
記住我

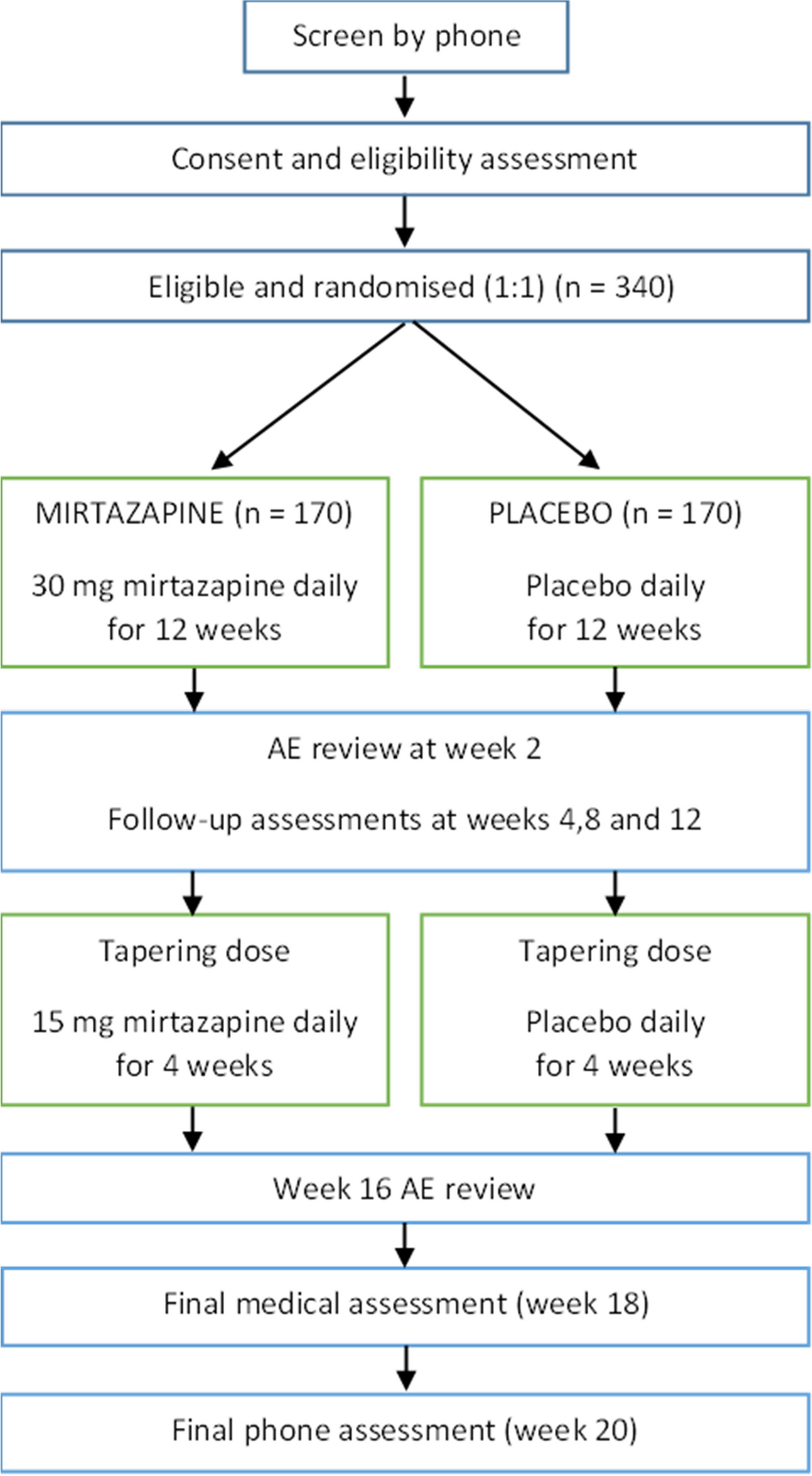




EORTC-2227-BTG (LEGATO, NCT05904119) is an investigator-initiated, pragmatic, randomized, open-label, multicenter phase III trial in patients with first progression of glioblastoma. Figure 1 summarizes the study design. Of note, the information provided reflects the protocol version 3.0 approved on 24 January 2024. Investigators must refer to the latest version of the full study protocol, which is available to study investigators in their trial files. Publicly available information and updates on the trial progress can be found at https://legato-horizon.eu.
Fig. 1
Study scheme of the EORTC-2227-BTG (LEGATO) trial
Trial populationMain eligibility criteria include age ≥18 years, written informed consent, histologic confirmation of glioblastoma, IDH wild-type per WHO 2021 classification, first progression or recurrence after first-line treatment with biopsy or maximal safe resection and standard radiotherapy or chemoradiotherapy having occurred at least 6 months after the end of prior radiotherapy, radiologically measurable disease according to RANO criteria with a maximum tumor diameter of 5 cm, WHO performance status of 0–2, and any MGMT promoter methylation status. The detailed eligibility criteria are shown in Table 2. The patients will receive extensive information about the study set-up and requirements during the recruitment by the local investigators, who are board-certified physicians with current good clinical practice (GCP) certification and confirmed delegation and completed training for clinical trial activities. The importance of completion of the follow-up will be stressed. A clinical trial insurance has been taken out according to the laws of the countries where the study will be conducted.
Table 2 Eligibility criteria for the EORTC-2227-BTG (LEGATO) trial.Objectives and endpointsThe objectives and endpoints of the LEGATO trial are detailed in Table 3. In brief, the primary efficacy endpoint is overall survival (OS) and secondary endpoints include progression-free survival (PFS), response rate, neurocognitive function, health-related quality of life, and health economic parameters.
Table 3 Objectives and endpoints of the EORTC-2227-BTG (LEGATO) trialOS is defined as the number of days from the date of enrolment to the date of death due to any cause. If a subject has not died, the data will be censored at the last date documented to be alive. PFS will be defined as the number of days from the date of enrolment to the date of earliest radiological disease progression or to the date of death due to any cause, if disease progression did not occur. Patients for whom neither death nor progression have been documented will be censored at the date of the last radiological assessment that the patient was progression-free.
Radiological follow-up for the evaluation of PFS and response rate will be performed by cranial MRI every 12 weeks. MRI will be assessed according to Response Assessment in Neuro Oncology (RANO) criteria interpretation by the local investigator.
Toxicity reporting will be done according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Neurocognitive functioning will be assessed using Mini-Mental State Examination (MMSE) every 6 weeks and the NANO scale will be utilized for evaluation of neurological function. Health-related Quality of Life (HRQoL) will be assessed every 6 weeks using EORTC Quality of Life Questionnaire (QLQ)-C30, QLQ-BN20 Brain tumor module and one additional item from the EORTC Item Library (IL)-46.
Self-reported HRQoL data will be transformed into health utility values for subsequent health economic analyses. To this end, the EORTC QLQ-C30 data collected for each study subject and at each HRQoL assessment time point will be mapped to health utility values using an established indirect mapping approach [15, 16]. In the adopted indirect mapping approach, first the probabilities of belonging to European Quality-of-Life-5 Dimensions (EQ-5D) categories will be calculated, and then the corresponding EQ-5D scores will be translated into health utility values using a country-specific value set for the conversion [16].
Tables 4, 5, and 6 summarize study calendar before treatment start, during treatment, and during follow-up. Data will be captured in electronic case report forms.
Table 4 Study calendar—before treatment startedTable 5 Study calendar—during protocol treatmentTable 6 Study calendar—follow-upStatistical considerations and data managementA total sample size of 411 patients is needed to detect an increase from an expected median OS of 9 months [17, 18] in the control arm to 12.5 months in the experimental arm based on a one-sided log-rank test at a significance level of 2.5% and a power of 80%, corresponding to a hazard ratio of 0.72. An increase of 3.5 months of survival when radiotherapy is added to lomustine would be considered clinically significant. Stratification factors will include country, MGMT promoter methylation status (unmethylated vs methylated vs unknown), steroid use at study entry (no, yes), and WHO performance status (0, > 0). There will be an interim futility and efficacy analysis organized after observation of 97 OS events (33%). The primary analysis will be performed in the intent-to-treat population (ITT), i.e., all randomized patients according to the arm they were allocated to. In the per protocol population, all randomized patients who have started their allocated treatment (i.e., at least one dose of lomustine or lomustine and radiotherapy) will be analyzed. In the per protocol population, patients will be classified and analyzed in the arm they were assigned at the time of enrolment. For data management procedures, EORTC, in its role of sponsor and data controller of the clinical study ensures that the processing activities on the personal data in scope of this study are compliant with, but not limited to, the requirements set by EU General Data Protection Regulation (GDPR EU 2016/679), its subsequent amendments and any additional national laws, recommendations, and guidelines as applicable. All data are collected via an electronic case report form by study staff with confirmed GCP certification named on delegation logs at the trial sites and are stored in secure database at EORTC Headquarter. The name of patients enrolled in the trial will neither be asked for nor recorded at the EORTC headquarters. A sequential identification number will be automatically allocated to each patient registered in the trial. This number will identify the patient and will be included on all case report forms and corresponding material and data associated with the patient. In order to avoid identification errors, the patient’s code (maximum of four alpha numerics) and year of birth will also be reported on the case report forms. Data collected during the course of the research will be kept strictly confidential and only accessed by members of the trial team (or individuals from the Sponsor organization or center sites where relevant to the trial). The EORTC headquarters will perform on-site and/or remote monitoring visits according to the approved study monitoring plan in order to maximize protocol adherence, correct false data entries, and minimize missing data. No imputation will be used to account for missing data. The first visit in a participating site will be performed within 6 to 12 months after the first patient’s enrolment at this site. Frequency and number of subsequent visits will depend on site’s accrual and quality observed during the previous visit. Reporting of adverse events indicating expectedness, seriousness, severity, and causality will be performed according to ICH GCP and EU Regulation 536/2014. At the trial sites, all reporting of adverse events must be done by the principal investigator or authorized staff member and will be transmitted electronically to the pharmacovigilance department of EORTC. As the sponsor, EORTC will be responsible for the reporting of suspected unexpected serious adverse reaction (SUSARs)/unexpected serious adverse reaction (SARs) to the competent authorities, ethics committees, EudraVigilance Clinical Trial Module (EVCTM), and all participating investigators as applicable. Medical review will be performed on a regular basis by a medical representative at EORTC and with the support of the principal investigator. Data collected during the course of the research will be kept strictly confidential and only accessed by members of the trial team (or individuals from the sponsor organization or center sites where relevant to the trial). The independent data monitoring committee for EORTC studies (IDMC) is in charge of the independent oversight of this study, according to the EORTC policies. LEGATO is an open-label trial and trial participants, care providers, outcome assessors, and data analysts will not be blinded. The clinical trial is registered at ClinicalTrials.gov with the identification number NCT05904119.
InterventionsPatients will be randomized by EORTC in a 1:1 ratio to the control arm of lomustine alone or the experimental arm of lomustine plus radiotherapy.
Control arm: lomustineIn the control arm, lomustine will be given at a recommended dose of 110 mg/m2 (maximum absolute dose 200 mg, minimum dose 80 mg) every 6 weeks. The maximum cumulative dose must not exceed 1000 mg/m2 to prevent pulmonary toxicity [19]. Participants must start lomustine within 7 days of enrolment. Treatment will be administered until disease progression, unacceptable toxicity, death, or until the occurrence of any predefined withdrawal criterion such as withdrawal of patient consent or safety concerns. Lomustine has a well-known safety profile that includes fatigue, hematological symptoms, and on rare occasions, the development of pulmonary toxicity after more than 6 months of treatment and a cumulative dose of 1000 mg/m2. Hematological toxicity, as the main concern in the treatment by lomustine occurs usually after 4 weeks after drug administration. Recommendations for dose modifications follow published guidelines [20].
Experimental arm: lomustine plus reirradiationIn the experimental arm, radiotherapy with a prescribed dose of 35 Gy (daily dose 3.5 Gy, 10 fractions) over 2 weeks will be delivered in addition to the same chemotherapy regimen as in the control arm (lomustine 110 mg/m2 every 6 weeks). Lomustine should be started within 7 days of enrolment. Radiotherapy should start within 14 days of randomization and/or within 7 days of the first lomustine intake. Megavoltage equipment able to deliver stereotactic, intensity-modulated radiotherapy (IMRT) or volumetric modulated arc therapy (VMAT) is required.
Radiotherapy delineation will be performed on a magnetic resonance (MR) image with contrast agent administration. Treatment planning using volumetric modulated arc therapy (VMAT) and image-guided radiation therapy (IGRT) is advised. IMRT or VMAT planning is allowed. Intensity-modulated radiation therapy (IMRT) and three-dimensional conformal radiotherapy are allowed.
The maximum diameter of contrast enhanced recurrent tumor allowed for inclusion in the trial is 5 cm. In case of multifocal disease, the lesions must be in proximity to one another, to be treated with a single isocenter, and the maximum cumulative tumor diameter is 5 cm.
The gross tumor volume (GTV) will be defined using the MRI images as a T1-weighted contrast enhancing lesion (contrast-enhanced CT for patients who cannot undergo MRI). In patients who undergo surgery, the GTV is defined by the post-operative resection cavity plus any residual enhancing tumor.
A clinical tumor volume (CTV) expansion of maximum 5 mm can be applied at the investigator discretion for lesions measuring less than 4 cm in maximum diameter or for new lesions. CTV is cropped out around natural fixed barriers for tumor spread (skull, falx, tentorium). Otherwise, no additional CTV expansion will be added.
An appropriate planning target volume (PTV) expansion, justified based on image guidance and immobilization, will be applied. Regardless, the PTV expansion should be no smaller than 2 mm. Daily image-guided radiation therapy (IGRT) is required for institutions utilizing PTV margins of less than 5 mm.
Normal tissue limits will be defined according to the ESTRO-EORTC consensus on reirradiation, reflecting possible overlap with previous radiation target or critical organs at risk with concern of toxicity from cumulative doses [21].
The main toxicity expected from re-irradiation is radionecrosis in less than 10% of cases. The increased, synergistic, risk of hematological toxicity in the combination of lomustine and reirradiation is expected to be minimal.
Study intervention complianceA record of the number of tablets dispensed to and taken by each patient will be maintained and reconciled with study intervention and compliance records. Intervention start and stop dates, including dates for intervention delays and/or dose reductions will also be recorded in the electronic case report forms.
Supportive care and concomitant medicationsSupportive care is left at the investigator’s discretion, but adherence to the EANO recommendations is advised [20].
Prohibited medications include live or attenuated vaccines at any time during the study and for a period of 3 months after treatment discontinuation. Yellow fever vaccine is strictly contraindicated because of the risk of fatal systemic vaccinal disease. Patients must not receive salicylates due to increased risk of bleeding in case of thrombocytopenia. Any concomitant systemic therapy intended for the treatment of cancer, whether health authority-approved or experimental, is prohibited.
Permitted medications considered necessary for a participant’s welfare according to the local investigator include growth factors in accordance with ASCO guidelines for secondary prophylaxis and steroids as anti-emetics or part of symptom management [22].
SPIRIT reporting guidelines for publication of clinical trials protocols [23] were used and were submitted as an additional file (see Additional file 1).
Study governance and trial sitesThe EORTC is the legal sponsor of the LEGATO trial. The Study Management Group (SMG) consists of the EORTC Headquarters team in charge of running the study (clinical research physician, statistician, clinical scientist, project manager, and data managers) and the principal study coordinators. The EORTC headquarter team is responsible for the day-to-day conduct of the trial. The study coordinator will assist the team in case of problems with patient evaluation (eligibility, treatment compliance, safety). The SMG also performs the medical review. The Study Steering Committee (SSC) for this study is composed at of the study coordinators and two representatives (clinical scientist and statistician) of the EORTC headquarters (study clinical research physician or clinical scientist or statistician). This committee provides the general oversight of the study and has executive power. The SSC monitors study progress and conduct and advises on its scientific credibility. The SSC will consider and act, as appropriate, upon the recommendations of the Independent Data Monitoring Committee. There is a patient representative in the protocol writing committee, which is composed of a total of 13 persons from various disciplines. LEGATO was activated in March 2024 and will enroll patients in 43 sites in 11 countries across Europe including Austria, Belgium, Czech Republic, Denmark, France, Germany, Italy, Norway, Spain, Switzerland, and The Netherlands. Information on the LEGATO trial network can be found at https://www.clinicaltrials.gov/study/NCT05904119 and https://legato-horizon.eu.
留言 (0)