
記住我





This is a randomized, controlled, single-center, open-label trial carried out in the ICU of the San Paolo General Hospital in Milan, Italy, which comprises three separate rooms with two or three beds each. The Ethics Committee of Milan Area 1 (Prot. 9827 of April 13, 2017) authorized the trial.
OutcomesThe main hypothesis is that both personalized and generalized MT can significantly reduce the need for neuroactive drugs in critically ill patients. We will investigate whether MT increases the number of days “free from neuroactive therapy” (analgesics, sedatives, anxiolytics, and antipsychotics) [30] in the first 28 days after ICU admission and, as secondary outcomes, whether it reduces the total of ten commonly used sedative and analgesic ICU medications (midazolam, lorazepam, propofol, dexmedetomidine, morphine, fentanyl, remifentanil, hydroxyzine, haloperidol, quetiapine). Sedative use will be measured as the daily sedative drug intensity score and dose frequency. The reduction of ICU stress will be measured using the validated ICU Environmental Stressor Scale (ICUESS) scale, which rates the perception of stressors during the whole ICU stay [31].
ConsentWritten informed consent has been gathered by the investigators from all competent patients; for temporarily non-competent ones, permission to use the personal data already collected has been granted as soon as they become competent, according to the ethics committee’s indications.
Additional consent provisions for collection and use of participant data and biological specimenNot applicable.
Eligibility criteriaAll critically ill patients were screened for enrolment as they are admitted to the ICU, according to these inclusion criteria: age > 18 years, expected mechanical ventilation > 48 h. The exclusion criteria are as follows: expected Glasgow Coma Scale < 12 at ICU discharge, hearing loss, advanced neurodegenerative dementia, any unbalanced psychiatric condition in their history, a change of bed or room during the ICU stay.
Interventions and blindingParticipants were randomly allocated to three groups, with a parallel assignment at ICU admission, applying an electronic minimization algorithm. Depending on their assigned group, they were admitted to a specific ICU room by the staff intensivist in charge at the time of ICU admission (Fig. 1).
Fig. 1
Group allocation at ICU admission
In the control group, patients could hear the background sounds (alerts, voices) of the ICU environment; listening to unspecified radio programs is allowed, according to medical/nursing judgments, as per usual local practice. Patients in the personalized MT group could listen to music chosen according to their preferences, for all time they wanted, with a minimum of 2 h per day. MT was selected from specific 30-min playlists of all the music available. They can ask for other particular tracks or types of music, if not immediately available. For comatose or deeply sedated patients, music was chosen by their relatives after an interview on the patient’s presumed preferences. The meeting with the music therapist was carried out within 24 h of randomization, and the Music Assessment Tool (MAT) was used to collect patients’ preferences, reported in the supplementary materials.
Patients allocated to the generalized MT group were admitted to a room where music was broadcast for 12.5 h per day, based on a specific “weekly playlist,” as follows. Sound was on from 07:00 to 22:00 (clock hours, see Fig. 2), with a 10-min break every 50 min of music, and silence at night, from 22:00 until 07:00 in the subsequent morning. Music was transmitted through the environment with specifically designed speakers at a controlled volume (5 dB above the ICU noise). Tracks were from both classical, modern, and so-called contemporary music (considering commercial pieces composed since the mid-twentieth century), chosen for easy listening, and selected according to the hours per day needed to restore circadian rhythm and predictable activities of care (hygiene, food, other therapies, physiotherapy, visits from relatives, etc.). Tracks were mixed to ensure continuity and fluidity of listening. The selection of music in the generalized group occurred after the music therapist had conducted a week-long participant observation period at the center’s ICU. During this observation period, the therapist was able to analyze the different phases of life on the ward to the point of defining the criteria for the choice of tracks shown in Table 1.
Fig. 2
Generalized music therapy during the clock hours. The tracks composing the playlist for the generalized MT were chosen according to the purposes shown. Every hour, there were 50 min of uninterrupted music and 10 min of silence to avoid habituation effect. From 22 to 7, the silence was used to promote physiological sleep. MT, music therapy
Table 1 Purposes of the time slots in generalized MTProvisions for post-trial careThere was no anticipated harm and compensation for trial participation, and no provision for post-trial participation was planned in the protocol.
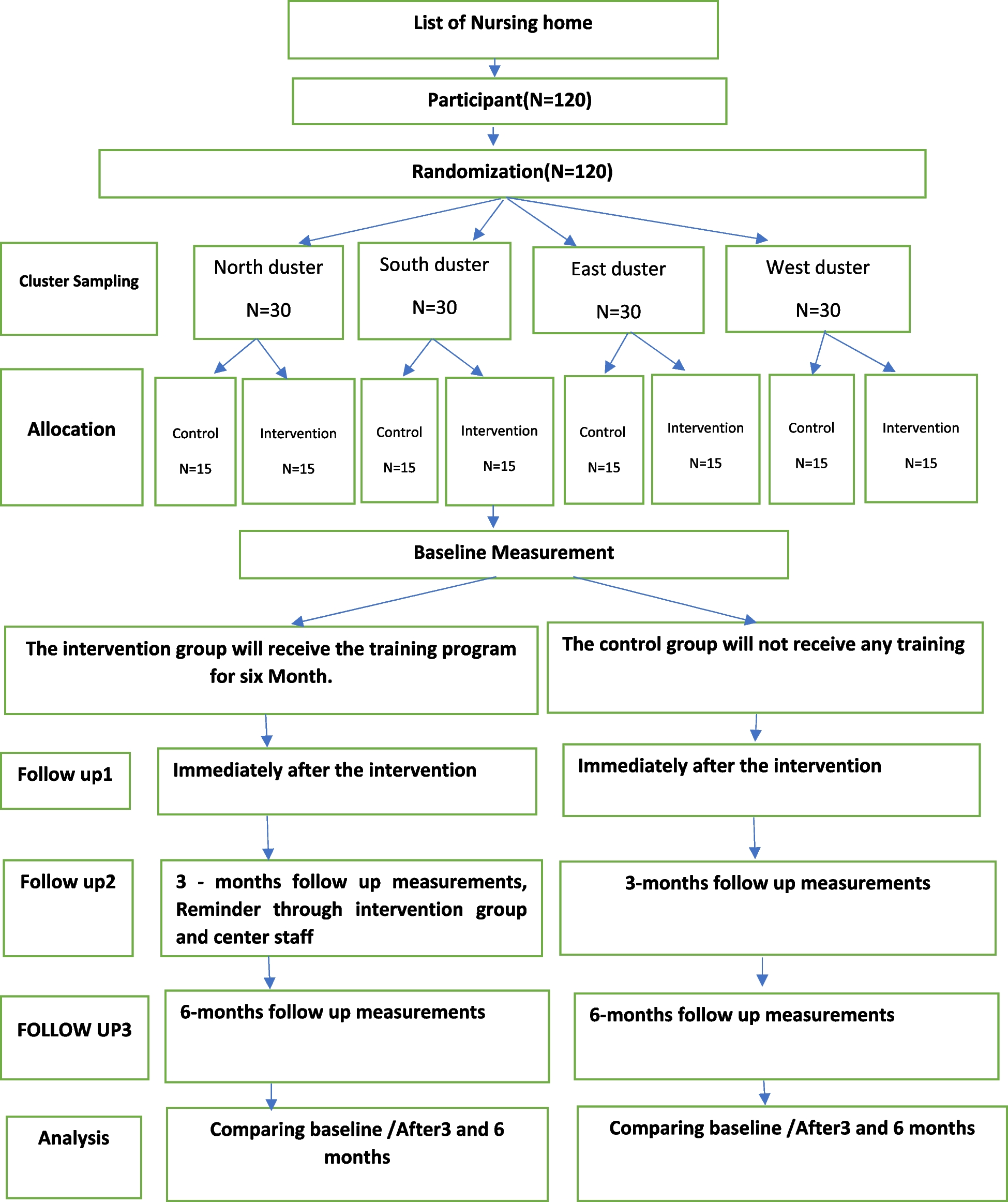
Data collection and participant timelineFor each participant, the following information was recorded: where admitted from, the reason for hospitalization, comorbidities, the Simplified Acute Physiology Score 2 (SAPS II) after 24 h in the ICU [32], the daily Sequential Organ Failure Assessment (SOFA) score [33], and Glasgow Coma Scale (GCS) [34]. At each change of nursing shift, vital signs, doses of neuroactive drugs, Behavioral Pain Scale (BPS) [35], Richmond Agitation Sedation Scale (RASS) [36], Confusion Assessment Method for the ICU (CAM-ICU) [37], use of physical restraints, and incidence of adverse events were recorded. Figure 3 depicts the overall schedule and time commitment for trial participants.
Fig. 3
SPIRIT schedule of enrolment, interventions, and assessments. The figure depicts the overall schedule and time commitment for trial participants. MT, music therapy; SOFA, Sequential Organ Failure Assessment Score; BPS, Behavioral Pain Score; RASS, Richmond Agitation-Sedation Scale; CAM, Confusion Assessment Methods; ICU, intensive care unit
In the room with generalized MT, the number of times the music was interrupted was recorded, while in the room with personalized MT, the total time the patients listened to music was recorded. On the day of ICU discharge, the Mini-Mental State Examination (MMSE) [38] was administered. If the score was higher than 24 points, the following tests were done: ICU Environmental Stressor Scale (ICUESS) [31], a Likert-type questionnaire to measure the stressfulness of commonly occurring items in the ICU, and the Short Screening Scale for Post-Traumatic Stress Symptoms (SSS-PTSS) [39], a seven-question survey to screen for the probability of a post-traumatic stress disorder.
Data were gathered daily, using values and drugs listed on the patient’s chart. Patients were assigned an ID to ensure their privacy. The ICUESS and SSS-PTSS questionnaires were recorded within 3 days from when the patient is discharged from the ICU. Finally, also, the hours of sleep have been recorded for each patient. All data collection sheets are available in Additional file 1 in the Italian version used.
Plans to promote participant retentionNot applicable as all data were gathered during hospital stay.
Plans for collection of biological specimens for genetic or molecular analysisNot applicable.
ConfidentialityAll study-related information were stored securely at the study site. All participant information were stored in locked file cabinets in areas with limited access. All records that contain names or other personal identifiers, such as locator forms and informed consent forms, were stored separately from study records identified by code number. All local databases were secured with password-protected access systems.
Personalized MTICU patients assigned to the personalized MT were screened with the Music Assessment Tool (MAT) [40] to determine their music preferences. The Italian version of MAT used is reported in Additional file 1. In case of neurological inability because of acute organic/metabolic disease or because of sedation, the MAT was completed with the help of the patients’ families. Then, the “preferred music” was transmitted for at least 2 h per day through a portable system and headphones, and patients could listen for the 2 h/per day until recovery of their neurological function. Neurologically competent patients could listen to their preferred music as long as they want.
The music therapist prepared several 30-min playlists; each patient (or his/her family) was invited to select at least four of these playlists—or to choose other genres. In this case, the music therapist prepared different playlists for the next day to meet these requests. If a patient preferred not to listen to music, s/he was not obliged, and his/her choice was recorded. Finally, also, the types of playlists and the time spent listening each day were recorded.
Generalized MTThe music tracks on the playlist for the generalized MT were chosen by a music therapist according to the characteristics presented in Table 1. For example, in the early hours of the day, we offered songs that encouraged gentle awakening, passing gradually to imaginative stimulation and encouraging the body to wake. Towards the end of the day, the rhythm slowed to encourage patients to relax and accompany them toward sleep.
Other kinds of music were intended for the total daily ICU routines (therapy, mobilization of patients, relaxation, visits from families) and to reactivate emotions (to evoke recollections and motivate the patient for complete recovery) [41].
Seven different playlists, with the duration on 15 h, were drawn up for each day of the week. Different tracks were chosen according to these rules:
Non-aggressive, simple, regular music (except for slots 4 and 6, where significantly more vigor is required)
Genres as varied and popular as possible, excluding niche music such as Gregorian chant, Neapolitan melodies, free jazz (to name just some), heavy metal, hard rock, and techno/disco numbers
Extreme variety of styles and ages. Exclusion of non-widely accepted or experimental styles
Preferably high-quality recordings and performances
Repertoire from Western culture, generally after the year 1600
Each item is selected after analyzing the phono-symbolic significance of the music while bearing in mind that it is impossible to predict what kind of synesthetic associations may be aroused in each patient since they are unique and differ widely for everyone
The songs were selected by a music therapist with 30 years of experience, mainly working in the psychiatric field, and based on dozens of interviews with people of various ages.
Additional file 1 gives a complete description of the generalized MT methods. Besides the list of rules for selecting tracks, also presented are the criteria for each time slot and the technical features used in preparing the playlists. A comprehensive list of the Italian musicology books used by the music therapist is also available in Additional file 1.
Statistical analysis and sample size calculationGiven the nature of the study, blinding was not possible for treating physicians and for investigators who collected the data. Assuming the possibility of transforming the data with the Blom method in order to obtain normal distribution and therefore higher power with the same sample size, and taking an effect size of 0.30 and doubling of the primary outcome parameter (days without needing neuroactive drugs) in the two intervention groups compared to the control group, and between the two interventions, 53 subjects per group were required for a power of 80%. This sample was also sufficient for comparing repeated measurements on the same patient. For this, a linear model will be used, which requires 51 subjects per group, assuming a 0.5 correlation coefficient between the measures and an effect size of 0.25. The power of the sample was calculated with SAS software. No interim analyses are planned. Missing data will not be imputed. The full protocol, participant-level data, and statistical code will be held by the principal investigator.
Steering committee, adverse events, and data monitoring committeeGiven the single-center nature of the study, members of the steering committee were always available on site to provide day-to-day support for the study. The steering committee has been meeting monthly to discuss the progress of the project and provide feedback to the operators involved in data collection.
The ethics committee met only at the beginning of the project but remained at the disposal of the other investigators for the duration of the protocol in case of emergence of problematic issues.
No adverse events were expected to occur given the nature of the interventions and, for this reason, no data monitoring committee was needed.
Plans for communicating important protocol amendments to relevant parties (e.g., trial participants, ethical committees)Any modifications to the protocol that could have an impact on the conduct of the study, or could have affected patient safety, including changes of study objectives, study design, patient population, sample sizes, and study procedures, would have required a formal amendment to the protocol to be approved by the ethics committee prior to implementation. However, no protocol amendments occurred during the recruitment period.
Dissemination plansThe study results will be released to the participating physicians, patients, and the general medical community.
Preliminary qualitative data: the ICU staff members’ viewpointsDuring the whole study, the comments of the healthcare staff working in the generalized MT milieu were collected. Seven weeks from the beginning of the study, physicians and nurses were asked if they found the music disturbing. They have reported that the music can be slightly distracting in the first few hours (“When we are doing some specific tasks, at the start of the new hour of music—especially if it’s known—may be distracting”) or in rare, specific conditions (“It would be better to turn off the speakers when we are doing tracheostomy or some other bedside intervention: the music, the sounds of the monitor, and us discussing things together … it’s chaotic!”). However, these comments have decreased over time, as being “immersed” in a musical atmosphere becomes a habit (“It’s nice to have these background songs, even though after a week I’ve already heard them all. It’s comforting to arrive and hear them” or “In the morning, during the nursing and attending to the patient’s hygiene, it’s very nice to have this kind of music: it would always be!”).
Many comments have been made on the choice of music—some deemed it inappropriate (“Christmas carols in the summer are silly…”) or it did not meet a patient’s musical tastes (“Hearing a rubbishy Italian song like Azzurro is not acceptable after the guitar solo of Sultans of swing: Mark Knopfler wouldn’t want it!”). Some have asked for more, different playlists (“To start with, it was a pleasant novelty, but after a while, the repetition of the tracks gets boring.”). These negative comments were reported by a minority of the staff since the wide variety of styles and tracks mainly satisfied everyone’s preferences (“I prefer to work in the generalized MT room instead of the control room because on the radio there’s so much more talk or advertising than good music.”).
Generalized music was considered better because it did not hinder clinical procedures and did not make the workload any heavier (“But isn’t it better to use loudspeakers for everyone? The headphones often come off when dressings are done, or during exercise.”). The headphones for personalized music can prove obstructive in some clinical maneuvers (e.g., mobilizing patients and physiotherapy), or they cannot be used because of particular clinical conditions (e.g., non-invasive mechanical ventilation with helmet CPAP or with some types of full-face mask, during an EEG, prone positioning, etc.).
Expected resultsSeveral studies have reported the positive effects of personalized music-based interventions [14, 16]; the present study aims to verify whether similar results can be obtained with generalized MT. The expected benefits for patients are an increase in sleep at night, reduction of anxiety and manifestations of psychomotor agitation, lower anxiety, and reduction in the frequency and duration of physical restraints.
Sleep deprivation—in quality and quantity—is widespread in the ICU, as is delirium [42]; these pathological conditions have a range of causes (Fig. 4). We hardly expected that normalization of the sleep-waking rhythm in the generalized MT group guided by a sound-full day and a silent night, with particular attention to the waking and falling asleep phases, could lower the prevalence of delirium and consequently possibly reduce the need for neuroactive drugs. Data on sleep distribution during the morning-afternoon-night phases were collected.
Fig. 4
Potential targets of music therapy. Representation of the potential targets of music therapy in the complex interactions between sleep disruption and delirium with increasingly worse outcomes in critically ill patients
留言 (0)