
記住我





Patient recruitment takes place in North Rhine-Westphalia, Germany, in four hospitals of the miners’ health insurance company (’Knappschaft’) with a total of eight centres: Dortmund, Bottrop, Marl, Lünen, Kamen, Gelsenkirchen, Recklinghausen and Lütgendortmund. The hospitals are academic teaching hospitals of the University of Duisburg-Essen and the Ruhr University Bochum.
Eligibility criteria Inclusion criteriaAge ≥ 18 years
Admitted to one of the participating hospitals
Health insured with ‘Knappschaft-Bahn-See’
Existing chronic renal disease (either already known and documented in the hospital information system as diagnoses ICD-10 N04.9, N17.99, N18.1–9, N19, R31, R80, or identified during hospitalisation (as distinct from acute renal failure))
Risk of end-stage renal disease within 5 years according to KFRE score of at least 15% (date of laboratory determination before 20 June 2023) or at least 9% (since 20 June 2023), respectively; see the section ‘Participant timeline ’ for details on this change.
Consent to contacting the general practitioner (GP) and specialists after discharge
General state of health sufficient for study participation
Exclusion criteriaPregnancy
Patients with ≥ 2 consultations with a nephrology specialist in the last 12 months before study inclusion
Inclusion in the MinDial study during a previous hospitalisation
Who will take informed consent?The study nurses inform eligible patients about the study and ask them if they consent to participate. If a patient has questions that cannot be answered by the study nurse, a study physician will be consulted before confirming the consent forms with the patient’s signature.
Additional consent provisions for collection and use of participant data and biological specimensIn the informed consent form, participants may optionally consent to provide their health insurance data for further assessment following the study.
InterventionsExplanation for the choice of comparatorsThe control group receives standard care, i.e. patients are discharged from the hospital as usual. This is the comparator of choice since the aim of the study is to assess if a risk-based appointment with a nephrology specialist reduces disease progression compared to current routine care.
Intervention descriptionThe intervention consists of making an appointment with a nephrology specialist as part of hospital discharge management for patients in the intervention group. Control patients will not receive a study-related intervention. In detail, the intervention is organised as follows: A nephrology study nurse selects three nephrologists near the patient’s home. The patient selects a specialist from this list, with whom an appointment is then scheduled within the next three months after discharge. The study nurse at the respective site then passes the appointment on to the patient.
Criteria for discontinuing or modifying allocated interventionsIf a study patient turns out to suffer from acute instead of chronic renal insufficiency, the intervention is cancelled for this patient. These patients are excluded from further follow-up.
Strategies to improve adherence to interventionsOne week after the agreed appointment, the study nurse calls the intervention patients to ask whether they have kept their appointment with the nephrologist and, if not, whether the nurse should arrange a new appointment.
Relevant concomitant care permitted or prohibited during the trialAny concomitant treatments and measures are permitted during the trial.
Provisions for post-trial careNo provisions are made for ancillary care, post-trial care or compensation. Patients in the control group are treated as in routine care and it can be expected that the intervention, consisting of an appointment with a nephrologist, will not be detrimental to the patient.
Outcomes Primary endpointThe eGFR was chosen as the primary parameter because it is considered a good indicator for the assessment of kidney patients and has also been used in numerous nephrology studies over time [18].
Secondary endpointsDifferences between intervention and control group, 12 months after hospital discharge:
Difference in proportion (%) of patients with controlled blood pressure (≤ 140/90 mmHG)
For diabetics: difference in proportion (%) with guideline-compliant HbA1c (6.5 to ≤ 7.5%)
Difference in proportion (%) of patients with non-guideline-compliant care about the prescription of selected medication groups (including statins, RAS blockers, ARBs and ACEIs; based on pre-specified ATC codes classified as non-guideline-compliant) according to the assessment of medication plans by consultant nephrologists
Difference in the proportion (%) of patients with non-guideline-compliant medication (resulting from the aforementioned assessment of medication plans by several consultant nephrologists)
Difference in the mortality rate (%)
Health economicsIntervention costs and costs of medical service utilisation in relation to the primary and secondary endpoints based on cost-effectiveness analyses
Process quality, acceptance and feasibility a)Comparison between intervention and control group:
b)Intervention patients:
Perceived quality of care (Patient Reported Outcome [PRO], 3 + 12 months), after 3 months incl. factors from the patient’s perspective that led to non-utilisation of nephrology care
Perception of illness (PRO: Brief-Illness-Perception-Questionnaire [BIPQ], 3 + 12 months)
Knowledge about kidney disease (PRO: Perceived Kidney Knowledge Survey [PIKS], 3 + 12 months)
Health-related quality of life (PRO: Short Form 12 [SF12], 3 + 12 months)
c)Control patients:
Perception of illness (PRO: BIPQ, 12 months)
Knowledge about the kidney disease (PRO: PIKS, 12 months)
Health-related quality of life (PRO: SF12, 12 months)
d)GPs/specialists:
Acceptance and feasibility of this new form of care (risk-based appointment scheduling): Semi-structured interviews with specialists (N = 4, 30 min) and GPs (N = 8, 20 min)
Participant timeline ScreeningFor newly admitted patients, the information on the patient in the hospital information system (HIS) is checked for known concomitant renal disease (ICD10 codes: N04.9, N17.99, N18.1-0.9, N19, R31, R80) or newly detected impaired renal function (eGFR < 60 ml/min/1.73 m2). If chronic renal disease is indicated, the patient’s 5-year ESRD risk will be estimated using the KFRE formula.
Evaluation of eligibilityIf a study patient meets all inclusion criteria and none of the exclusion criteria, this is indicated to the corresponding study nurse in the HIS. In the first step, the study nurse classifies this patient (Fig. 2), assessing whether the patient has chronic renal disease based on the available patient data and entries in the HIS. If chronic renal disease appears certain, the patient will be informed about the study and asked for consent.
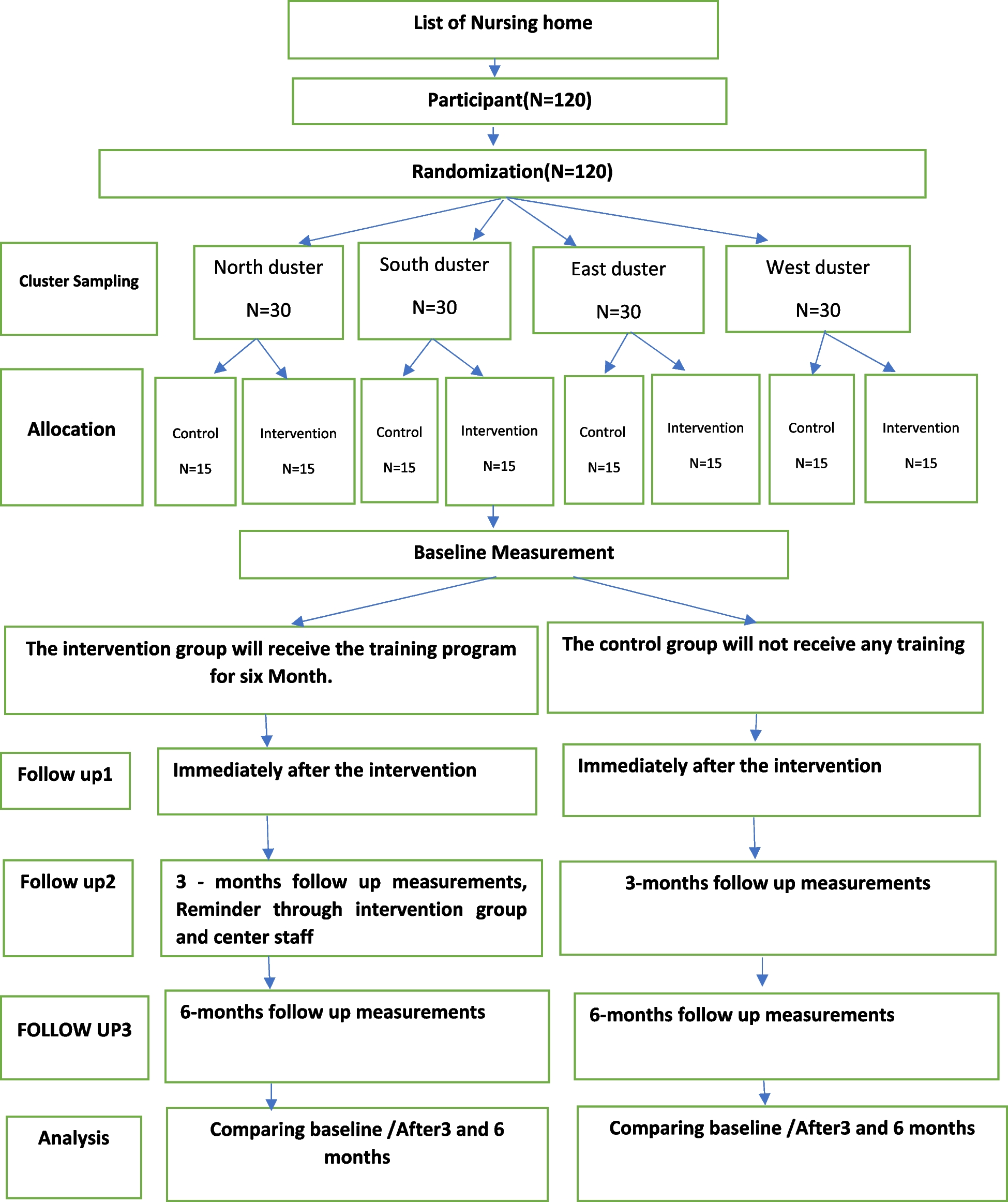
Fig. 2
Patient enrolment and follow-up in the MinDial study. Generally, eligibility is assessed by the study nurses. In doubtful cases, the decision for or against inclusion is made by study physicians, as detailed in this section
Consultation (study physicians)If the study nurse cannot determine a definite chronic renal disease or study eligibility appears questionable due to critical health conditions (infirm prognosis, the patient may not survive the study), the electronic medical record will be forwarded to a study physician for evaluation. Therefore, a special mask implemented for this study in HIS is used, where the study nurses can tag a patient and additionally leave a note with the emerged question. The next time the patient is checked by the study doctor, he can immediately see the marked patients, process the requests and mark the patients back for the study nurses.
Recruitment (or exclusion from the study)After a positive assessment of the patient by the study nurse or study physician, the informed consent form and an initial questionnaire are printed for the corresponding patient. After the study nurse has informed the patient about the study and the patient or the legal guardian has consented to the study participation, the patient is moved to the category ‘has consented’ in the HIS, and the informed consent form, as well as the initial questionnaire, is scanned and stored in the HIS.
The exclusion of patients from the study is documented with corresponding reasons.
Baseline dataOnce a patient is recruited for the study, he or she is entered into an electronic case report form (eCRF, Clincase). The patient receives an identification number, the so-called Clincase key. This key is also used for subsequent pseudonymised merging with possible additional health insurance data, which can be coded with an insurance key. Subsequently, the study-relevant patient data are transferred to the eCRF (details on the data collection are depicted in Table 1).
Table 1 Variables of interest and time of collectionTo document serum creatinine, KFRE score, blood pressure and HbA1c in the eCRF, all values are taken at a time interval around the date when the KFRE score is ≥ 15% (date of laboratory determination before 20 June 2023) or ≥ 9% (since 20 June 2023) for the first time in the current case.
Follow-up Three-month follow-up after discharge (intervention patients)Three months after discharge, intervention patients are contacted by mail and asked to fill out a questionnaire. Patients are asked whether they utilised the appointment by the nephrologist and if yes, how they assess the benefit of this referral. In addition, their quality of life (SF12), the knowledge about their kidney disease (PIKS), and how they perceive their disease (BIPQ) are asked via standardised questionnaires.
Twelve-month follow-up (all patients)One year after discharge from the hospital, a follow-up is performed for each patient regarding renal function, HbA1c, blood pressure, medication, frequency of physician visits, quality of life, knowledge about the disease and illness perception. For this purpose, the GP and/or nephrologist are contacted by the study nurse by mail and/or phone to check the vital status of the patient and to request laboratory data concerning serum creatinine and Hba1c in diabetic patients, as well as the latest three blood pressure measurements, the number of patients visits during the last year, incident diabetes and the actual medication (via the standardised medication plan). The medication is assessed whether relevant medication classes are included (antihypertensives, statins, ACE inhibitors or RAAS blockers, and SGLT2).
The data collected at the 3-month and 12-month follow-ups are detailed in Table 1, together with the baseline data.
QuestionnairesIn principle, the questionnaires are to be answered by the study participants themselves. If this is not possible for elderly or mentally incompetent patients, the legal guardian can answer the questionnaires for the patient. It is documented whether the answers were given exclusively by the caregiver/relatives or by the patients themselves.
Sample size Original sample size calculation (before shifting from 4 to 8 clusters)The sample size calculation was based on the primary endpoint. If after 12 months there is a mean difference in the decline of eGFR of 2 ± 4 ml/min/1.73 m2 (according to CKD-EPI; Cohen’s d = 0.5) between the control and intervention groups, in the cross-sectional complete cluster-randomised design chosen here (4 clusters, 4 steps, 5 measurement time points/periods), a difference can be detected in a linear mixed model with the Wald z-test for equality of means at the two-sided significance level α = 5% with a power of 80%, when 340 observations are available (PASS, version 15.0.3). Here, an intra-cluster correlation coefficient of 0.02 was assumed; this magnitude seems realistic, since the intervention is not directed at the treating physicians in the hospitals, but at the patients [19]. Furthermore, the assumed standard deviation of σ = 4 ml/min/1.73 m2 (assuming an eGFR variability [20] of 10% of the maximum eGFR of 40 ml/min/1.73 m2 expected in the patient population) seems realistic, and the mean difference of 2 ml/min/1.73 m2 seems achievable as well as clinically relevant [4]. Since we anticipate a drop-out of 20% at 12 months follow-up, n = 425 patients should be enrolled in the study, 85 in each of the 3-month periods until the next change of a cluster to the intervention phase.
Updated power calculation for the stepped-wedge design with 8 clustersBefore the start of the project, it was assumed that the shift from control to intervention conditions would have to take place simultaneously at all sites of a hospital (each with two sites) and that a design with four clusters would therefore have to be used. As it became clear that the eight sites were independent of each other in this respect, a design with one cluster per site was used instead, to improve the statistical power with the same use of resources.
An analysis of hospital data from 2020/21 after the project started had shown that recruitment numbers were expected to vary widely between sites in some cases. Assuming that 340 patients with complete follow-up would be recruited as planned, the following distribution among the 8 sites could be expected: 77, 63, 50, 37, 37, 34, 25 and 17 participants. By switching to a design with 8 clusters (one cluster per site) and under otherwise unchanged assumptions for the sample size calculation, a power of 87.5% was now expected before randomisation (R version 4.1.3, CRTpowerdist version 0.4.0 [21]). Since the actual power depends on the randomisation result, randomisation was performed under the constraint of largely balanced expected intervention and control group sizes. For this purpose, the set of possible randomisation outcomes was restricted to those where a maximum size difference between the intervention and control group of 20 subjects was expected. This corresponded to the exclusion of the less balanced half of all theoretically possible randomisations.
Second update of the power calculation (based on interim sample size)In the fourth quarter of 2023, the statistical power was recalculated. In contrast to the previous calculations, actual recruitment figures were taken into account for each site and recruitment period (for periods 1–7; projections based on past recruitment numbers were used for periods 8–13). For an optimistic prediction of future recruitment numbers, the mean values of the three stronger recruitment periods were assumed. According to this prediction and factoring in a 20% drop-out rate, 286 patients with complete follow-up are expected to be available for the final analysis.
Considering the slow recruitment, it was decided to switch to one-sided testing to increase statistical power. In the original planning, impartial two-sided testing was planned, which would have allowed verification of both an advantage and a disadvantage of the intervention. On the one hand, it is much more relevant in the context of health care to prove an advantage of the intervention than a disadvantage. On the other hand, it is more likely to assume an advantage (of unknown magnitude) than patients getting worse in terms of their kidney function as a result of an appointment with a nephrologist.
With one-sided testing and otherwise unchanged assumptions (regarding effect size, intra-cluster correlation coefficient and significance level), this corresponds to a power of 72.1% (R version 4.3.2, swCRTdesign version 4.0 [22]). The power would be 80.0% if the actual mean difference in the decrease in eGFR is 2.23 ml/min/1.73 m2 instead of the originally assumed 2.0 ml/min/1.73 m2.
RecruitmentHospital data from the past years (2020, 2021) was used to examine the potential of each of the eight medical centres to enrol eligible participants. Achieving the target sample size of n = 425 participants based on this data seemed realistic. Moreover, the study schedule included an optional time slot to extend the recruitment beyond 15 months, if necessary.
In November 2022, the first recruitment phase (of control patients) was prolonged by 5 weeks to compensate for a slow start. Because of ongoing underrecruitment especially regarding the intervention group, in October 2023, it was decided to extend the recruitment by four additional phases, 50 days each.
留言 (0)