As was previously indicated, advancements in ART alongside heightened awareness have led to a rising trend of infertile patients with pSS seeking ART interventions. However, concerns have escalated regarding the negative effects of pSS antibody on the pregnancy process and the newborn [3]. In addition, few studies have explored the prevalence of pSS in infertile women and the exact impact of pSS on female fertility and its downstream effects. There are also no studies that examine whether women with pSS irreversibly impaire oocyte and embryonic development potential. In the current study, we comprehensively assessed the effect of pSS on oocyte and embryo competence, ovarian reserve, clinical and obstetric outcomes. The results of present study showed that in comparison to women with common infertility, women with diagnosed pSS or a history of pSS had compromised oocyte and embryo viability and lower ovarian reserve, thus resulting in poorer IVF clinical outcomes. We provided a new perspective on fertility assessment in pSS patients in terms of evident observation of oocyte and embryo development.
For one thing, the ovarian function was observed a significantly diminished in pSS patients compared to comparison. Patients with pSS not only exhibited lower AMH levels and AFC counts, but also had a much higher incidence of DOR and POR than comparison. This was in line with the results of a cohort study of a Turkey population, which found the ovarian reserve may be reduced in pSS patients [10]. And some prior studies reported that patients with pSS experienced early menopause or menstrual abnormality more frequently than the general population, which can also be a sign of declined ovarian function [19, 20]. In fact, prior investigations have reported the impact of autoimmune disorders, notably systemic lupus erythematosus (SLE), on female reproductive health, including ovarian reserve impairment and heightened susceptibility to premature ovarian failure [21, 22]. However, in contrast to the extensive scrutiny afforded to SLE in the context of female fertility, the studies concerning pSS remains notably limited. Therefore, this study could provide a valuable supplementary, especially as more and more pSS patients are choosing for ART.
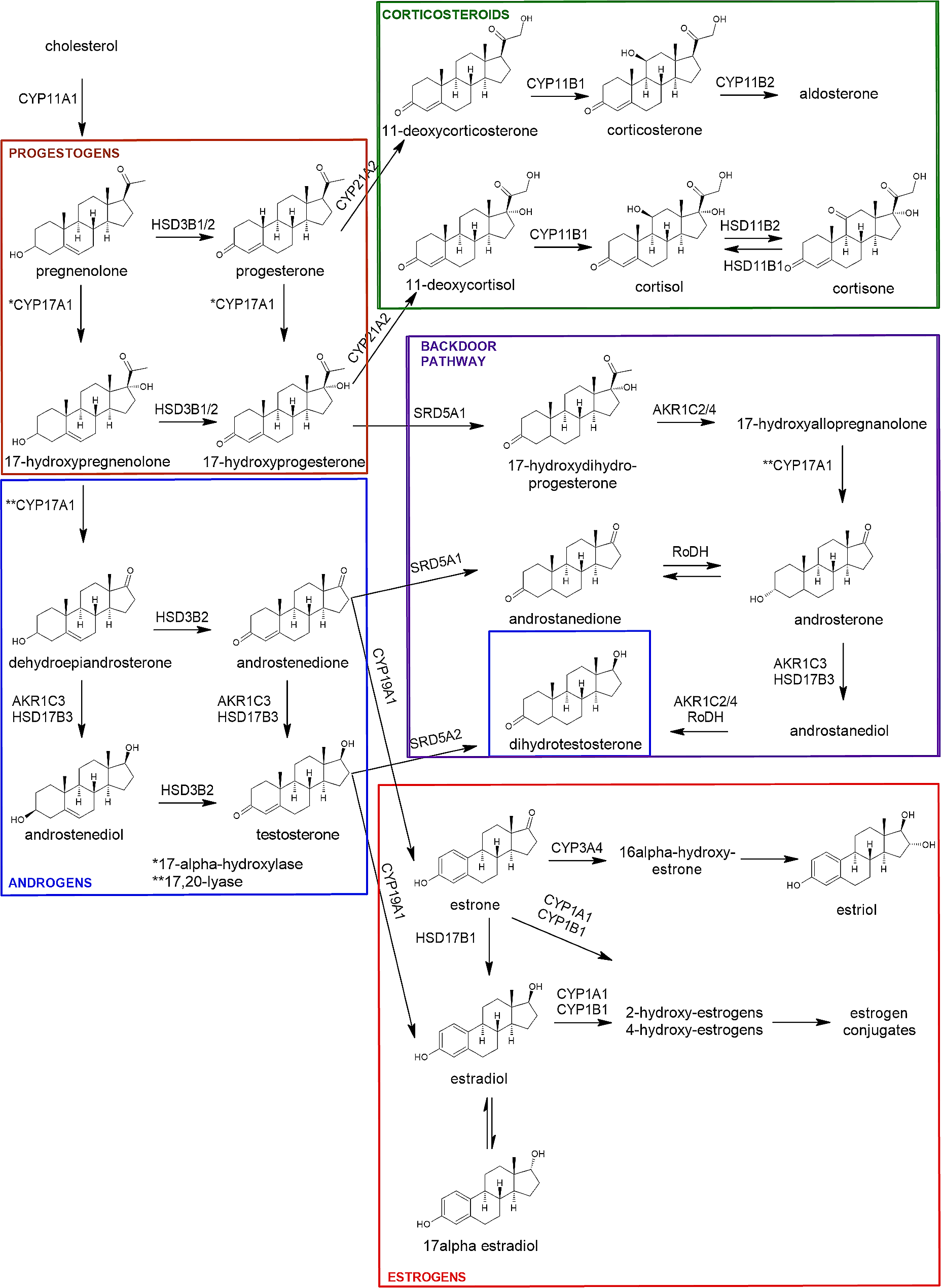
Secondly, as with most autoimmune diseases, environmental and hormonal are implicated in the pathogenesis of pSS. Cumulative evidence suggested low estrogen levels, and localized dihydrotestosterone deficiency appeared to be more prone to pSS [25, 26]. Increasing estrogen exposure could be negatively related with risk of pSS [27]. Our findings also showed a significantly lower E2 level in pSS group even after controlled ovarian hyperstimulation. Of concern is that studies revealed that pSS could be associated with dysfunction of hypothalamic–pituitary–adrenal (HPA) axis and thyroid axes. Distinctly lower basal adrenocorticotropin (ACTH) and cortisol levels were found in patients with pSS [28]. Not only that, but serum prolactin levels may also be elevated in patients with pSS, which are widely considered to be associated with female infertility [29, 30]. Hence, in instances where patients diagnosed with pSS present with the above clinical attributes, it is essential for them to undergo comprehensive assessment by interdisciplinary teams comprising rheumatologists and reproductive specialists. This collaborative approach will facilitate the formulation of tailored treatment strategies aimed at optimizing early fertility outcomes.
In terms of oocyte and embryonic development in patients with pSS, the present study provided valuable insights that have not yet been focused on in previous studies. It is worth mentioning that our results also showed that pSS patients exhibited worse oocyte and embryonic development in terms of oocytes retrieval, maturation, embryo cleavage and blastocyst formation. The potential mechanisms for this could be multifaceted and complex. Primary Sjogren's syndrome is a chronic autoimmune disease with abnormal immunity activation. Over-activated immune cells and a variety of auto-antibodies may play an important role in the process [23, 24], but research is needed to further elucidate. For patients with pSS undergoing ART, the compromised development of oocytes and embryos typically translates to suboptimal treatment outcomes, but so far there has not been widespread concern about the outcome of ART in such patients, and thus there is still no consensus on subsequent interventions strategies. Nonetheless, we still advocate early involvement of rheumatologists and reproductive specialists in the evaluation and management of infertility in patients diagnosed with pSS, taking into account the patient's ovarian reserve function and the development of oocyte and embryos, and integrating a combination of pSS treatment and ART to closely monitor the development of oocytes and embryos in order to achieve the best therapeutic outcome. It's worth noting that our results showed that even pSS was in a remission period, patients still had impaired oocyte and embryo development and poor clinical outcomes. Therefore, any patient with pSS who intended to undergo ART should implement so as soon as possible after evaluation of the disease and try not to let age be a second barrier to fertility.
Additionally, our previous work found that SLE patients also exhibit oocyte and embryonic developmental abnormalities [31], which may imply some commonalities between autoimmune diseases.Delving deeper into the potential mechanisms may enrich our understanding of their complex relationship.In relation to the clinical pregnancy, our study provides a more comprehensive assessment of clinical outcomes, and our results show that even when more embryos are transferred on average, the rates of implantation, LBR per complete cycle, and LBR per transfer are distinctly decreased in pSS patients than in comparison patients. Actually, similar to our findings, a case–control study by Priori et al. reported that the average number of pregnancies in pSS patients were quite lower than normal patients [32]. However, it should be noted that some previous works differ from our results. As early as 1994, a study by Fotini et al. found that the viable infant rate between pSS patients and control were comparable [33]. This conclusion was in line in another study in Denmark, which reported that pregnancy and live births between pSS patients and controls were generally similar [34]. But what has to be mentioned is that above previous studies assessed the pregnancy outcomes of pSS patients included pregnancies before and after diagnosis, representing a possible bias [11, 12, 32,33,34], whereas our studies only included patients after diagnosis of pSS. It's reasonable to speculate that pSS may exert a relatively small effect on patient with pre-diagnostic pregnancy, which have been confirmed in some subgroup studies. Priori et al. reported that the average pregnancies per woman with the diagnosis of pSS was only 1.27, which was less than the women prior to the diagnosis of pSS, which was two. Moreover, several studies included patients who were menopausal women, and related information may be obtained through questionnaires or oral surveys tracing childbearing history at a young age [11, 33, 34], which has a great potential for bias. In addition, some retrospective studies have simply reported pregnancy rates and live births in patients with pSS without control group [35]. Therefore, conclusions in many previous studies were doubtful due to various bias, while our study offered relatively objective evidence by enrolling clinical diagnosed pSS patients from different hospitals, with propensity score matched analysis and visualized oocyte and embryo manifestation, and further showing impaired CLBR and implantation condition of pSS patients, so we have more reason to believe that the pSS patients did suffer from deteriorated pregnancy outcomes.
Furthermore, the impact of pSS on fertility outcomes may not be limited to pregnancy outcomes. Women with pSS could experience amenorrhea or menstrual disorders significantly more often than normal women [19]. And not only that, but studies reported that pSS mothers may experience a delayed pregnancy, which means giving birth at an older age than normal ones [9], this in turn leads to a decline in ovarian reserve, and further make it increasingly difficult for them to conceive. Hence, we still emphasize the need for a combination of pSS treatments, a comprehensive fertility evaluation, and ART treatments for a comprehensive range of therapeutic options. Additionally, many prior studies reported that pSS may be associated with preterm birth, low birthweight and neonatal defects especially neonatal heart block [34, 36, 37]. A substantial correlation between congenital heart block and anti-Ro/SS-A and anti-La/SS-B have been demonstrated in previous studies [38,39,40]. A meta-analysis of nine studies suggested that SS was highly associated with preterm birth (RR = 2.27, 95% CI 1.46‒3.52) and low birth mass (RR = 1.99, 95% CI 1.34‒2.97) [37], and this conclusions were also similar to our results. Additionally, a literature review including seven studies by Sara et al. showed that pSS patients could accompanied with distinct increases of spontaneous abortions, preterm deliveries and cesarean section [12], and presented that pSS was responsible for adverse clinical outcomes. It's worth noting that a newborn in our pSS group performed one degree of conduction block and the maternal SSA antibody titer was as high as 1:1000 during pregnancy, which gives us more alert in providing pregnancy instruction in pSS patients with high SSA antibody titer. Although the other neonatal outcomes were essentially similar to the normal group, due to sample size limitations, more large-scale evidence and follow-up also need to be conducted in future studies.
Strength and limitationStrength:
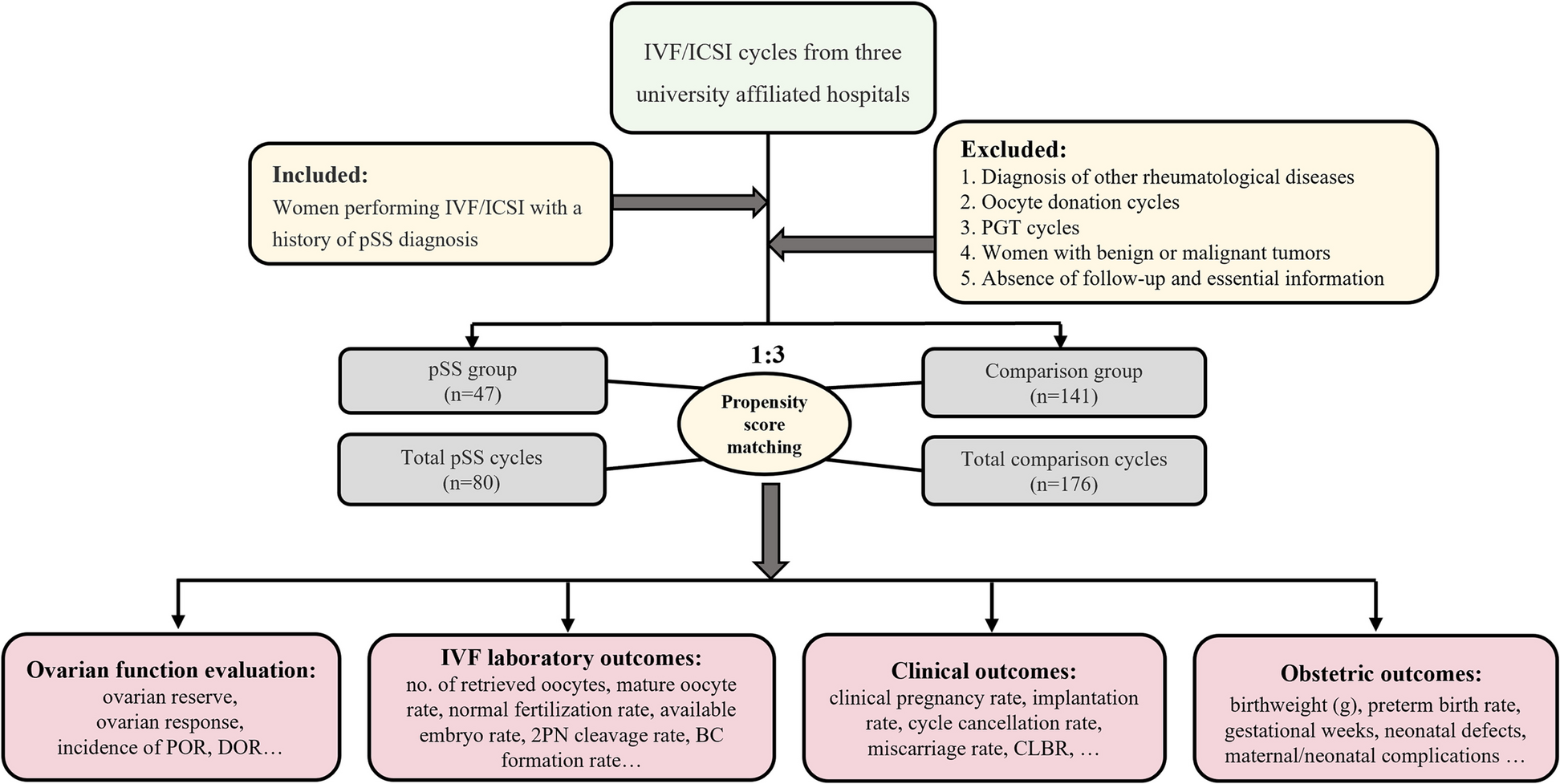
The present study first provided a new perspective on the impact of pSS on female fertility in terms of oocyte and embryo viability, while prior researchers had usually concentrated on obstetric and fetal complications of pSS. Meanwhile, the study also took the ovarian reserve and clinical pregnancy outcomes of pSS patients into consideration, which was a comprehensive analysis of the impact of pSS on female fertility. In addition, this study combined data from several hospitals, and the corresponding comparison group excluded possible interferences such as a history of endometriosis, PCOS, and ovarian surgery by PSM matching. Lastly, both conservative and optimistic CLBRs were calculated to exhibit the ART outcomes that patients were most concerned about.
Limitation:
This study also has several certain limitations. Firstly, it’s a retrospective study, which is always relevant to an inevitable risk of bias. Secondly, two patients had been treated with methotrexate therapy, which may also potentially affect their ovarian function. Lastly, due to its special population selection, the sample size of this study is not quite large.



留言 (0)