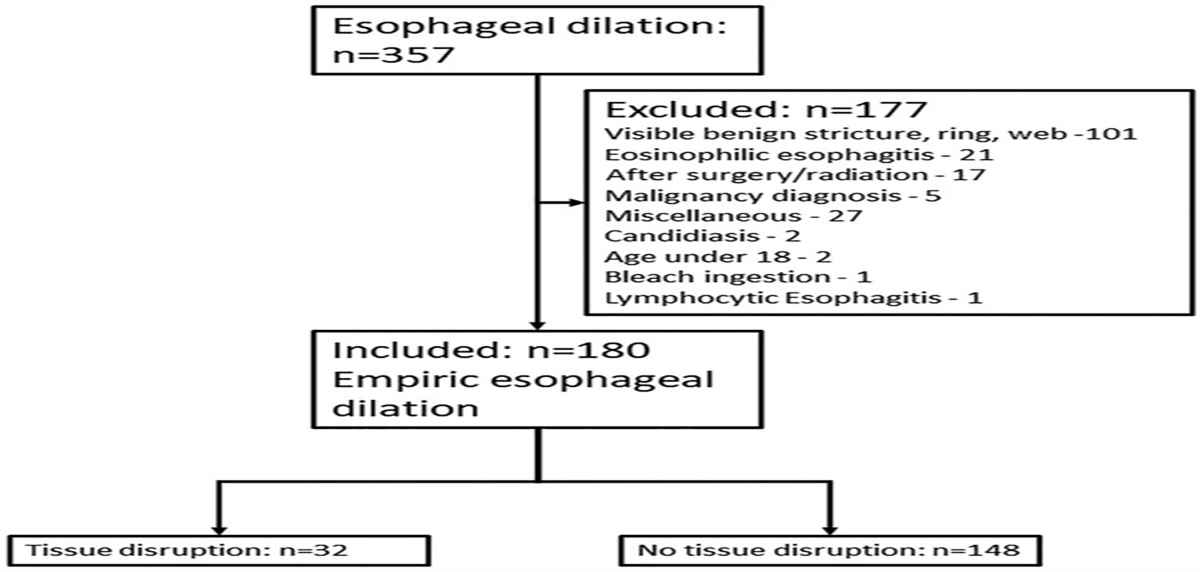
RESULTS Retrospective armThere were 357 patients who underwent esophageal dilation during the study period in the retrospective arm. We excluded 177 patients: 57% (n = 101) with endoscopically visible strictures or rings, 13% (n = 21) with eosinophilic esophagitis, and other reasons detailed in Figure 1. Exclusions left a total of 180 patients for analysis.
 Figure 1.:
Figure 1.: Retrospective arm flow diagram.* Miscellaneous reasons include patients who had an evidence of a stricture on a different endoscopy, inconclusive diagnosis of eosinophilic esophagitis, use of a 30-mm pneumatic balloon, and missing data.
The mean age of the cohort was 54.5 ± 14.9 years, and patients were predominantly white (87%) and female (70%). Endoscopic findings are described in Table 1 with 27% having endoscopic findings consistent with gastroesophageal reflux disease (i.e., having a hiatal hernia, esophagitis, or Barrett's esophagus). All esophageal dilations were performed with Maloney or Savary bougie dilators (the majority at least 58-Fr [19.3 mm] in diameter: 69%; more than 90% at least 50-Fr [16.7 mm] in diameter) (Table 1).
Table 1. - Baseline characteristics of the retrospective cohort Demographics (n = 180 unless otherwise noted) Age, yr, mean ± SD 54.4 ± 14.9 Female sex, % (n) 70 (126) Race, % (n) White 87 (157) Black 3 (6) Asian 2 (4) American Indian or Alaska Native 1 (2) Two or more 1 (1) Unknown/missing/other 6 (10) Ethnicity, % (n) Hispanic 1 (2) Bougie size (Fr), % (n) 60 (20 mm) 62 (112) 58 Fr (19.3 mm) or larger 69 (134) Under 60 (<20 mm) 38 (68) Under 50 (<16.3 mm) 9 (16) Endoscopic findings, % (n) Endoscopic GERD (HH/esophagitis/Barrett's) 27 (48) Hiatal hernia 15 (27) Esophagitis 11 (19) Barrett's esophagus 4 (7) Manometry diagnoses (N = 38), % (n) Normal 45 (17) Absent peristalsis 5 (2) Ineffective esophageal motility 29 (11) Esophageal hypermotility disorder 21 (8) Esophagogastric junction outflow obstruction 13 (5) Hypercontractile esophagus 3 (1) Distal esophageal spasm 3 (1) Achalasia (type 3) 3 (1) Comorbidities, % (n) Anxiety/depression 64 (116) Pain syndrome 64 (116) Neuromodulator use 47 (84) Anxiety/depression or pain syndrome 78 (140) Anxiety/depression, neuromodulator use, or pain syndrome 87 (156)GERD, gastroesophageal reflux disease; HH, hiatal hernia
Tissue disruption occurred in 18% (n = 32) of dilations, with no immediate bleeding requiring endoscopic treatment. All patients with tissue disruption had a bougie catheter sized 58 Fr (19.3 mm) or larger: 100% > 58-Fr dilator size (n = 32) vs 62% (n = 92) in those without disruption (P < 0.001). The location of the tissue disruption was the gastroesophageal junction in 53% (n = 17) and the proximal esophagus or upper esophageal sphincter in 47% (n = 15). One patient with gastroesophageal junction tissue disruption also had a milder laceration in their proximal esophagus. Furthermore, no differences were found in age, sex, demographics, or psychiatric comorbidities between patients with and without tissue disruption after EED (Table 2, Figure 2).
Table 2. - Comparison of patients with and without tissue disruption in the retrospective cohort Patients with tissue disruption (N = 32) Patients without tissue disruption (N = 148) P value Age, yr, mean ± SD 55.5 ± 15.1 58.8 ± 14.6 0.27 Female sex, % (n) 72 (23) 70 (103) 0.80 White race, % (n) 81 (26) 89 (131) 0.26 Hispanic ethnicity, % (n) 0 (0) 1 (2) 1.0 Dilator size, mean ± SD 59.8 ± 0.7 56.4 ± 5 <0.001b Dilator 58 Fr or larger, % (n) 100 (32) 62 (92) <0.001b Perforation, % (n) 0 (0) 0.5 (1) 1.0 Esophageal hypermotility disordersa (n = 38), % (n) 44 (4/9) 14 (4/29) 0.049 Hiatal hernia, % (n) 13 (4) 16 (23) 0.79 Barrett's esophagus, % (n) 6 (2) 3 (5) 0.61 Esophagitis, % (n) 9 (3) 11 (16) 1.0 Having anxiety or depression, % (n) 54 (15) 62 (80) 0.41 Having chronic pain disorder, % (n) 71 (22) 81 (94) 0.61 Neuromodulator use, % (n) 54 (15) 52 (69) 0.87aEsophageal hypermotility disorders: achalasia, distal esophageal spasm, hypercontractile esophagus, and esophagogastric junction outflow obstruction.
bP < 0.001.
 Figure 2.:
Figure 2.: Tissue disruption at the proximal esophagus after empiric esophageal dilation.
Perforation occurred in 1 patient (0.5%), managed conservatively, see Supplementary SR1 (Supplementary Digital Content 1, https://links.lww.com/CTG/B113) for details.
HREM was available in 38 patients. A potentially dysphagia-associated hypermotility disorder was present in 21% (n = 8) of patients with manometry (Table 1). Furthermore, 44% (n = 4) of the 9 patients with tissue disruption who had undergone manometry had esophageal hypermotility disorders (achalasia n = 1, distal esophageal spasm n = 1, and esophagogastric junction outflow obstruction n = 2) compared with 14% (n = 4) of those without disruption, P = 0.049 (Table 2).
Prospective armA total of 52 patients undergoing EED for NOD were prospectively surveyed using the PROMIS GI disrupted swallowing scale. Some patients were lost to follow-up and did not answer further questionnaires, leaving 41 patients who answered the questionnaire at 1 month, 35 patients at 3 months, and 31 patients at 6 months.
There were 44% (23) patients with tissue disruption after EED (18 distal esophagus, 2 proximal, 1 in both, and other 2 unspecified). When comparing patients with and without tissue disruption after EED, baseline characteristics were similar. Patients with tissue disruption after EED had a lower proportion of comorbid anxiety and depression compared with those without disruption: 24% vs 55%, P = 0.015, respectively. HREM (n = 10) showed ineffective esophageal motility in 2 patients, whereas the rest had a normal manometry (Table 3).
Table 3. - Demographic and comorbidities in patients with tissue disruption and without tissue disruption after dilation in the prospective cohort Total patients (N = 52) Patients with tissue disruption after dilation (N = 23) Patients without tissue after dilation (N = 29) P value Female sex, % (n) 58 (30) 65 (15) 36 (8) 0.32 Age, yr, mean ± SD 54.9 ± 13.1 54.5 ± 12.8 55.2 ± 13.5 0.85 Average BMI ± SD 28.8 ± 7.9 27.1 ± 6.1 30 ± 8.9 0.19 Dilation type, % Maloney (N) 94 (49) 91 (21) 97 (28) 0.577 Dilation size, % 60 Fr (N) 96 (50) 100 (23) 93 (27) 0.34 Average baseline dysphagia score (raw) ± SD 60.1 ± 9.0031 59.2 ± 8.1 60.9 ± 9.8 0.505 Underwent HREM 21 (10) 15 (3) 25 (7) 0.49 Esophageal hypermotility diagnoses 0 (0) 0 (0) 0 (0) Not available Anxiety or depression, % positive (N) 40 (21) 24 (5) 55 (16) 0.015a Pain syndrome, % positive (N) 27 (14) 17 (4) 35 (10) 0.17 Neuromodulation, % on at least one (N) 60 (31) 48 (11) 69 (20) 0.02aBMI, body mass index; HREM, high-resolution esophageal manometry.
aP < 0.05.
To account for missing data, we estimated the mean T-score from a repeated-measures mixed model with unstructured covariance among the repeated measures to determine adjusted means for a measure at each study time point. The primary outcome, the mean disrupted swallowing T-score, was 60.1 ± 9.1 at baseline, 56.1 ± 9.5 at 1 month (P = 0.03), 57 ± 9.6 at 3 months (P = 0.10), and 56 ± 10 at 6 months (P = 0.02) (Table 4). Minimal clinical important difference, defined as 0.5-SD improvement (or 5 T-score units), occurred in 46% (19) of patients at 1 month, 34% (12) at 3 months, and 36% (11) at 6 months.
Table 4. - Primary and secondary outcome data over time in the prospective cohort Total cohort Baseline (N = 52) 1 mo (N = 41) Estimated change 95% CI P value 3 mo (N = 35) Estimated change 95% CI P value 6 mo (N = 31) Estimated change 95% CI P value Total dysphagia score (T-score) 60.1 ± 9.1 56.1 ± 9.5 −2.13 −7.99 to −0.34 0.03a 57 ± 9.6 −1.58 −7.3 to 0.76 0.10 56 ± 10 −2.11 −8.63 to −0.31 0.02a Patients with tissue disruption Baseline (N = 23) 1 mo (N = 19) Estimated change 95% CI P value 3 mo (N = 18) Estimated change 95% CI P value 6 mo (N = 16) Estimated change 95% CI P value Total dysphagia score (T-score) 59.2 ± 8.1 53.0 ± 9.6 −2.2 −11.8 to −0.66 0.03a 55.1 ± 9.8 −1.40 −9.7 to 1.6 0.16 54.0 ± 10.5 −1.74 −11.1 to 0.65 0.08 Patients without tissue disruption Baseline (N = 29) 1 mo (N = 22) Estimated change 95% CI P value 3 mo (N = 17) Estimated change 95% CI P value 6 mo (N = 15) Estimated change 95% CI P value Total dysphagia score (T-score) 60.1 ± 10 58.6 ± 8.6 −0.75 −7.16 to 3.20 0.45 58.7 ± 9.2 −0.81 −7.81 to 3.22 0.42 57.5 ± 9.5 −1.22 −9.31 to 2.18 0.22Data shown are T-score transformation of the PROMIS GI disrupted swallowing. Higher scores signify worse dysphagia. Data are shown as estimated means (SE) from mixed-model repeated-measures analysis with unstructured covariance among the repeated measures to determine adjusted means for a measure at each study time point and whether there was a significant difference in measure over time from baseline to each time point.
CI, confidence interval; GI, gastrointestinal; PROMIS, Patient-Reported Outcomes Measurement Information System.
aP < 0.05.
When examining the change in the specific PROMIS dysphagia subcomponents using the same repeated-measures mixed-model analysis, we found the only significant improvement occurred in solid food dysphagia: with an estimated mean of 1.9 ± 1.1 at baseline, improving to 1.1 ± 1.0 (P < 0.01) at 1 month, 1.3 ± 1.1 (P < 0.01) at 3 months, and 1.2 ± 1.1 (P < 0.01) at 6 months (see Supplementary Table SR1, Supplementary Digital Content 1, https://links.lww.com/CTG/B113).
When comparing the patients with tissue disruption to those without, the change in total dysphagia T-score was significantly improved at 1 month (P = 0.03) but not at 3 months (P = 0.16) or 6 months (P = 0.08). However, in patients without tissue disruption, the means were similar in all time points (P > 0.05 for all comparisons) (Table 4 and Figure 3). There were no significant differences in minimal clinical important difference proportions at any time point between the tissue disruption and no tissue disruption groups. A clinically important difference was found in 10 (52.6%) in those with tissue disruption compared with 9 (47.4%) in those without at 1 month (P = 0.453); in 6 (33.3%) in those with tissue disruption compared with 6 (35.3%) in those without at 3 months (P = 0.903); and in 6 (37.5%) in those with tissue disruption compared with 5 (33.3%) in those without at 6 months (P = 0.809).
The solid food dysphagia subcomponent also significantly improved only in patients with tissue disruption but not in those without. Baseline, 1-month, 3-month, and 6-month raw scores were 2 ± 1.1, 0.8 ± 1.0 (P < 0.01), 1.2 ± 1.1 (P = 0.02), and 1.1 ± 1.1 (P < 0.01), respectively, in patients with tissue disruption. The scores were 1.7 ± 1.2, 1.4 ± 0.9 (P = 0.18), 1.3 ± 1.0 (0.14), and 1.3 ± 1.1 (P = 0.13), respectively, for patients without tissue disruption (see Supplementary Tables SR2 and SR3, Supplementary Digital Content 1, https://links.lww.com/CTG/B113).
No AEs occurred in the prospective cohort, without bleeding episodes that necessitated intervention or procedure-related deaths.
DISCUSSIONAlthough the practice of EED is widespread, evidence supporting its use remains conflicting. In this prospective assessment of efficacy and retrospective real-world review of EED safety, we found EED induces a clinically meaningful dysphagia improvement, especially solid food dysphagia, which may last for at least 6 months. It is also safe, with no bleeding or procedure-related deaths, and a 0.5% perforation rate.
We observed a significant improvement in 34%–46% of patients lasting at least 6 months after EED. This improvement was primarily driven by a significant change in solid food dysphagia scores. In addition, patients with tissue disruption after EED (but not those without) experienced prolonged improvements in dysphagia scores compared with their predilation baselines.
Although the presence of tissue disruption suggests relief of an esophageal narrowing that can be missed on endoscopy, the factors associated with initial success or durability of EED in NOD are poorly characterized. Comparing our findings with those of other studies is limited by variations in study design, patient selection criteria, dilation protocols, and the use of various dysphagia assessment scales at different time points. Nevertheless, most studies tend to support the benefits of large-caliber bougie dilation for the treatment of NOD, which aligns with our findings.
Jacob et al show that when a mucosal tear occurs after an EED, dysphagia improvement occurs at a similar rate to dilation of visible strictures, at least during the 2-week follow-up period reported in their study (13). Our study shows the difference in dysphagia improvement persists for a month and perhaps longer.
Marshall et al used empiric bougie dilation for NOD (n = 37) and found a 95% complete resolution in patients with solid food dysphagia, compared with a 47% partial response in patients with mixed liquid and food dysphagia (14). Similarly, Colon et al showed patients were able to eat a larger variety of solid foods after a dilation with a 50-fr, but not 26-Fr bougie (n = 22) (15).
By contrast, a retrospective study of 107 patients showed similar efficacy in patients treated with gastroesophageal reflux disease medications whether they had undergone empiric dilation or not, although selection bias in their study design is a serious limitation (16). A prospective study of 83 patients with widely patent Schatzki rings examining the efficacy of through-the-scope balloon dilation showed no difference whether the balloon was inflated or not at the gastroesophageal junction (17). Our finding that 47% of patients had tissue disruption in the proximal esophagus may explain their negative findings because their protocol excludes the proximal esophagus. We prefer using a bougie dilator for EED to address the entire esophagus because multiple through-the-scope dilations would be more cumbersome and prolong procedural time (18).
Our study confirms the safety of empiric dilation with no bleeding or procedural deaths and a perforation rate of 0.5%. In a study of intraprocedural complications recorded during endoscopy, a perforation rate of 0.03% and a bleeding rate of 0.04% were documented (19). When reviewing studies with extended follow-up periods, no instances of perforation or bleeding were reported in 242 patients in several smaller-scale studies of EED in NOD dilation (6,14,16,19–22).
To the best of our knowledge, this is the first substantive study applying the PROMIS dysphagia questionnaire in the setting of EED for NOD. Our study suggests that systematic assessment with validated patient-reported outcomes can guide NOD management. Our results suggest that with careful patient selection, EED is effective and safe in the management of NOD. We also offer our approach to manage patients with NOD (Figure 4).
 Figure 3.:
Figure 3.: T-score change after empiric esophageal dilation stratified according to the presence of tissue disruption. Data shown are T-score transformation of the PROMIS GI disrupted swallowing. Higher scores signify worse dysphagia. Data are shown as estimated means (SE) from mixed-model repeated-measures analysis with unstructured covariance among the repeated measures to determine adjusted means for a measure at each study time point and whether there was a significant difference in measure over time from baseline to each time point. The mixed model accounted for missing data when participants withdraw. *P < 0.05. GI, gastrointestinal; PROMIS, Patient-Reported Outcomes Measurement Information System.
 Figure 4.:
Figure 4.: Algorithm for EED in NOD. DES, diffuse esophageal spasm; EED, empiric esophageal dilation; EGJOO, esophagogastric junction outflow obstruction; NOD, nonobstructive dysphagia; PRO, patient-reported outcome.
The finding of tissue disruption, suggesting relief of a luminal narrowing with EED, does not obviate the need for motility testing. However, whether the identified motility disorders have effective treatment options is debatable. A similar requirement for HREM, despite an alternate dysphagia explanation, is also supported by recent research, suggesting an association between eosinophilic esophagitis and achalasia (15).
Finally, our work shows that clinical factors associated with disordered gut-brain interaction (DGBI) must remain within the list of differential diagnoses of endoscopists managing NOD. Functional dysphagia with esophageal hypersensitivity is believed to be characterized by pain/discomfort, which likely falls within the reflux hypersensitivity DGBI umbrella (23). Although anxiety and depression do not cause DGBIs, they are frequent comorbidities (24). That patients with tissue disruption had lower rates of comorbid anxiety or depression suggests a DGBI component in patients with dysphagia but no tissue disruption. Because knowledge of tissue disruption is only available after the decision for empiric dilation has been made, anxiety and depression disorders may alert physicians to a subgroup that is less likely to benefit from EED.
Our study is not without limitations. A lack of a control group may overestimate the effect of empiric dilation without a placebo comparator. Our finding that efficacy is associated with objective findings, such as tissue disruption, may partially address that concern. Despite being one of the largest prospective published studies on empiric bougie dilation, our prospective arm recruitment was limited by the COVID-19 pandemic. Our retrospective cohort does not offer efficacy data beyond recording of tissue disruption. Because examining efficacy is much more difficult retrospectively, even with rigorous chart review, we did not examine efficacy of EED in the retrospective cohort. Safety, however, is well reflected in the retrospective study arm, and our cohort is the largest to date to show 30-day AE rates. We recognize that low HREM utilization may overestimate motility disorder prevalence because of selection bias. This circumstance also constrains the possibility of tailoring patient management based on motility disorder diagnosis. However, the low utilization of manometry serves as a noteworthy finding in itself, emphasizing the importance of HREM testing.
In conclusion, our study suggests that empiric dilation in patients with NOD is both efficacious and safe. When tissue disruption occurs after dilation, a significant improvement in dysphagia lasting up to 6 months can be expected (particularly for the complaint of solid food dysphagia). The finding of tissue disruption does not preclude HREM because motility disorders may still coexist. We found patients with comorbid anxiety and depression are less likely to have tissue disruption, which may help inform decision-making when considering the need for empiric dilation.
CONFLICTS OF INTERESTGuarantor of the article: Christopher Vélez, MD.
Specific author contributions: C.V., B.K., and K.S.: study conception and design. A.P.B., F.R., J.N., N.B., and M.P.: data collection. N.B., M.P., K.S., C.V., and B.K.: analysis and interpretation of results. N.B., M.P., C.V., K.S., and B.K.: draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
Financial support: All authors disclose no conflicts of interest related to this study. K.S. is supported by NIH K23DK120945. C.V. received funding research grants from the Cystic Fibrosis Foundation, Ironwood and the American College of Gastroenterology.
Potential competing interests: None to report.
Study Highlights
WHAT IS KNOWN ✓ Dysphagia is common and sometimes managed with empiric esophageal dilation in nonobstructive dysphagia. ✓ The efficacy and safety of empiric esophageal dilation are debatable. WHAT IS NEW HERE ✓ Empiric esophageal dilation is safe, with low perforation rates. ✓ Empiric esophageal dilation is effective for at least 6 months when tissue disruption occurs. ✓ Esophageal manometry is underused in the assessment of dysphagia cases meriting endoscopy assessment. REFERENCES 1. Leslie P, Smithard DG. Is dysphagia under diagnosed or is normal swallowing more variable than we think? Reported swallowing problems in people aged 18–65 years. Dysphagia 2021;36(5):910–8. 2. Varadarajulu S, Eloubeidi MA, Patel RS, et al. The yield and the predictors of esophageal pathology when upper endoscopy is used for the initial evaluation of dysphagia. Gastrointest Endosc 2005;61(7):804–8. 3. Chaptini L, Chaaya A, Depalma F, et al. Variation in polyp size estimation among endoscopists and impact on surveillance intervals. Gastrointest Endosc 2014;80(4):652–9. 4. Bill J, Rajagopal S, Kushnir V, et al. Diagnostic yield in the evaluation of dysphagia: Experience at a single tertiary care center. Dis Esophagus 2018;31(6):doy013. 5. Kamal F, Khan MA, Lee-Smith W, et al. Efficacy of empiric esophageal dilation in patients with non-obstructive dysphagia: Systematic review and meta-analysis. Scand J Gastroenterol 2021;56(12):1490–5. 6. Al Saleh HA, Malikowski T, Patel DA, et al. Empirical dilation of non-obstructive dysphagia: Current understanding and future directions. Dig Dis Sci 2022;67(12):5416–24. 7. Richter JE. Esophageal dilation in eosinophilic esophagitis. Best Pract Res Clin Gastroenterol 2015;29(5):815–28. 8. Nalichowski R, Keogh D, Chueh HC, et al. Calculating the benefits of a Research Patient Data Repository. AMIA Annu Symp Proc 2006;1044. 9. ASGE Standards of Practice Committee, Pasha SF, Acosta RD, et al. The role of endoscopy in the evaluation and management of dy
留言 (0)