
記住我


Hepatic encephalopathy (HE) is a group of neuropsychiatric symptoms caused by hepatic insufficiency and/or portal-systemic shunting (1,2). Despite advances in understanding the complex pathogenesis of HE, the precise mechanism underlying the disease remains unknown. Hyperammonemia has been identified as a significant contributor to brain dysfunction in HE, particularly in acute liver failure (3–5). However, several clinical studies have failed to find a direct correlation between the degree of hyperammonemia and HE severity (6–8). In addition, previous studies found that the systemic inflammatory response score, serum tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and IL-18 levels were higher in cirrhotic patients with HE compared with those without, indicating a relationship between systemic inflammation and HE (8–10).
Bacterial translocation (BT) is the migration of bacteria and/or bacterial products from the intestine to mesenteric lymph nodes and other extraintestinal sites (11). BT is more prevalent in patients with advanced chronic liver disease, with a prevalence rate of 3.4%, 8.1%, and 30.8% in those with Child-Turcotte-Pugh (CTP) classes A, B, and C, respectively (12). Several mechanisms may contribute to the increased BT in patients with cirrhosis, including small intestinal bacterial overgrowth, increased intestinal permeability, and immunological impairment, such as reduction of hepatic macrophage function and decreased serum and ascitic fluid complement levels (13,14). BT induces systemic inflammation, increases portal pressure, and worsens hemodynamics in patients with cirrhosis (15,16). Furthermore, BT-related systemic inflammation is associated with a high mortality rate (17) and cirrhotic complications such as ascites and variceal bleeding (18,19).
Bacterial DNA (bactDNA), serum lipopolysaccharide-binding protein (LBP), soluble CD14 (sCD14), and endotoxin have all been studied as potential biomarkers for BT. BactDNA testing allows for broad-range detection and rapid identification of bacteria, primarily by detecting the 16S ribosomal ribonucleic acid genes that are universally present in all bacteria. BactDNA translocation is associated with systemic circulatory abnormalities and intrahepatic endothelial dysfunction in patients with cirrhosis (20). Furthermore, a previous study found that the presence of bactDNA in serum and ascitic fluid was related to the development of acute-on-chronic liver failure (ACLF) and a high 1-year mortality rate (21). A previous observational study showed that bactDNA translocation was associated with worse neurocognitive scores in cirrhotic patients with minimal HE (22). There is limited evidence of a link between bactDNA translocation, serum inflammatory markers, ammonia, and the presence of HE. Therefore, this study aimed to investigate the association between bactDNA translocation, serum inflammatory markers, ammonia levels, and severity of HE in patients with cirrhosis, as well as the association of these biomarkers and 6-month mortality.
METHODS Study participantsPatients with liver cirrhosis aged 18–80 years were consecutively prospectively enrolled from the Liver Clinic and inpatient wards at Chulalongkorn University Hospital in Bangkok, Thailand, from June 2022 to January 2023. Cirrhosis was diagnosed based on clinical or laboratory data and confirmed by radiological imaging. Exclusion criteria were history of any bacterial infection, antibiotic, lactulose, psychotropic or recreational drugs use, active neurological or psychiatric diseases (i.e. acute stroke, dementia, and psychosis) in the previous 2 weeks, clinical suspicion of bacterial infection 2 weeks after enrollment, previous transjugular intrahepatic portosystemic shunt or shunt surgery, recent alcohol misuse in the past 3 months, and inability to read and write. Clinical suspicion of bacterial infections was diagnosed using systemic inflammatory response syndrome criteria, which included any 2 of the following: body temperature > 38 or < 36 ° C, heart rate > 90 beats/minutes, respiratory rate > 20 breaths/minute, or leukocyte count greater than 12,000 or less than 4,000/mL. Alcohol misuse was diagnosed based on the National Institute on Alcohol Abuse and Alcoholism definitions (https://www.niaaa.nih.gov). Decompensated cirrhosis was diagnosed if the patient had at least one decompensating event, including overt HE, ascites, or variceal bleeding.
All patients underwent physical and neurological examination and laboratory testing. Serum and ethylenediaminetetraacetic acid plasma were obtained using standard sterile procedures and stored at −80 °C until analysis. The patients were then followed for 6 months, with death recorded. The required number of patients for the study was determined to be 63 patients without HE and 63 for those with HE, based on a calculation using the formula provided in Supplementary Digital Content (see Supplementary Figure 1, https://links.lww.com/CTG/B99).
The study protocol and patient consent form were approved by the Institutional Review Board, Faculty of Medicine, Chulalongkorn University (IRB no. 0171/65). All participants or their legitimate representatives provided written informed consent to participate in the study. The study protocol adhered to the Helsinki Declaration's ethical principles and the Good Clinical Practice recommendations. The study protocol was registered at the Thai Clinical Trial Registry (TCTR20220528002, May 18, 2022).
Evaluation of hepatic encephalopathyHE was diagnosed and graded using the West Haven Criteria. Patients without overt HE were assessed using the Thai version of the Psychometric Hepatic Encephalopathy Score (PHES) battery, which had previously been standardized and validated in our previous study (23). PHES comprises 5 paper-pencil tests: number connection-A, number connection-B, digit symbol test, serial dotting test, and line tracing test. The final PHES was calculated by adding the scores from 5 subtests ranging from +5 to −15. Minimal HE was diagnosed when the sum of 5 subtests scores ≤ −5 points (23). Covert HE was diagnosed as minimal HE or grade I HE by West Haven Criteria.
Quantification of plasma bactDNABactDNA was extracted from 400 μL of plasma under complete aseptic conditions using the MagDEA Dx reagents and the automated sample preparation system (Precision System Science, Chiba, Japan). A real-time polymerase chain reaction (PCR) for the broad-range detection of the bacterial 16S ribosomal ribonucleic acid gene was adapted from a previous study (24). Briefly, primers directed against the V7–V9 variable region of the 16S gene (forward: RW01; 5'-AACTGGAGGAAGGTGGGGAT-3'; reverse: DG74.R; 5'-AGGAGGTGATCCAACCGCA-3') were mixed with a custom fluorescent probe (5'-6-FAM-TACAAGGCCCGGGAACGTATTCACCG-BHQ-3'; Integrated DNA Technologies, Singapore) at final concentrations of 0.3 mM and 0.05 mM, respectively. This was mixed with 5 μL of the 2X Maxima Probe no ROX qPCR Master Mix (Thermo Fisher Scientific Baltics, UAB, Lithuania), 1 μL of Uracil-DNA Glycosylase (Thermo Fisher Scientific Baltics), 1 μL of 10X buffer Uracil-DNA Glycosylase (Thermo Fisher Scientific Baltics), 1.3 μL of PCR-grade water, and 1 μL of the DNA template to give a final reaction volume of 10 μL. A 50-cycle PCR was run in a Light Cycler 480 System (Roche Diagnostics, Switzerland) using the following cycling conditions: one cycle at 50 °C for 2 minutes and 95 °C for 10 minutes; 50 cycles at 95 °C for 15 seconds and 60 °C for 1 minute.
A serial 10-fold dilution of microbial DNA (3–3,000,000 pg/μL) from Escherichia coli (MBD0013; Sigma-Aldrich, Pte Ltd, Singapore) and negative control were used to generate a standard curve. The standards and samples were tested in duplicate, and the mean was calculated. Standard curves were generated, and the bactDNA concentrations were determined using the Prism software, Version 9.0 (GraphPad, La Jolla, CA). The bactDNA levels were expressed as pg/µL of collected whole blood. BT was diagnosed if bactDNA levels were above 3 pg/μL.
Measurement of venous ammonia, cytokines, and endotoxin markersTo measure ammonia levels, venous blood samples were collected into ethylenediaminetetraacetic acid tubes, immediately placed on ice, and transferred to the laboratory, where they were processed and tested within 30 minutes. Venous ammonia levels were measured on the ARCHITECT c8000 system using the enzymatic glutamate dehydrogenase assay kits (Abbott Laboratories, Germany) according to the manufacturer's protocol.
BT markers and studied cytokines, including LBP and sCD14, IL-6, and TNF-α, were determined in stored plasma samples using the Human SimpleStep enzyme-linked immunosorbent assay kits (Abcam, UK; ab279407, ab208983, ab178013, and ab181421, respectively) according to the manufacturer's instructions.
Statistical analysisCategorical variables were expressed as numbers and percentages and compared groups using the Pearson χ2 or Fisher exact test. Continuous variables were analyzed for normality using the Shapiro-Wilk test. Normally distributed data were expressed as mean (SD) and compared groups using the independent t test, whereas non-normally distributed data were expressed as median (interquartile range) and compared groups using the Mann-Whitney U test. The Spearman correlation coefficient was used to correlate the PHES score, plasma bactDNA level, inflammatory cytokines, and venous ammonia levels in patients without overt HE. Logistic regression analysis was used to identify factors associated with the presence of HE. Univariate and multivariate Cox regression analyses were used to identify potential factors related to 6-month mortality. Survival analysis was performed using Kaplan-Meier curves, and the Wilcoxon test was used to compare survival rates. Statistical analysis was performed using the SPSS software, Version 22 (IBM, Armonk, NY), and 2-sided P values less than 0.05 were considered statistically significant.
The study protocol and patient consent form were approved by the Institutional Review Board, Faculty of Medicine, Chulalongkorn University (IRB no. 0171/65).
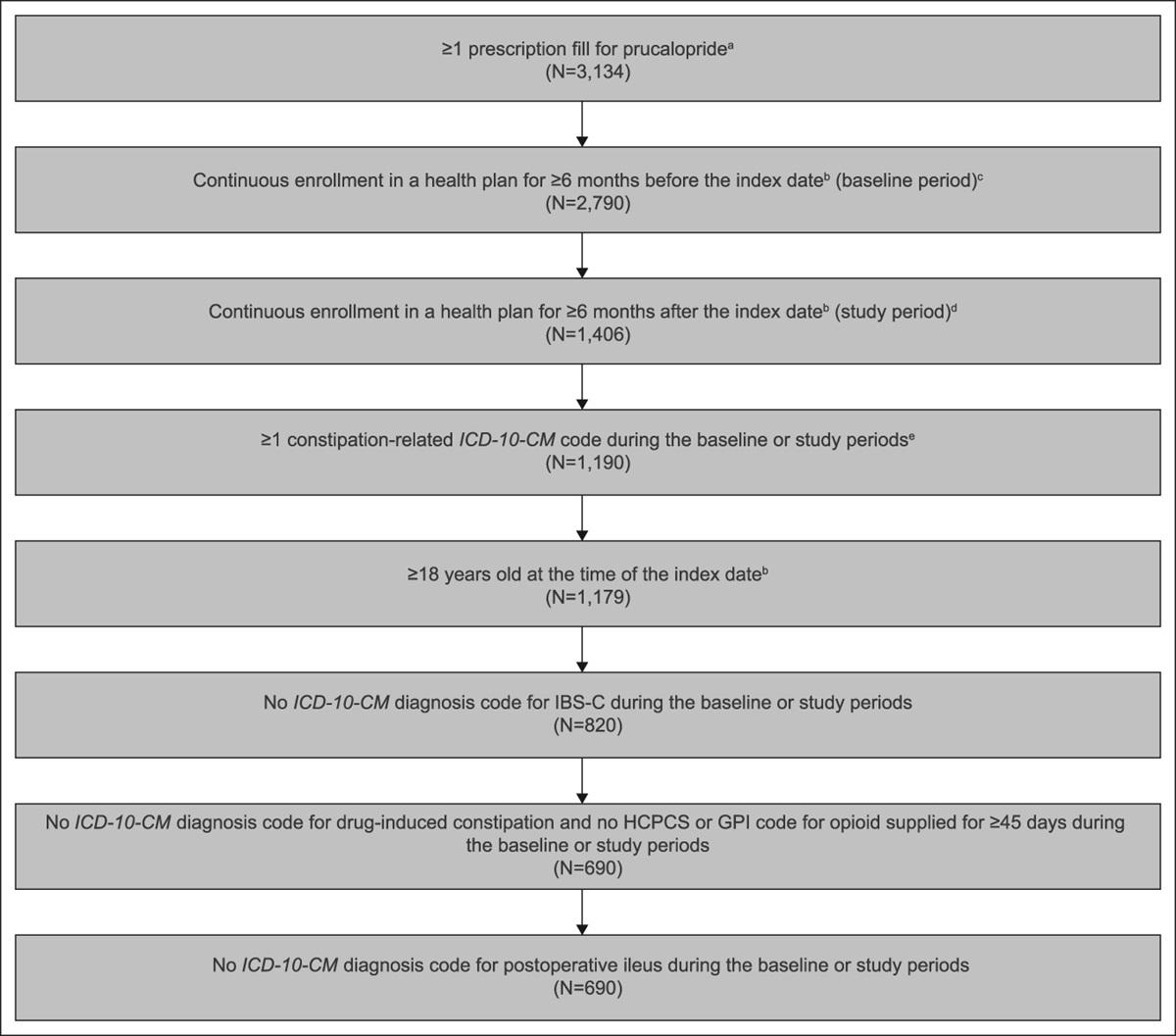
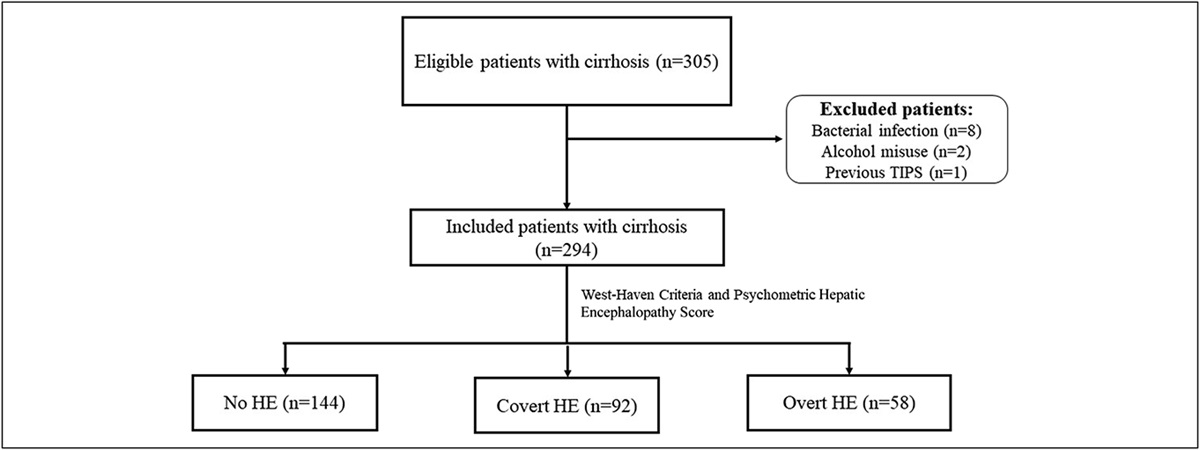
RESULTS Patient characteristicsIn this study, 294 of the 305 patients with liver cirrhosis were consecutively enrolled, whereas 11 were excluded because of one or more exclusion criteria. The flowchart of patient enrollment is shown in Figure 1. The patients had a mean age of 58.8 ± 13.6 years, with 58.8% male (n = 173). The most common etiology of cirrhosis was chronic hepatitis B virus (n = 87, 29.6%), followed by alcohol-related liver disease (n = 79, 26.9%). The median CTP and Model for End-Stage Liver Disease (MELD) scores were 6 [Interquartile range (IQR: 5-9)] and 11 (IQR 8–17), respectively. In total, 92 patients (31.3%) were diagnosed with covert HE (HE grade 1 [n = 70] and minimal HE [n = 22]), whereas 58 (19.7%) had overt HE (HE grade 2 [n = 42], HE grade 3 [n = 13], and HE grade 4 [n = 3]). The baseline characteristics and laboratory findings stratified by HE severity are summarized in Table 1. Patients with overt HE had significantly higher CTP and MELD scores than those with covert HE or no HE.
 Figure 1.:
Figure 1.: Flow chart of patient enrollment. HE, hepatic encephalopathy.
Table 1. - Baseline patient characteristics classified according to the severity of hepatic encephalopathy No HE (n = 144) Covert HE (n = 92) Overt HE (n = 58) P value Age, yr 59 (48–65) 62 (55–69) 62 (52–73) 0.004 Male, n (%) 80 (55.6%) 56 (60.9%) 37 (63.8%) 0.50 Etiology of cirrhosis, n (%) HBV, n (%) 43 (29.9%) 27 (29.3%) 17 (29.3%) 0.99 ARLD, n (%) 31 (21.5%) 28 (30.4%) 20 (34.5%) 0.11 Ascites, n (%) 22 (15.3%) 25 (27.2%) 38 (65.5%) <0.001 Child-Pugh class <0.001 A 111 (77.1%) 51 (55.4%) 2 (3.4%) B 26 (18.1%) 26 (28.3%) 16 (27.6%) C 7 (4.9%) 15 (16.3%) 40 (69.0%) Child-Pugh score 5 (5–6) 6 (5–8.8)a 10 (9–12)a,b <0.001 MELD 9 (8–13) 11 (8–16)c 20.5 (14.3–27)a,b <0.001 Hb, g/dL 12.2 ± 2.3 11.3 ± 2.7 9.5 ± 3.0 <0.001 WBC, cells/µL 5,715 (4,210–7,840) 5,220 (4,190–7,180) 8,330 (4,880–11,610)a,b <0.001 Neu/lym ratio 2.1 (1.5–3.4) 2.4 (1.6–4.1) 6.2 (2.9–10.2)a,b <0.001 Platelet, ×109/L 171 (101–238) 115 (80–171) 102.5 (73.8–171.8) <0.001 TB, mg/dL 1.0 (0.7–1.6) 1.5 (0.8–2.8) 4.8 (2.1–13.8) <0.001 AST, U/L 35 (24–51) 42 (28–60) 68 (40–130) <0.001 ALT, U/L 28 (19–42) 27 (20–43) 33 (22–59) 0.20 Albumin, g/dL 3.9 (3.3–4.2) 3.3 (2.9–3.8) 2.7 (2.2–3.0) <0.001 INR 1.2 (1.1–1.4) 1.2 (1.1–1.4) 1.5 (1.3–2.1) <0.001 Creatinine, mg/dL 0.9 (0.7–1.0) 0.9 (0.7–1.2) 0.9 (0.7–1.5) 0.06 Sodium, mEq/L 138 (136–140) 137.5 (135–140) 134 (130–138) <0.001Categorical variables were expressed as number and frequency, whereas continuous variables were expressed as mean ± SD or median (IQR), as appropriate.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; ARLD, alcohol-related liver disease; Hb, hemoglobin; HBV, hepatitis B virus; HE, hepatic encephalopathy; Neu/lym ratio, neutrophil-to-lymphocyte ratio; TB, total bilirubin; VB, variceal bleeding; WBC, white blood cell count.
aP < 0.001 compared with no HE.
bP < 0.001 compared with overt HE and covert HE.
cP < 0.05 compared with no HE.
BactDNA translocation was detected in 36.1% of all patients (n = 106) and 31.3% (n = 45), 35.9% (n = 33), and 48.3% (n = 28) of cirrhotic patients with CTP classes A, B, and C, respectively. Patients with decompensated cirrhosis tended to have higher bactDNA levels than those with compensated cirrhosis (423.2 ± 4,546.2 vs 225.2 ± 1,201.2 pg/μL, P = 0.10), but the difference was not statistically significant. Furthermore, bactDNA was found in 31.3% (n = 45), 35.9% (n = 33), and 48.3% (n = 28) in patients with no HE, covert HE and overt HE, respectively. BactDNA translocation was significantly higher in patients with overt HE than those without HE (P = 0.02). In addition, bactDNA levels (381.7 ± 1,572.2 vs 76.9 ± 522.9 pg/μL, P < 0.001) and serum LBP (11,165 [IQR: 8,144–15,023] vs 8,615 [IQR: 6,762–12,802] ng/mL, P = 0.01) were significantly higher in patients with overt HE than in those without HE, indicating that BT was greater in patients with overt HE. Furthermore, patients with overt HE exhibited higher serum TNF-α (P = 0.04) and IL-6 levels (P < 0.001) than those without HE, implying a higher proinflammatory state. Ammonia levels were significantly higher in patients with overt HE [84.5 (IQR: 63–120) μg/dL] than those without HE (57 [IQR: 45–73] μg/dL, P < 0.001]). By contrast, patients with covert HE tended to have higher bactDNA, serum LBP, and sCD14 levels than those without HE, although the differences were not statistically significant. Serum TNF-α and IL-6 levels were significantly higher in patients with covert HE than those without HE. Figure 2 demonstrates the studied biomarker levels according to the severity of HE.
 Figure 2.:
Figure 2.: Bacterial translocation, inflammatory markers, and ammonia levels stratified by severity of HE. HE, hepatic encephalopathy. *p<0.05, ** p<0.001.
Logistic regression analysis of factors associated with the presence of overt HE at baseline was shown in Supplementary Digital Content (see Supplementary Table 1, https://links.lww.com/CTG/B100). Univariate analysis showed that the CTP score, presence of bactDNA, IL-6, and ammonia were associated with the presence of overt HE. In multivariate analysis, including these factors, only the CTP score (adjusted odds ratio = 1.98, 95% confidence interval [95% CI]: 1.66–2.37, P < 0.001) was found to be an independent predictor of the presence of overt HE (model 1). However, bactDNA (adjusted odds ratio = 2.20, 95% CI: 1.00–4.82, P = 0.04) was an independent factor associated with overt HE when adjusting for the CTP score (model 2).
Patients with bactDNA translocation had significantly higher white blood cell count, neutrophil-to-lymphocyte ratio, serum IL-6, and LBP levels than those without, with no significant differences in CTP and MELD scores, as well as TNF-α, sCD14, and ammonia levels (Table 2).
Table 2. - Baseline characteristics and inflammatory mediators in patients with and without bacterial DNA translocation Absence of bactDNA translocation (n = 188) Presence of bactDNA translocation (n = 106) P value Age, yr 60 (50–66) 60 (50–68) 0.07 Male, n (%) 115 (61.2%) 58 (54.7%) 0.28 Hb, g/dL 11.4 ± 2.9 11.3 ± 2.7 0.31 WBC 5,645 (4,192–7,913) 6,410 (4,770–8,620) 0.04 Neu/lym ratio 2.8 (1.7–4.4) 2.2 (1.3–4.5) 0.33 Platelet 134 (81.5–194) 129 (81–218) 0.55 TB, mg/dL 1.3 (0.8–2.8) 1.5 (0.8–3.7) 0.82 AST, U/L 37 (26–60) 44 (28.5–71.5) 0.34 ALT, U/L 27 (18–41) 30 (23–52.5) 0.67 Albumin, g/dL 3.4 (2.8–4) 3.5 (2.7–4.1) 0.14 INR 1.3 (1.1–1.4) 1.3 (1.1–1.7) 0.55 Creatinine, mg/dL 0.9 (0.7–1.1) 0.8 (0.7–1.1) 0.82 Sodium, mEq/L 138 (135–140) 137 (134–140) 0.06 Child-Pugh score 6 (5–9) 6 (5–10) 0.08 MELD 11 (8–16) 12 (8–19) 0.94 TNF-α, pg/mL 6.7 (3.9–11.0) 6.5 (3.9–9.7) 0.82 IL-6, pg/mL 1.8 (0–16.1) 5.9 (0–31.1) 0.009 sCD14, ng/mL 2,510 (1,828–3,445) 2,527 (1,953–3,608) 0.63 LBP, ng/mL 8,811 (6,707–12,617) 11,163 (7,164–16,011) 0.003 Ammonia, μg/dL 62 (49–89) 62 (46.5–90) 0.92Categorical variables were expressed as number and frequency, whereas continuous variables were expressed as mean ± SD or median (IQR), as appropriate.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; BactDNA, bacterial deoxyribonucleic acid; Hb, hemoglobin; IL-6, interleukin-6; LBP, lipopolysaccharide-binding protein; Neu/lym ratio, neutrophil-to-lymphocyte ratio; sCD14, soluble CD14; TB, total bilirubin; TNF-α, tumor necrosis factor-alpha; WBC, white blood cell count.
In 236 cirrhotic patients without overt HE, the correlation between PHES and liver function, the severity of cirrhosis, inflammatory markers, BT markers, and ammonia levels were investigated (see Supplementary Table 2, https://links.lww.com/CTG/B100). PHES had a significantly negative correlation with total bilirubin (r = −0.24, P = 0.003), the International Normalized Ratio (INR) (r = −0.24, P = 0.004), CTP score (r = −0.26, P = 0.001), MELD score (r = −0.30, P < 0.001), and serum sCD14 levels (r = −0.19, P = 0.02), but a significantly positive correlation with serum albumin. However, it did not have any significant correlations with white blood cell counts and serum transaminase, bactDNA, TNF-α, IL-6, LBP, and ammonia levels.
Predictive value of bactDNA, cytokines, and ammonia for 6-month mortalityDuring a 6-month follow-up period, 40 patients (13.6%) died, and 4 patients (1.36%) received liver transplantation. The common cause of death was bacterial infection (n = 30, 75%), followed by ACLF development (n = 6, 15%) and variceal bleeding (n = 4, 10%). Cirrhotic patients who died within 6 months had more bactDNA translocation (57.5% vs 32.7%, P = 0.002) and higher levels of serum IL-6, TNF-α, LBP, and ammonia than those who survived (see Supplementary Table 3, https://links.lww.com/CTG/B100).
A Cox regression analysis was conducted to assess the role of BT, inflammatory markers, and ammonia in predicting 6-month mortality. The multivariate analysis revealed that bactDNA translocation (adjusted hazard ratio [aHR]: 2.49, 95% CI: 1.22–5.11, P = 0.01), MELD score (aHR: 1.12, 95% CI: 1.09–1.16, P < 0.001), age (aHR: 1.05, 95% CI: 1.02–1.08, P < 0.001), and serum IL-6 (aHR: 1.001, 95% CI: 1.000–1.002, P = 0.02) were all independent baseline factors associated with the 6-month mortality in patients with cirrhosis (Table 3). Figure 3 depicts the Kaplan-Meier survival analysis at 6 months based on bactDNA detection. Patients with no detectable bactDNA had a higher 6-month survival rate than those with detectable bactDNA (91% vs 78.3.3%, P = 0.01).
Table 3. - Factors independently associated with 6-month mortality in cirrhotic patients Univariate Cox regression analysis Multivariate Cox regression analysis HR (95% CI) P value HR (95% CI) P value Age, yr 1.02 (0.99–1.05) 0.06 1.05 (1.02–1.08) <0.001 MELD 1.09 (1.07–1.12) <0.001 1.12 (1.09–1.16) <0.001 BactDNA-positive 2.62 (1.40–4.90) 0.003 2.49 (1.22–5.11) 0.01 TNF-α, pg/mL 1.02 (1.002–1.03) 0.03 IL-6, pg/mL 1.001 (1.00–1.002) 0.002 1.001 (1.00–1.002) 0.02 sCD14, ng/mL 1.00 (1.00–1.00) 0.27 LBP, ng/mL 1.00 (1.00–1.00) 0.05 Ammonia, μg/dL 1.01 (1.005–1.02) <0.001BactDNA, bacterial deoxyribonucleic acid; CI, confidence interval; IL-6, interleukin-6; LBP, lipopolysaccharide-binding protein; MELD, Model for End-Stage Liver Disease; sCD14, soluble CD14; TNF-α, tumor necrosis factor-alpha.
 Figure 3.:
Figure 3.: Six-month survival according to bacterial DNA in patients with cirrhosis. BactDNA, bacterial DNA.
Association of bactDNA, cytokines, ammonia, and ascitesAt enrollment, 85 (28.9%) patients had ascites. Neutrophil-to-lymphocyte ratio, serum LBP, sCD14, LBP, and ammonia levels were significantly higher in patients with ascites than those without ascites. Although bactDNA levels tended to be higher in patients with ascites, there was no statistically significant difference (see Supplementary Table 4, https://links.lww.com/CTG/B100). These indicate prominent characteristics of BT and systemic inflammatory state in patients with ascites.
DISCUSSIONThe current study investigated the association between bactDNA translocation, serum LBP, IL-6, TNF-α, sCD14, ammonia levels, and HE severity. Furthermore, we assessed the potential value of these biomarkers in predicting mortality in patients with cirrhosis. Our main findings revealed that bactDNA translocation was more prevalent in advanced liver disease, with prevalence rates of 31.3%, 35.9%, and 48.3% in cirrhotic patients with CTP classes A, B, and C, respectively. In addition, patients with overt HE had more bactDNA translocation and higher serum LBP, TNF-α, IL-6, and ammonia levels than those without HE, indicating a relationship between BT, systemic inflammatory state, and overt HE. Moreover, bactDNA translocation, MELD score, age, and serum IL-6 were independent factors associated with 6-month mortality in patients with cirrhosis. Furthermore, patients without overt HE, bactDNA, TNF-α, IL-6, and ammonia levels did not correlate with PHES.
BT and subsequent systemic inflammation are well-known causes of acute decompensation and ACLF in patients with cirrhosis (25). A recent single-center case-control study identified antiendotoxin immunoglobulin M antibody and transforming growth factor-beta as predictors of variceal hemorrhage (19). BactDNA was detected in patients with spontaneous bacterial peritonitis (SBP) more frequently than those with noninfected ascites (100% vs 34%). BactDNA translocation and cytokine responses were suppressed with norfloxacin treatment in patients with SBP (18). In terms of HE, systemic inflammation increases blood-brain barrier permeability and neuroinflammation of the central nervous system (26,27). In addition, systemic inflammation modulates the cerebral effect of ammonia in cirrhosis (28). Previous studies on the influence of BT on HE yielded inconclusive results. An Indian cohort study by Jain et al revealed that serum endotoxin, inflammatory mediator, and arterial ammonia levels correlated with HE severity, increased as the HE stage progressed, and were higher in patients with minimal HE than those without HE (10). By contrast, another Danish study found that serum endotoxin, LBP, inflammatory cytokine, and arterial ammonia levels did not differ between patients with and without minimal HE (29). The current study found that cirrhotic patients with overt HE had significantly higher bactDNA levels, inflammatory mediators, and venous ammonia than those without HE. When adjusted by CTP score, bactDNA translocation was found to be an independent factor associated with the presence of overt HE. Although bactDNA translocation was associated with overt HE, bactDNA and serum LBP levels were comparable in patients with covert HE and those without HE. Furthermore, the PHES did not correlate with BT markers. We hypothesized that the amount of bactDNA translocation might be an essential component in developing overt HE. The discrepancies among studies could be explained by differences in the severity and etiology of cirrhosis, as well as the type of BT indicators used. The current study provides new insights into the pathogenesis of HE, particularly those related to BT, enabling novel advancements in treatment and care. However, further investigations may be required.
In terms of mortality, our study revealed that age, MELD score, bactDNA detection, and serum IL-6 were all independent predictors of 6-month mortality in cirrhotic patients. Liver transplantation was not included in the analysis because of a limited number of patients receiving transplantation (1.36%). It should be taken into account that the study did not assess bactDNA at different time points during the follow-up in the same patients. Future studies should evaluate the clinical significance of bactDNA monitoring during the course of cirrhosis. Published studies on the impact of bactDNA detection in blood or ascitic fluid on survival in cirrhotic patients without infection have yielded conflicting results because of differences in detection techniques. Engelmann et al showed that patients with detectable ascitic bactDNA had a lower 6-month survival rate than those without (42.6% vs 61.6%, P = 0.03) (30). Mani et al found that ascitic bactDNA detection was related to 30-day mortality in patients who recovered from SBP (31). In contrast, Zapater et al demonstrated that 1-year mortality was comparable in patients with noninfected ascites with and without detectable serum or ascitic bactDNA (21).
In recent years, ammonia and its implications for prognostic prediction in cirrhosis have received more attention. Previous large prospective cohort studies demonstrated that ammonia was an independent predictor of mortality (5,32), organ failure (5), and hospitalization in patients with cirrhosis (32). A recent study of clinically stable outpatients with advanced chronic liver disease found that venous ammonia independently predicted liver decompensation, ACLF, liver-related hospitalization, and death (33). However, the current study found that cirrhotic patients who died during a 6-month period had higher baseline venous ammonia levels than those who survived. Baseline ammonia level was not an independent factor of death. One possible explanation might be the selected variables for the multivariate Cox regression analysis. The current study included age, MELD score, inflammatory cytokines, and the presence of bactDNA for adjustment, in contrast to the previous studies that adjusted for CTP score, MELD score, patient baseline characteristics, and basic laboratory tests (5,32,33).
Our study has some limitations. First, there were a small number of patients with overt HE. However, to the best of our knowledge, this is the first study to assess bactDNA in patients with HE. Second, the variability of ammonia testing is high. Arterial ammonia may be preferable to venous ammonia (34,35). However, venous ammonia was used in this study because it is far more convenient for patients and physicians than arterial ammonia, making it more likely to be used in clinical practice. Furthermore, both venous and arterial ammonia were associated with HE severity (7). Third, clinical history and physical examination were used to exclude patients with active bacterial infection and other neuropsychological diseases. Regarding infection, we did not perform an infectious workup at enrollment. We would like to point out that signs and symptoms may be subtle and have limited sensitivity in diagnosing early bacterial infection. Therefore, it is possible that some patients with bacterial infection might have been overlooked and enrolled in the study. However, we excluded patients who developed clinical suspicion of bacterial infections within 2 weeks before and after enrollment. In addition, 30%–50% of cirrhotic patients with bacterial infection had negative cultures (36). Fourth, although the study excluded patients with systemic inflammatory responses, it is possible that some patients with subclinical tuberculosis, viral, or fungal infections might have been enrolled, which might have affected cytokine levels. Furthermore, the primer pairs used in the current study are unable to detect Mycobacterium tuberculosis, indicating that this organism does not affect bactDNA levels.
In conclusion, the study provided evidence supporting the theory of mechanistic pathogenesis of BT and the development of overt HE in patients with liver cirrhosis. In addition, bactDNA may be a potential marker for detecting HE and predicting 6-month mortality in cirrhotic patients.
CONFLICTS OF INTERESTGuarantor of the article: Piyawat Komolmit, MD, PhD.
Specific author contributions: K.T. and P.K. were involved in the conception and design of the study. K.T., S.S. (Sirinporn Suksawatamnuay), S.W., P.T., N.S., P.A., S.S. (Supachaya Sriphoosanaphan), J.V., S.T., Y.P. and P.K. were involved in data curation and formal analysis. K.T. and N.S. organized the assessments of the psychometric HE test. S.S. (Sirinporn Suksawatamnuay) performed real-time PCR and ELISA assays. K.T. and P.K. were involved in writing the original draft. All authors had access to the study data, reviewed, and approved the final version of this manuscript.
Financial support: The study was supported by the Ratchadapiseksompotch Endowment Fund of the Center of Excellence in Hepatic Fibrosis and Cirrhosis research unit (GCE 3300170037), the Ratchadapiseksompotch Endowment Fund (RA 65/021 and RA(DO) 005/67), Faculty of Medicine, Chulalongkorn University, the 90th and 100th Anniversary of Chulalongkorn University Scholarship under the Ratchadapisek Somphot Endowment Fund, the Thailand Science Research and Innovation Fund, Chulalongkorn University (HEA663000044), the Thai Red Cross Research Committee (2022), the Medical Council of Thailand, the Royal College of Physicians of Thailand (Polic General Dr. Jongjate Aojanepong Foundation), and the Thai Association for the Study of Liver.
Potential competing interests: None to report.
Clinical trial number: This trial was registered at the Thai Clinical Trial Registry (TCTR20220528002) (https://www.thaiclinicaltrials.org/) on May 18, 2022.
Data availability: The data that support the findings of this study are available from the corresponding author on reasonable request.
Study Highlights
WHAT IS KNOWN ✓ Hyperammonemia is an important contributor to hepatic encephalopathy. ✓ Bacterial translocation plays an essential role in the pathogenesis of cirrhotic complications, particularly spontaneous bacterial peritonitis. WHAT IS NEW HERE ✓ Bacterial DNA translocation is a potential factor associated with overt hepatic encephalopathy in cirrhotic patients. ✓ Detection of bacterial DNA may be a factor related to 6-month mortality in cirrhosis. ACKNOWLEDGMENTSWe thank the staff of the Division of Gastroenterology and Hepatology, Excellence Center in Liver Diseases, Center of Excellence in Hepatic Fibrosis and Cirrhosis, Faculty of Medicine, Chulalongkorn University, and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, for their technical assistance and clinical support. We thank the funding support from the Medical Council of Thailand (Police General Dr. Jongjate Aojanepong Foundation), the 90th and 100th Anniversary of Chulalongkorn University Scholarship under the Ratchadapisek Somphot Endowment Fund. We thank Assoc. Prof. Thanin Asawavichienjinda from Chulalongkorn Comprehensive Headache Center, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand, for statistical consultation.
REFERENCES 1. Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the America
留言 (0)