
記住我
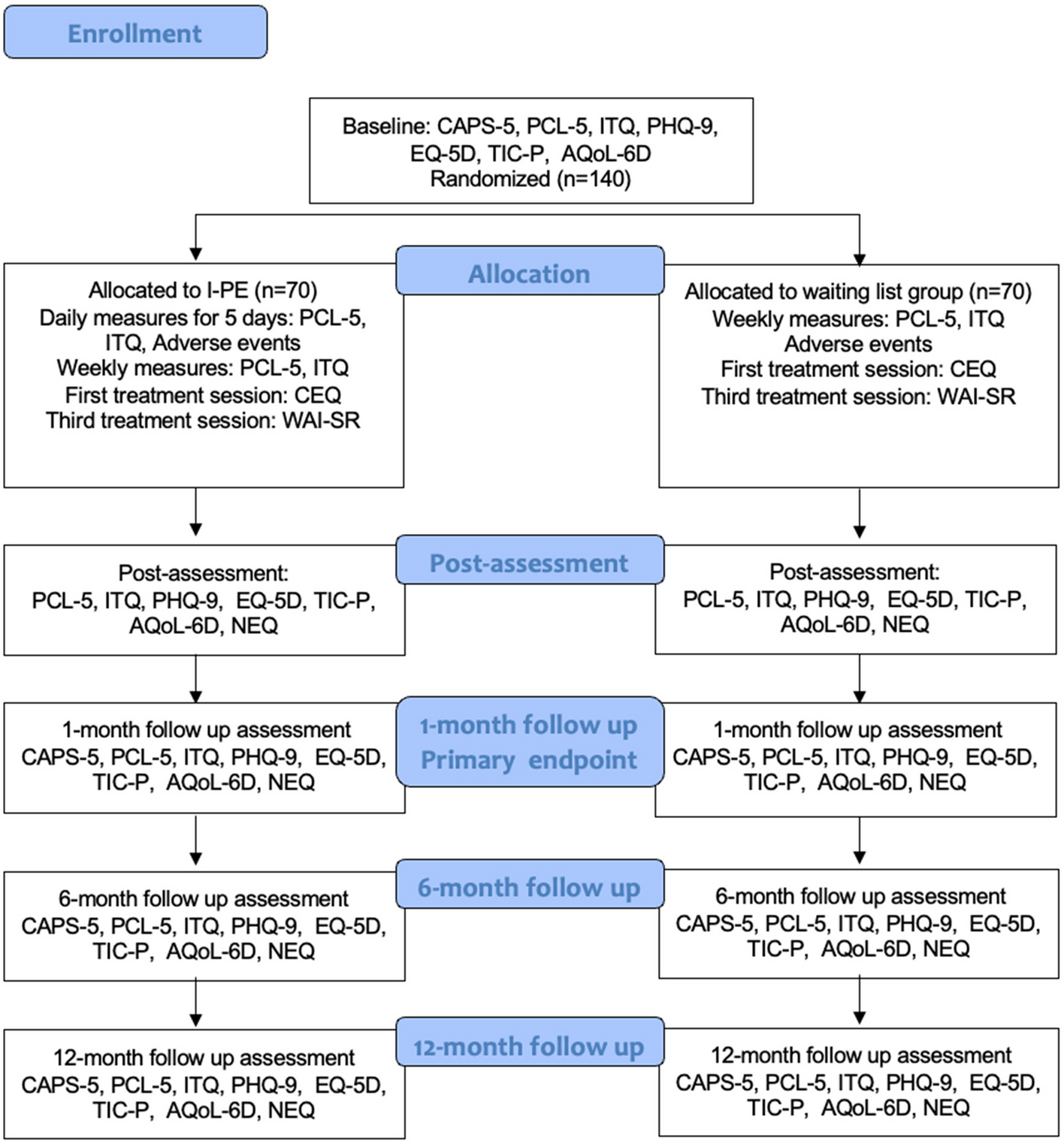


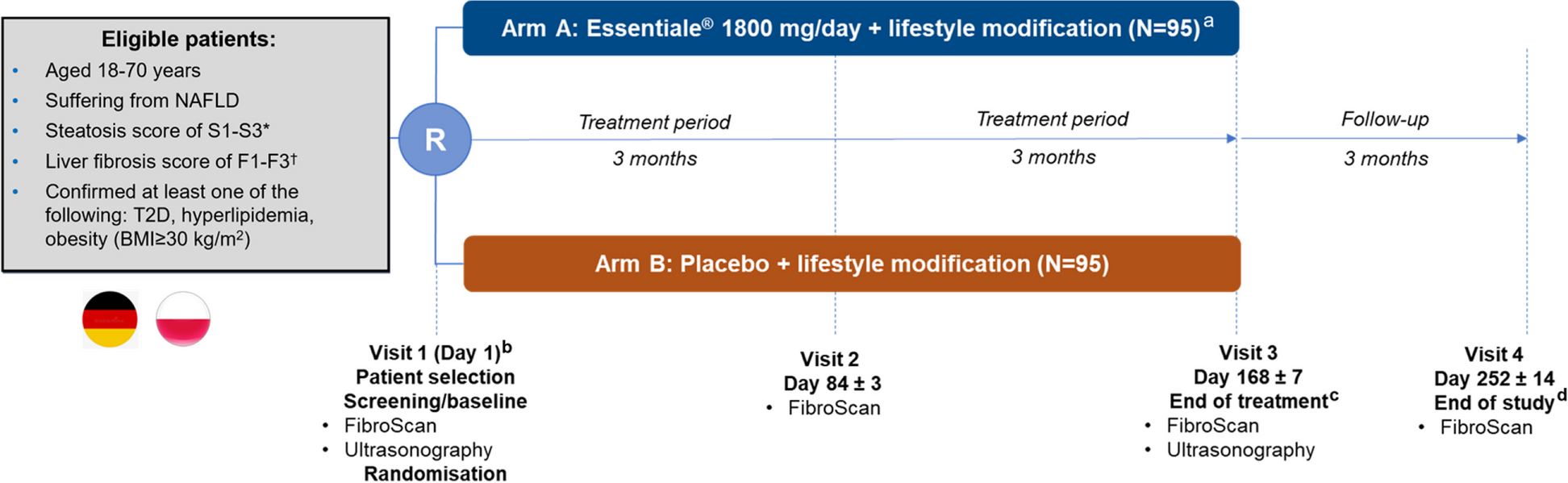

Figure 1 shows included RCTs and responses from authors approached. Sixty-two RCTs were eligible for inclusion from the original sample of 96 [7]. We were able to email the authors of 59 trials and 14 responded (response rate 24%) with PILs from trials published between 2005 and 2018.
Fig. 1
Sampling, approach and responses from eligible RCTs from Cousins et al. [7]
Characteristics of RCTs of included PILsOf the included trials, the majority were trials with sites only in Europe (n = 8, 57%) and they involved various surgical specialties (Table 1). In one case, PILs were provided from two RCTs testing the same intervention within the ear, nose and throat. Sample sizes across the 14 RCTs ranged from 22 to 313 (median = 77) and where the number of centres was reported this ranged from 1 to 36. Most (n = 10) included a high-fidelity placebo comparator, i.e. one which closely resembles the surgical procedure under evaluation except that the key component has been removed.
Table 1 Characteristics of included PILsFrequency of information items within PILsOverall, most of the PILs in the sample included general items on trial design with at least 50% of all PILs covering content such as the purpose of including a placebo; blinding (and timing of unblinding) of the trial team and participants; and whether those receiving placebo will be offered the intervention at end of study (Table 2). The most frequently reported items within the PILs were within the intervention description section, with both a description of components of the placebo and a description of the intervention being reported in all PILs analysed. Yet, explanations of how the placebo differs or is similar to the surgical intervention (i.e. fidelity) were only reported in 6 (43%) of the included PILs.
Table 2 Analysis of content items across PILsWhen considering the presence of information on the risks and benefits of the placebo comparator and the surgical intervention, the majority (57%) of the PILs included information on the potential therapeutic benefits of the surgical intervention. One (7%) of the PILs included information on potential indirect therapeutic improvements from invasive components of the placebo, with a further PIL including information on the potential non-therapeutic effects of the placebo intervention. With regard to risk information, again only a small number (n = 5, 36%) presented the known risks of the placebo intervention, whilst 57% (n = 8) presented information on the known risk of the surgical intervention. Only two PILS included descriptions of the differences in potential risks between surgical and placebo interventions. Most of the included PILs did not separate the potential benefits or risks associated with the placebo or the surgical interventions individually.
The following section of the findings considers the specific content items identified in the frequency analysis of information content of the placebo surgical trials PILs.
Purpose of including a placebo interventionOf the 14 included PILs, seven (50%) included information on the purpose of including a placebo intervention in the trial. One PIL stated that conflicting results from previous studies were largely due to participants being unblinded and over/underestimating effects on outcome. Other PILs stated that the purpose was to ‘be absolutely certain of the value of’ the surgery, or to ‘allows us to make a proper comparison of the effect without being biased’ so as ‘to scientifically and objectively evaluate a treatment method of this kind’. One PIL gave the following justification:
This particular study design is the only possible way to ultimately provide evidence whether the treatment is effective and to establish that the observed outcomes are not down to a so-called “placebo effect”.
Term(s) used to describe placebo and surgical interventionsAll 14 PILs included terms to describe the placebo intervention. A range of different words were used as descriptors, which included (and some PILs used more than one term to describe): control (n = 3); placebo (n = 3); mock [surgery] (n = 2); sham (n = 2); ‘treatment without [intervention]’ (n = 2); dummy treatment (n = 1); medical treatment alone (n = 1); placebo surgery (n = 1); and type of surgery (n = 1). Terms used to describe the treatment intervention with the PILs focussed on treatment (n = 3), active (n = 2), actual surgery (n = 1), experimental (investigational) device or procedures (n = 1), new (n = 1), real surgery (n = 1) and surgical treatment (n = 1);
Explanation of how the placebo differs or is similar to the surgical intervention (fidelity)Content on placebo fidelity (i.e. how the placebo differs or is similar to the surgical intervention) was included in a number of PILs. These PILs discussed this in terms of how the procedure was similar to the surgical intervention, e.g. ‘Apart from the shaving away of a small amount of bone that sits above the tendons, the operation is very similar to the shoulder arthroscopy (above).’ (high fidelity placebo), and ‘if you are assigned to the control group, you will be treated in the same way as patients in the actual surgery group before and after surgery. The muscles or the nerves, however, will not be removed.’ (low fidelity placebo). However, within some PILs the content described the difference between the surgical intervention and placebo as a dichotomy, e.g. ‘the other group (called a “control” group) will NOT receive a sphincterotomy’ (medium fidelity placebo).
Inclusion of information on benefits and risks of placebo and surgical interventionOnly one PIL included content in relation to potential placebo/non-therapeutic effects from the placebo intervention, stating: ‘Sometimes, people feel better due to a “placebo effect”—that is, they expect to feel better because something may have been done to help their condition’. The study that included information on the potential therapeutic improvements from invasive components of the placebo (in this case a diagnostic bronchoscopy) stated that it could lead to a diagnosis of (lung) cancer or detect ‘potential airways abnormalities, polyps, or foreign objects’. Information about known risks related to the placebo intervention focussed on the risks associated with anaesthesia or the intervention or the combination, e.g. ‘Rarely, there are allergic reactions to the local anaesthesia.’; ‘those patients who are allocated to the medication only group may require a third procedure in which they have coronary stenting. This will be an additional risk and will be the same as that of routine coronary angioplasty (1 in 100 risk of major bleeding, death, heart attack or stroke following coronary angioplasty).’; and ‘The risks associated with bronchoscopy are related to sedation and the procedure itself’.
留言 (0)