
記住我


Colonoscopy is a widely accepted method for diagnosing and managing many colorectal diseases, including colorectal cancer, inflammatory bowel disease, and other mucosal abnormalities (1–3). Inadequate bowel preparation (BP) may lead to missed or misdiagnosed lesions, prolonged operation duration, and increased costs due to repeated operations; for these reasons, adequate BP is essential to ensure the accuracy and safety of colonoscopy (4,5). However, studies have shown that approximately 20%–30% of patients do not have adequate BP before a colonoscopy (6,7). Patients with inadequate BP may require an additional colonoscopy within 1 year and may necessitate more aggressive BP methods (8,9). Therefore, identification of patients with an increased likelihood of inadequate BP before colonoscopy can enable endoscopists to alter the BP strategy to prevent unnecessary colonoscopies.
In previous research, many factors have been found to correlate with insufficient BP in patients. Patient-related factors include the patient's age, gender, comorbidities, medication history, and smoking history. In addition, preprocedure education, diet, and the choice of BP regimen (including the type of laxative, dosage, and timing of administration) can all affect the quality of a patient's BP (10–15). Four simple predictive models were developed to evaluate the possibility of inadequate BP (16–19). These models were based on traditional statistical methods, with small sample sizes. Because of these shortcomings, the prediction ability of these models is unsatisfactory.
The rapid development of artificial intelligence and machine learning (ML) technology has allowed researchers to overcome complex medical difficulties and achieve desirable outcomes (20–23). Theoretically, an ML model can automatically learn and identify factors affecting intestinal preparation from large volumes of patient data to provide clinicians with accurate prediction results and personalized intervention suggestions. In previous studies, ML has also been able to predict the quality of BP by identifying images of rectal effluent during the BP and guiding patients to undertake additional measures (24). However, there is still a lack of ML models that can predict the quality of BP based on patient characteristics before BP. This study aimed to determine the risk factors of inadequate BP in Chinese adults and develop a predictive model using ML to identify patients at higher risk of inadequate BP.
METHODS Study design and populationThis was a multicenter prospective study. From January 2021 to May 2023, we enrolled consecutive adult (aged 18 years or older) outpatients scheduled for screening colonoscopies at Xuanwu Hospital, Beijing Friendship Hospital, Beijing Aviation General Hospital, and Beijing Shijingshan Hospital who provided informed consent. This study protocol was reviewed and approved by the Ethics Committees of Xuanwu Hospital, Capital Medical University, approval number IRB# 20220913, and it was registered in the China Clinical Trial Registry (https://www.chictr.org.cn) as number ChiCTR2300072076.
Exclusion criteria included the following: (i) severe heart failure (New York Heart Association grades III to IV) or renal failure (serum creatinine ≥3 mg/dL); (ii) history of total/subtotal proctocolectomy; (iii) BP using a nonstandard regimen; (iv) polyethylene glycol (PEG) allergy; (v) severe mental illness; (vi) pregnancy or lactation; and (vii) incomplete colonoscopy for reasons other than BP quality.
BP and colonoscopyBoston Bowel Preparation Scale (BBPS) was used to evaluate the quality of BP (25). All centers used the standard regimen for BP. When the patients were scheduled for colonoscopy, the clinician identified those meeting the criteria for enrollment and asked them to provide informed consent for the clinical trial. All participants received oral and written instructions that asked them to intake a low-fiber diet the day before procedures and liquid diet on the day of colonoscopy. The regimen for the drinking of laxatives was highlighted in the written instructions. Three liters of PEG were used for BP. One liter was administered the night before colonoscopy and 2 L on the morning of the procedure. Each liter of PEG should be consumed within 1 hour. In addition, participants were advised to drink as much cool water as possible. All colonoscopies were performed by 10 endoscopists who had performed more than 1,000 before the study. Endoscopists from different centers held conferences every 2 months conducted online during the COVID-19 pandemic; we also invited an expert to review and ensure BBPS uniformity.
Data collectionOn the day of the appointment, data collectors acquired data using a questionnaire, including (i) baseline characteristics (age, gender, height, weight, grade of education [less than bachelor, bachelor, and over bachelor]) and smoking history; (ii) abdominal surgical history, comorbidities (diabetes, constipation, stroke, cirrhosis, and hyperthyroidism), and use of medicines (opioids, calcium antagonists, simethicone, and tricyclic antidepressants [TCAs]), which is defined as usage for more than 2 weeks and at a dosage not less than the minimum therapeutic dose; (iii) history of smoking and inadequate BP; and (iv) interval time (from the completion of BP to the start of the colonoscopy).
The primary outcome was BP quality, which the endoscopists assessed using the BBPS during the colonoscopies. The BBPS includes scores of right, transverse, and left colons. Inadequate BP was defined as a total BBPS score of less than 6 or any segment score of less than 2. The secondary outcomes included polyp detection rate and bowel bubble score, rated 0–3 in ascending order of the number of bubbles in the whole bowel before rinse and suction.
Statistical analysisContinuous variables were expressed as mean and SD, while categorical variables were expressed as frequency and percentage. The χ2 and Fisher exact tests were used to compare categorical variables, and the t test was used to test continuous variables. P values were used to describe the correlations between variables. The variables included age, gender, body mass index, grade of education, smoking history, stroke, cirrhosis, diabetes, constipation, hyperthyroidism, use of opioids, calcium antagonists, TCAs, or simethicone, abdominal or pelvic surgery history, inadequate BP history, and the interval time.
We generated a multivariate logistic regression model to evaluate the predictive ability of ML models. All patients were randomly assigned to the development and validation cohorts with a ratio of 8:2. Univariate correlation analysis was performed for each factor, and variables with a 2-sided P value less than 0.1 were included in the multifactor logistic regression analysis and model construction. In the multivariate analysis, variables with a 2-sided P value less than 0.05 were considered risk factors of inadequate BP. Support vector machines (SVMs), decision trees, extreme gradient boosting (XGB), and a bidirectional projection network (BPNet) were used to construct models.
According to the data from the development and validation cohorts, receiver operating characteristic curves were drawn to verify the prediction ability of the models. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated to obtain the optimal cutoff. Due to the imbalance between the adequate and inadequate BP ratio, the area under the receiver operating characteristic curve (AUROC, also known as C-statistic) of the validation cohort was calculated to assess the predictive capacity of the models.
Univariate analysis, multivariate analysis, and plotting of logistic regression curves were performed using the ggplot2 and rms packages in R software (version 4.2.3 for Windows, Bell Laboratories). The construction of ML models used the scikit-learn package in Python software (version 3.11.4 for Windows).
The sample size was calculated based on the events per variable method. According to the requirement of 10 samples per variable and the occurrence rate of inadequate BP in our first 300 patients (approximately 20%), the sample size required to establish a multivariate regression model with 17 variables was approximately 850. Following an 8:2 ratio, the validation cohort included 213 patients, totaling approximately 1,063. We tripled the sample size to 3,189 to train the ML models thoroughly.
RESULTS Patient characteristics and outcomesColonoscopy was performed on 4,120 outpatient patients in 4 centers; 903 patients were excluded, of whom 115 were with severe heart or renal failure, 87 were with a history of total/subtotal proctocolectomy, 519 used nonstandard BP regimens, 12 were allergic to PEG, 92 were with severe mental illness, 31 were pregnant or lactating, and 47 did not complete colonoscopy for reasons other than BP quality. The left 3,217 patients were included in the analysis. Of the whole sample, the average age was 53.86 ± 12.97 years, the median age was 54 years (interquartile range 45–63 years), and 52.63% (1,693 out of 3,217) were men. The average body mass index was 24.29 ± 3.52 kg/m2. Regarding education, 7.43% (239/3,217), 43.99% (1,415/3,217), and 48.59% (1,563/3,217) earned over bachelor, bachelor, and under bachelor, respectively. Constipation was the most common comorbidity (13.62%, 438/3,217), followed by diabetes (11.13%, 358/3,217) and a history of stroke (1.65%, 53/3,217). Hyperthyroidism was found in 0.59% (19/3,217), and cirrhosis was reported in 0.37% (12/3,217). Regarding medication use, 0.19% (6/3,217) were taking opioids, while 0.44% (14/3,217) were using TCAs. Calcium antagonists were used by 22.57% (726/3,217), and simethicone was used by 9.61% (309/3,217); 23.44% (754/3,217) had undergone abdominal or pelvic surgery, while 15.54% (500/3,217) had a smoking history, and 6.87% (221/3,217) reported a history of improper colonoscopy preparation. The average interval time was 6.08 ± 1.79 hours. A total of 13 patients were diagnosed with inflammatory bowel disease in the study.
Regarding outcomes, the average BBPS was 6.60 ± 1.64. The average score of the right colon was 2.02 ± 0.65, the transverse colon was 2.24 ± 0.64, and the left colon was 2.34 ± 0.69. Adequate BP was reported in 78.86% (2,537/3,217), with adequate preparation rates for each intestinal segment being 83.21% (2,676/3,217), 91.11% (2,931/3,217), and 90.05% (2,897/3,217), respectively. The polyp detection rate was 44.05% (1,417/3,217), and the average bowel bubble score was 0.90 ± 0.72.
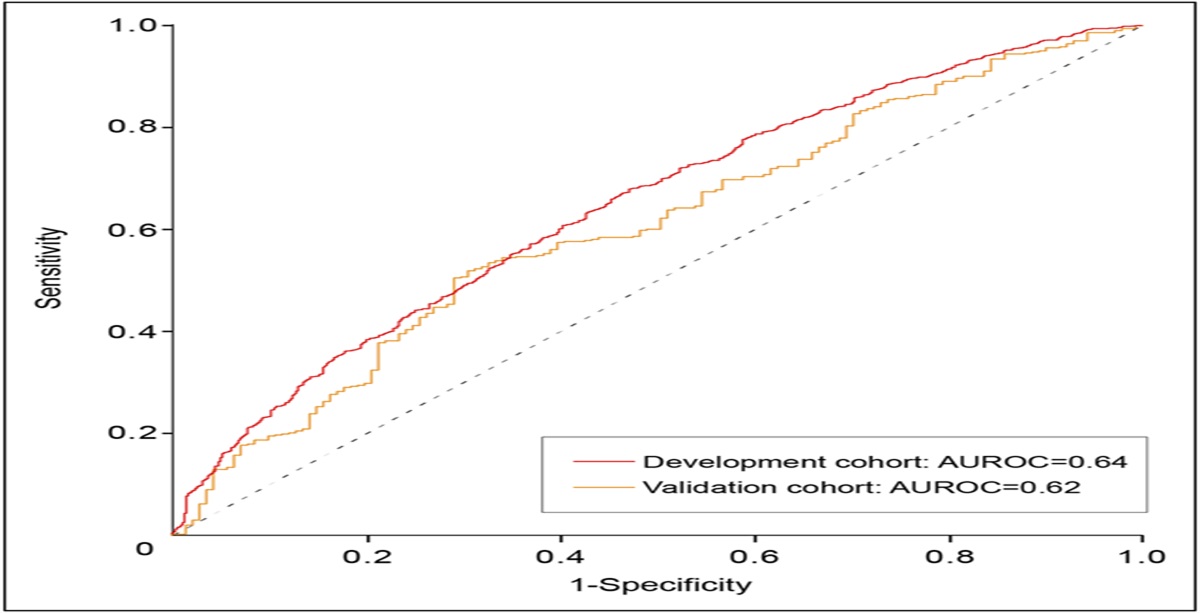
Logistic regression analysisWe randomly divided the data into 5 parts, with 4 parts as the development validation and 1 as the validation cohort. In the development cohort, 79.05% achieved adequate BP. We performed a univariate correlation analysis (Table 1). Subsequently, all factors with P < 0.1 were included in the multivariate regression analysis and used to establish a logistic regression model. Table 1 also summarizes the results of the multivariate regression. The factors associated with inadequate BP included low degree of education, diabetes, constipation, use of calcium antagonists or simethicone, history of smoke, history of inadequate BP, and longer interval time. Figure 1 shows the AUROCs of the logistic regression analysis in development and validation cohorts. The AUROC of the development cohort was 0.65 (95% confidence interval [CI] 0.62–0.67), with a sensitivity of 67.89%, specificity of 52.88%, PPV of 84.46%, NPV of 28.99%, and accuracy of 64.78%. In the validation cohort, 78.11% had adequate BP. The AUROC was 0.62 (95% CI 0.55–0.66), with a sensitivity of 50.50%, specificity of 70.92%, PPV of 78.97%, NPV of 28.86%, and accuracy of 55.04%.
Table 1. - Univariate and multivariate analyses of factors associated with inadequate bowel preparation (development cohort) Adequate bowel preparation (n = 2,034) Inadequate bowel preparation (n = 539) P value Univariate Multivariate Age, yr, mean ± SD 53.52 ± 12.91 55.29 ± 12.66 0.004 0.458 Female, n (%) 940 (46.21) 273 (50.65) 0.073 0.333 BMI, kg/m2, mean ± SD 24.25 ± 3.47 24.53 ± 3.78 0.101 — Grade of education, n (%) <0.001 0.021 Over bachelor 172 (8.46) 025 (4.64) Bachelor 919 (45.18) 216 (40.10) Under bachelor 943 (46.36) 298 (55.29) Comorbidities, n (%) Diabetes 209 (10.28) 094 (17.44) <0.001 0.004 Cirrhosis 007 (0.34) 002 (0.37) 1.000 — Stroke 032 (1.57) 009 (1.67) 1.000 — Hyperthyroidism 011 (0.54) 003 (0.56) 1.000 — Constipation 232 (11.41) 106 (19.67) <0.001 <0.001 Use of drugs, n (%) Opioids 002 (0.10) 001 (0.18) 0.506 — Tricyclic antidepressants 004 (0.20) 004 (0.74) 0.065 0.126 Calcium antagonists 429 (21.09) 152 (28.20) <0.001 0.012 Simethicone 221 (10.87) 026 (4.82) <0.001 0.003 Abdominal or pelvic surgery history, n (%) 436 (21.44) 150 (27.83) 0.002 0.143 History of smoke, n (%) 291 (14.31) 123 (22.82) <0.001 <0.001 History of inadequate bowel preparation, n (%) 127 (6.24) 056 (10.39) 0.001 0.022 Interval time, h, mean ± SD 6.02 ± 1.66 6.42 ± 2.29 <0.001 <0.001 Figure 1.:
Figure 1.: Receiver operating characteristic curves of the logistic regression model in the development and validation cohorts. AUROC, area under the receiver operating characteristic curve.
ML modelsFigure 2 shows the ML models of 4 algorithms. From A to D, there were SVM, decision trees, XGB, and BPNet, respectively. For the development cohort, the SVM model had an AUROC of 0.84 (95% CI 0.79–0.89), with a sensitivity of 64.09%, specificity of 90.10%, PPV of 85.39%, NPV of 73.53%, and accuracy of 77.76%. The decision trees model had an AUROC of 0.82 (95% CI 0.81–0.83) for the development cohort, with a sensitivity of 95.49%, specificity of 69.34%, PPV of 59.07%, NPV of 97.07%, and accuracy of 78.14%. For the XGB model, the AUROC was 0.77 (95% CI 0.75–0.79), with a sensitivity of 51.61%, specificity of 99.81%, PPV of 99.59%, NPV of 69.55%, and accuracy of 76.94%. The BPNet model had an AUROC of 0.81 (95% CI 0.79–0.83), with a sensitivity of 71.18%, specificity of 75.92%, PPV of 72.75%, NPV of 74.48%, and accuracy of 73.67%.
 Figure 2.:
Figure 2.: Receiver operating characteristic curves of the machine learning models in the development and validation cohorts. (a) Model by support vector machines. (b) Model by decision trees. (c) Model by extreme gradient boosting. (d) Model by bidirectional projection network. AUROC, area under the receiver operating characteristic curve.
Table 2 summarizes the results of the predictive capacity for the validation cohort of the 4 models. The decision trees model showed the best prediction capacity according to the AUROC of the validation cohort. The risk factors at the nodes included body mass index, education grade, use of simethicone, diabetes, age, history of inadequate BP, and longer interval time (Figure 3).
Table 2. - Predictive capacity of different models Sensitivity, % Specificity, % PPV, % NPV, % Accuracy, % AUROC (95% CI) LR 50.50 70.92 78.97 28.86 55.04 0.62 (0.55–0.66) SVM 57.21 81.95 76.88 64.62 69.29 0.76 (0.71–0.81) DT 73.95 72.68 73.95 72.68 73.33 0.80 (0.78–0.82) XGB 53.95 100 100 67.43 76.43 0.77 (0.72–0.82) BPNet 64.18 63.26 66.67 63.84 65.24 0.71 (0.70–0.72)AUROC, area under the receiver operating characteristic curve; BPNet, bidirectional projection network; CI, confidence interval; DT, decision trees; LR, logistic regression; NPV, negative predictive value; PPV, positive predictive value; SVM, support vector machines; XGB, extreme gradient boosting.
 Figure 3.:
Figure 3.: Decision trees. BMI, body mass index; BP, bowel preparation.
We performed a decision curve analysis revealing that the net benefit at a threshold probability of 0.55 was 0.20. This value equates to identifying 20 patients with inadequate BP per 100 patients. The ratio was nearly the incidence of inadequate BP in this study; therefore, the decision trees model was deemed the most appropriate for identifying patients at risk of inadequate BP (Figure 4).
 Figure 4.:
Figure 4.: Decision curve analysis of the decision trees model.
DISCUSSIONWe reported an inadequate BP rate of 21.14%, similar to our previous study (26). Multivariate regression revealed that the predictive factors were inconsistent with previous studies (7,27). This study did not find a significant impact of opioids and TCA medications on the quality of BP, which is inconsistent with the results of previous studies, particularly those conducted in developed countries such as in Europe and America (17,18). However, in our study, we observed that patients taking these 2 classes of medications had a higher rate of poor BP than control patients, although the difference was not statistically significant. In China, all psychotropic medications are strictly regulated, resulting in lower usage rates, which may not reveal a significant difference. In this study, lower education grade was related to inadequate BP, unlike the result of ’ the study conducted by Vincent (17). Simethicone is believed to affect the bowel bubble score. However, it significantly correlated with BBPS in this study. We speculate that simethicone improves the BBPS by reducing the adhesion of feces to the intestinal wall. Furthermore, patients with inadequate BP had longer interval time. However, according to other studies, the risk of inadequate BP increases when the interval is shorter than 3 hours or longer than 8 hours (28,29).
As a rapidly evolving technology, ML has already found numerous applications in colonoscopy screening. Beyond aiding endoscopists in identifying colorectal polyps, ML has also been used for predicting the quality of BP before colonoscopy (30). For example, 1 study integrated an ML model into a smartphone application, allowing patients to take photographs of the rectal effluent during the BP. The app could then predict the volume of fecal residue during colonoscopy based on these images (24). Because traditional prediction models for BP have not been able to yield better predictive power, we have explored the use of ML methods for modeling. To select the model with the best performance, we established 4 models using different algorithms. The decision trees model demonstrated the best predictive capacity, with an AUROC of 0.80 in the validation cohort. The decision trees model is a tree-based algorithm that recursively splits the dataset based on the feature that provides the highest information gain or the lowest impurity (31–33). We used an information gain algorithm to build the model. To avoid overfitting, we applied pruning techniques by limiting the maximum depth of the tree to 10 and setting a minimum number of samples required to split a node at 10. The decision trees model is interpretable and beneficial for clinical use (34). As the decision curve analysis showed, when the threshold probability was set as 0.55, the benefit net was 0.2. This finding demonstrates the practicability of the model. Therefore, although the AUROC of this study did not show a substantial improvement compared with previous clinical models (16–19), the clinical decision curve of the model has demonstrated its practical utility in a clinical setting. The decision trees model has been used to establish models for colorectal cancer screening, treatment, and outcomes (35–37). However, as a step before colonoscopy, the risk factors of BP quality have not been verified using ML models.
This study has several limitations. First, although it was a prospective multicenter study, the patients were all from Beijing; therefore, the model may not be generalizable to other populations. We are currently collecting patient data from regions outside of Beijing and plan to use these data for external validation of our model. Second, we attempted to validate the model with databases from different countries and races, similar to what was described in a model concerning coronary artery disease (38). However, no public database related to BP existed. Third, the study relied on self-reported data for some variables, which may be subject to recall bias. Fourth, the study did not include all potential factors influencing BP, such as dietary habits and physical activity. Finally, although the decision trees model predicts patients with inadequate BP, there is no universal agreement regarding designing a suitable screening program. Studies focused on patients with adequate BP; it is necessary to perform studies to help patients with inadequate BP.
In conclusion, this study identified several risk factors of inadequate BP and developed a decision tree model with good predictive capacity. This model can identify patients at higher risk of inadequate BP before colonoscopy, allowing for personalized BP strategies to be implemented. For this group of patients, BP may require a higher dose of PEG or the addition of other auxiliary medications (39). By applying this ML model, the quality of BP will be improved through better visualization and preventing unnecessary repeat colonoscopies.
CONFLICTS OF INTERESTGuarantor of the article: Huihong Zhai, MD, PhD.
Specific author contributions: F.G., J.N.X., and H.H.Z.: conceptualization and design. All authors: acquisition, analysis, or interpretation of data. F.G.: drafting of the first manuscript. J.N.X. and H.H.Z.: critical revision of the manuscript for important intellectual content. F.G. and J.N.X.: statistical analysis. H.H.Z.: supervision and project administration. All authors have read and approved the final version of the manuscript submitted.
Financial support: This study was supported by National Natural Science Foundation of China (No. 8197031585) and the Project Foundation of Chinese Nursing Association (ZHKY202103).
Potential competing interests: None to report.
Statement of ethics: This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Written informed consent was obtained from participants (or their parent/legal guardian/next of kin) to participate in the study. This study protocol was reviewed and approved by Ethics Committees of Xuanwu Hospital, Capital Medical University, approval number IRB# 20220913, and it was registered in the China Clinical Trial Registry (https://www.chictr.org.cn) as number ChiCTR2300072076.
Data availability statement: Huihong Zhai takes full responsibility for the conduct of the study. She has access to the data and control of the decision to publish. Template data collection forms, data used for all analyses, analytic code, and any other materials used in the article are available from the corresponding author on request.
Study Highlights
WHAT IS KNOWN ✓ Colonoscopy is important for the early detection of colorectal cancer. ✓ The quality of bowel preparation can affect the detection rate. ✓ It is hard to indicate the patients who will get inadequate bowel preparation before colonoscopy. WHAT IS NEW HERE ✓ A decision trees model was built to predict the bowel preparation. ✓ The predict effectiveness is better than the traditional models. ACKNOWLEDGMENTWe gratefully express our gratitude to Zhenjie Lv for the avenues of statistical analysis he has provided. We gratefully acknowledge the financial supports by the National Science Foundation of China under Grant numbers (No. 8197031585).
REFERENCES 1. Lieberman D, Ladabaum U, Cruz-Correa M, et al. Screening for colorectal cancer and evolving issues for physicians and patients: A review. JAMA 2016;316(20):2135–45. 2. Rex DK, Boland CR, Dominitz JA, et al. Colorectal cancer screening: Recommendations for physicians and patients from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2017;153(1):307–23. 3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71(3):209–49. 4. Bechtold ML, Mir F, Puli SR, et al. Optimizing bowel preparation for colonoscopy: A guide to enhance quality of visualization. Ann Gastroenterol 2016;29(2):137–46. 5. Guo F, Chen C, Holleczek B, et al. Strong reduction of colorectal cancer incidence and mortality after screening colonoscopy: Prospective cohort study from Germany. Am J Gastroenterol 2021;116(5):967–75. 6. Lebwohl B, Kastrinos F, Glick M, et al. The impact of suboptimal bowel preparation on adenoma miss rates and the factors associated with early repeat colonoscopy. Gastrointest Endosc 2011;73(6):1207–14. 7. Amitay EL, Niedermaier T, Gies A, et al. Risk factors of inadequate bowel preparation for screening colonoscopy. J Clin Med 2021;10(12):2740. 8. Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: Recommendations from the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 2014;109(10):1528–45. 9. Pantaleon Sanchez M, Gimeno Garcia AZ, Bernad Cabredo B, et al. Prevalence of missed lesions in patients with inadequate bowel preparation through a very early repeat colonoscopy. Dig Endosc 2022;34(6):1176–84. 10. Rostom A, Jolicoeur E. Validation of a new scale for the assessment of bowel preparation quality. Gastrointest Endosc 2004;59(4):482–6. 11. Nguyen DL, Wieland M. Risk factors predictive of poor quality preparation during average risk colonoscopy screening: The importance of health literacy. J Gastrointestin Liver Dis 2010;19(4):369–72. 12. Rex DK, Katz PO, Bertiger G, et al. Split-dose administration of a dual-action, low-volume bowel cleanser for colonoscopy: The SEE CLEAR I study. Gastrointest Endosc 2013;78(1):132–41. 13. Hassan C, East J, Radaelli F, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline: Update 2019. Endoscopy 2019;51(8):775–94. 14. Agrawal R, Majeed M, Attar BM, et al. Predictors of poor bowel preparations and colonoscopy cancellations in inpatient colonoscopies, a single center retrospective study. Transl Gastroenterol Hepatol 2022;7:4. 15. Gao Y, Lin XJ. Effect of bowel preparation to colonoscopy interval on preparation quality and colonoscopy outcomes: A meta-analysis. Turk J Gastroenterol 2023;34(1):26–34. 16. Hassan C, Fuccio L, Bruno M, et al. A predictive model identifies patients most likely to have inadequate bowel preparation for colonoscopy. Clin Gastroenterol Hepatol 2012;10(5):501–6. 17. Dik VK, Moons LM, Huyuk M, et al. Predicting inadequate bowel preparation for colonoscopy in participants receiving split-dose bowel preparation: Development and validation of a prediction score. Gastrointest Endosc 2015;81(3):665–72. 18. Gimeno-Garcia AZ, Baute JL, Hernandez G, et al. Risk factors for inadequate bowel preparation: A validated predictive score. Endoscopy 2017;49(6):536–43. 19. Fuccio L, Frazzoni L, Spada C, et al. Factors that affect adequacy of colon cleansing for colonoscopy in hospitalized patients. Clin Gastroenterol Hepatol 2021;19(2):339–48.e7. 20. Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med 2019;25(1):24–9. 21. Topol EJ. High-performance medicine: The convergence of human and artificial intelligence. Nat Med 2019;25(1):44–56. 22. Shu L, Tang J, Liu S, et al. Plasma cell signatures predict prognosis and treatment efficacy for lung adenocarcinoma. Cell Oncol (2023). http://dx.doi.org/10.1007/s13402-023-00883-w 23. Wang J, Ren F, Wang Y, et al. Urinary exosomal tRNA-derived small RNA signatures as a predictive biomarker in lung cancer. FEBS Open Bio 2024. https://doi.org/10.1002/2211-5463.13716 24. Zhu Y, Zhang DF, Wu HL, et al. Improving bowel preparation for colonoscopy with a smartphone application driven by artificial intelligence. NPJ Digit Med 2023;6(1):41. 25. Lai EJ, Calderwood AH, Doros G, et al. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointest Endosc 2009;69(3 Pt 2):620–5. 26. Guo R, Wang YJ, Liu M, et al. The effect of quality of segmental bowel preparation on adenoma detection rate. BMC Gastroenterol 2019;19(1):119. 27. Shi L, Liao F, Liao W, et al. Risk factors for inadequate bowel preparation before colonoscopy: A retrospective cohort study. BMC Gastroenterol 2023;23(1):204. 28. Kim TK, Kim HW, Kim SJ, et al. Importance of the time interval between bowel preparation and colonoscopy in determining the quality of bowel preparation for full-dose polyethylene glycol preparation. Gut Liver 2014;8(6):625–31. 29. Sun J, Chen Y, Gu Y, et al. Graphical education and appropriate time before elective colonoscopy make better bowel preparation. J Minim Access Surg 2023;19(1):130–7. 30. Gimeno-Garcia AZ, Benitez-Zafra F, Nicolas-Perez D, et al. Colon bowel preparation in the era of artificial intelligence: Is there potential for enhancing colon bowel cleansing? Medicina (Kaunas) 2023;59(10):1834. 31. Salzberg SL. C4.5: Programs for machine learning by J. Ross Quinlan. Morgan Kaufmann Publishers, Inc., 1993. Machine Learn 1994;16:235–40. 32. Kotsiantis SB. Decision trees: A recent overview. Artif Intell Rev 2013;39(4):261–83. 33. Probst P, Wright M, Boulesteix AL. Hyperparameters and tuning strategies for random forest. arXiv 2018. doi:10.48550/arXiv.1804.03515 34. Bae JM. Clinical decision analysis using decision tree. Epidemiol Health 2014;36:e2014025. 35. Nopour R, Shanbehzadeh M, Kazemi-Arpanahi H. Developing a clinical decision support system based on the fuzzy logic and decision tree to predict colorectal cancer. Med J Islam Repub Iran 2021;35:44. 36. Su Y, Tian X, Gao R, et al. Colon cancer diagnosis and staging classification based on machine learning and bioinformatics analysis. Comput Biol Med 2022;145:105409. 37. Zhang Y, Zhang Z, Wei L, et al. Construction and validation of nomograms combined with novel machine learning algorithms to predict early death of patients with metastatic colorectal cancer. Front Public Health 2022;10:1008137. 38. Forrest IS, Petrazzini BO, Duffy A, et al. Machine learning-based marker for coronary artery disease: Derivation and validation in two longitudinal cohorts. Lancet 2023;401(10372):215–25. 39. Chen L, Kang X, Ren G, et al. Individualized intervention based on a preparation-related prediction model improves adequacy of bowel preparation: A prospective, multi-center, randomized, controlled study. Dig Liver Dis 2024;56(3):436–43.
留言 (0)