
記住我


Emerging data have shown that abnormal lipid homeostasis may contribute to the pathogenesis of hepatic inflammation and liver fibrosis.1,2 Hyperlipidemia is associated with intrahepatic fat accumulation, which can trigger the progression of liver fibrosis through an increase in oxidative stress.3 Meanwhile, intrahepatic fat accumulation has been shown to induce hepatocyte apoptosis and macrophage recruitment, which contribute to hepatic inflammation and fibrosis.4 Because hyperlipidemia is common in patients with chronic liver disease, it would be interesting to study whether lipid-lowering agents play a therapeutic role in patients with liver fibrosis.
Plasma cholesterol circulates as a constituent of lipoprotein, and hypercholesterolemia is characterized by elevated levels of low-density lipoprotein (LDL). An elevated plasma level of LDL has been associated with atherosclerosis, which in turn is associated with a higher incidence of coronary and cerebral vascular events. In addition, oxidized LDL (ox-LDL) has been associated with atheroma rupture and ischemic heart disorder.5 Apart from coronary and cerebral vasculature, ox-LDL has also been associated with portal inflammation and fibrosis in nonalcoholic fatty liver disease.1 Moreover, ox-LDL has been found in Kupffer cells, hepatic stellate cells, macrophages, and liver endothelial cells.6 Emerging data have shown that ox-LDL can exacerbate hepatic inflammation and liver fibrosis, and lysosomal lipid accumulation in blood-derived macrophages was also shown to trigger ox-LDL-dependent hepatic inflammation in a nonalcoholic steatohepatitis murine model.7 In addition, plasma levels of ox-LDL have been reported to be significantly higher in chronic hepatitis C patients than in normal controls, and to be strongly correlated with viral load, grade of inflammation, and cirrhotic status.8
Ezetimibe is a lipid-lowering agent which exerts anti-inflammation and anti-oxidant effects in addition to lipid-lowering effects.9 Ezetimibe can inhibit cholesterol absorption by targeting Niemann-Pick C1-like 1 protein (NPC1L1), which is related to intestinal cholesterol absorption. In addition to blocking intestinal cholesterol absorption, a previous study demonstrated that hepatic NPC1L1 could exacerbate steatohepatitis, and that this effect could be rescued by ezetimibe.10 The study also found that hepatic NPC1L1 is a cholesterol re-absorber from bile to the liver, which can aggravate fat accumulations in the liver.10 Taken together, we hypothesized that ezetimibe treatment may decrease ox-LDL levels, attenuate oxidative stress, ameliorate intrahepatic fat accumulation, and consequently alleviate portal hypertension and liver fibrosis in rats with chronic liver inflammation and cirrhosis.
2. METHODS 2.1. Animal model for biliary cirrhosis with portal hypertensionMale Sprague-Dawley rats weighing 280 to 320 g at the time of surgery were used for the experiments. The rats were housed in cages and allowed free access to food and water. Secondary biliary cirrhosis and portal hypertension were induced by common bile duct ligation (BDL) under anesthesia with Zoletil (50 mg/kg intramuscularly).11 A high yield of secondary biliary cirrhosis was noted 4 weeks after the ligation.12 To avoid coagulation defects, the BDL rats received weekly vitamin K injections (50 μg/kg intramuscularly). Rats in the control group received sham operation without common BDL.
2.2. Study protocolOne day before BDL or sham operation, the rats were randomly divided into three groups to receive oral gavage of the following agents: (1) Sham-operated rats, normal saline (2 mL) (Sham + vehicle, SV group); (2) BDL rats, normal saline (BDL + vehicle, BV group); (3) BDL rats, ezetimibe (10 mg/kg/d) (BDL + Ezetimibe, BE group). Survival and body weight (BW) were monitored. After 4 weeks of treatment, hemodynamic data were measured. Blood was withdrawn to measure tumor necrosis factor α (TNF-α), creatinine, total cholesterol, triglycerides, high-density lipoprotein (HDL), LDL, ox-LDL, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin levels at the end of the experiments. Hepatic protein expressions were also determined. Systemic lipid peroxidation was assayed by measuring thiobarbituric acid reactive substances (TBARS). Liver histology, intrahepatic fat accumulation, ox-LDL, and fibrosis were evaluated.
2.3. Measurement of systemic and portal hemodynamicsRight femoral arteries and mesenteric veins were cannulated with PE-50 catheters connected to a Spectramed DTX transducer (Spectramed Inc., Oxnard, CA) to record mean arterial pressure (MAP), heart rate, and portal pressure (PP) on a multi-channel recorder (model RS 3400, Gould Inc., Cupertino, CA). Cardiac output was measured using a thermodilution method as previously described.13 Cardiac index (CI) was calculated as cardiac output per 100 g BW. Systemic vascular resistance was calculated as MAP divided by CI. Superior mesentery arterial resistance was calculated as (MAP-PP)/superior mesentery artery flow (SMAf) per 100 g BW.
2.4. Portal venous flow and superior mesenteric artery flow measurementMeasurements of portal venous flow and superior mesenteric artery flow (SMAf) were performed using a nonconstrictive perivascular ultrasonic transit-time flow probe (lRB, 1-mm diameter; Transonic Systems, Ithaca, NY).14
2.5. Hepatic hematoxylin and eosin, Oil red, and Sirius red stainingThe livers were fixed in 10% formalin, embedded in paraffin, sectioned at 5 μm, and stained with hematoxylin-eosin to evaluate histological changes. Liver paraffin sections were stained using Sirius red and Oil red kits (Polysciences Inc., Warrington, PA) to determine liver fibrosis and intrahepatic fat accumulation, respectively.
2.6. Immunohistochemical staining study for intrahepatic ox-LDLThe presence of ox-LDL in the paraffin-embedded liver tissue sections was evaluated using immunohistochemical staining. The sections were incubated with primary antibodies against ox-LDL (1:400; MyBioSource, MBS620958, Vancouver, British Columbia, Canada) for 18 to 24 hours at 4°C. Signals were detected and visualized using an EnVision Detection System (Dako, K5007, Copenhagen, Denmark).
2.7. Determination of plasma TNF-α levelsPlasma samples were centrifuged at 3000 rpm for 10 minutes at 4°C and stored at −80°C until being tested. Plasma TNF-α levels were measured using a commercially available solid-phase sandwich enzyme-linked immunosorbent assay (rat TNF- kits; R&D Systems, Minneapolis, MN).
2.8. Determination of oxidative stress and lipid peroxidationOxidative stress was evaluated according to TBARS activity in the blood as previously described.15 TBARS values were calculated with the extinction coefficients of malondialdehyde (MDA) to be 1.56 × 105/M/cm and then expressed as U/mg protein in the serum.
2.9. Determination of plasma ox-LDL levelsPlasma samples were centrifuged at 3000 rpm for 10 minutes at 4°C and stored at −80°C until being tested. Plasma ox-LDL levels were measured using a commercially available solid-phase sandwich enzyme-linked immunosorbent assay (rat Ox-LDL ELISA Kit; Elabscience®, Taipei, Taiwan).
2.10. Western blot analysisLiver tissues were frozen in liquid nitrogen and stored at −80°C until Western blot analysis. Blots were incubated with the primary antibodies (nuclear factor of kappa light polypeptide gene enhancer in B-cells inhibitor α [IkBα] [1:1000, Cell Signaling 4814S; Danvers, MA, USA], cyclooxygenase 1 [COX-1] [1:2000, Cell Signaling 4841S; USA], cyclooxygenase 2 [COX2] [1:1000, Cell Signaling 12282S; USA], lectin-like ox-LDL rececptor-1 [LOX-1] [1:3000, GeneTex GTX 59636; USA], NPC1L1 [1:1000, GeneTex GTX30599; USA], beta-actin [1:5000, GeneTex Gtx629630; Irvine, CA, USA]), and then the blots were incubated with secondary antibodies (horseradish peroxidase-conjugated goat anti-mouse IgG antibody; Sigma Chemical Co., St. Louis, MO). Specific proteins were detected by enhanced chemiluminescence (Immobilon Western Chemiluminescent HRP Substrate; Merk Millipore Co., Billerica, MA) and scanned with a computer-assisted video densitometer and digitalization system (BioSpectrum® 600 Imaging System; Ultra-Violet Products Ltd., Upland, CA). Signal intensity (integral volume) of the appropriate band was then analyzed.
2.11. DrugsEzetimibe was purchased from MSD International GmbH, Belgium. All drugs and solutions were freshly prepared on the days of experiments.
2.12. Statistical analysisResults were expressed as mean ± SD. Statistical analyses were performed using an unpaired Student’s t test between SV and BV, and BV and BE groups, respectively. Survival curve analysis was performed using the log-rank test between the BV and BE groups. Results were considered statistically significant at p < 0.05.
3. RESULTS 3.1. Mortality rateThere was no significant difference in mortality rate between the ezetimibe- and vehicle-treated BDL rats (survival rate: BV vs BE, 27% [3/11] vs 20% [2/10], p > 0.05). All of the sham-operated rats survived throughout the 4-week treatment period.
3.2. BW and hemodynamic parametersTable 1 shows the BW and hemodynamic parameters of the sham-operated and BDL rats with or without ezetimibe treatment. Compared to the sham-operated rats, the BDL rats presented with significantly lower BW, higher PP and CI, and lower systemic vascular resistance. There were no significant differences in MAP, heart rate, portal venous flow, SMAf, and superior mesentery arterial resistance between the sham-operated and BDL rats. Ezetimibe treatment did not affect hemodynamic parameters in the BDL rats as compared to the sham-operated rats.
Table 1 - Hemodynamic parameters of the sham-operated and BDL rats treated with vehicle or ezetimibe Sham + vehicleBDL = bile duct ligation; BW after = body weight after 28 days of treatment; BW before = body weight before operation; CI = cardiac index; HR = heart rate; MAP = mean arterial pressure; PP = portal pressure; PVf = portal venous flow; SMAf = superior mesentery arterial flow; SMAR = superior mesentery arterial resistance; SVR = systemic vascular resistance.
aSham + vehicle vs BDL + vehicle, p < 0.05.
Table 2 shows the biochemistry parameters of the sham-operated and BDL rats with or without ezetimibe treatment. Compared to the sham-operated rats, the BDL rats had higher plasma levels of total cholesterol, triglycerides, LDL, ALT, AST, and total bilirubin. Ezetimibe did not influence liver biochemistry, lipid profiles, or renal function in the BDL rats.
Table 2 - Biochemistry parameters of the sham-operated and BDL rats treated with vehicle or ezetimibe Sham + vehicleALT = alanine aminotransferase; AST = aspartate aminotransferase; BDL = bile duct ligation; Cr = creatinine; HDL = high-density lipoprotein; LDL = low-density lipoprotein; TB = total bilirubin; TC = total cholesterol; TG = triglyceride.
aSham + vehicle vs BDL + vehicle, p < 0.05.
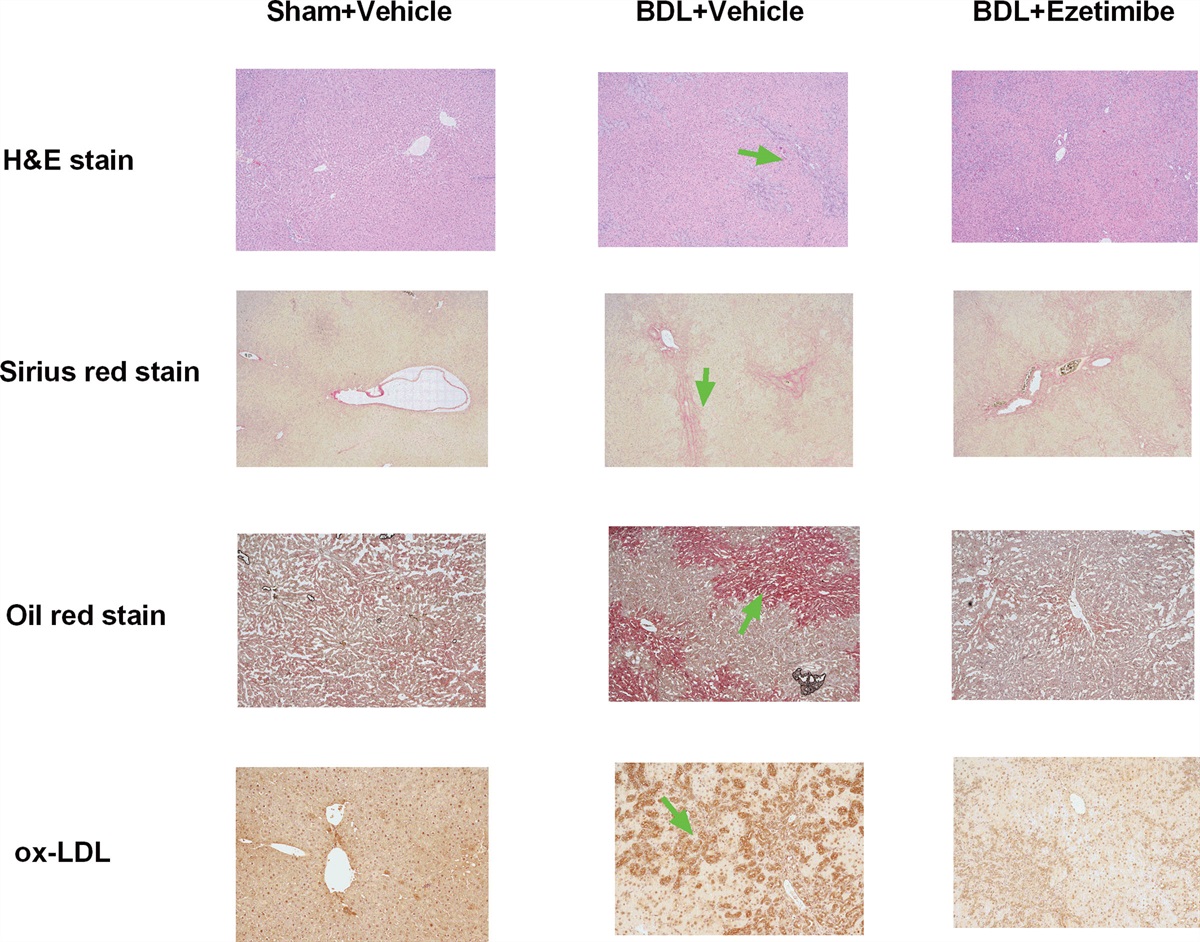
Fig. 1 shows representative images of liver histology and immunohistochemical staining in the sham-operated and BDL rats. The hepatic histology of the sham-operated rats showed normal architecture of liver tissue. In contrast, the livers of the BDL rats showed bile duct proliferation and inflammatory cell accumulation. Ezetimibe treatment did not improve intrahepatic inflammation in the BDL rats. Sirius red staining revealed obvious fibrosis in the livers of the BDL rats compared to the sham-operated rats, which was not attenuated by ezetimibe treatment. However, the BDL rats had significant increases in Oil red staining and ox-LDL-positive stained cells in the liver compared to the sham-operated rats, both of which were diminished by ezetimibe treatment.
 Fig. 1:
Fig. 1: Liver histology and immunohistochemical staining of the sham-operated and BDL rats. Representative H&E staining image of a sham-operated rat showing normal architecture of liver tissue. In contrast, many inflammatory cells and bile duct proliferation were observed in the livers of BDL rats (green arrow, magnification 40×). Ezetimibe treatment did not abolish intrahepatic inflammation in the BDL rats. Sirius red staining revealed obvious liver fibrosis (green arrow) in the BDL rats compared to the sham-operated rats, which was not attenuated by ezetimibe (magnification 40×). In addition, the BDL rats had significant Oil red staining in the liver compared to the sham-operated rats (green arrow, magnification 40×). Ezetimibe significantly attenuated the Oil red staining, indicating a decrease in intrahepatic steatosis. The immunohistochemical staining of the liver revealed many ox-LDL-positive stained cells (green arrow) in the livers of the BDL rats, which was also diminished by ezetimibe treatment (magnification 100×). BDL = bile duct ligation; ox-LDL = oxidized low-density lipoprotein.
3.5. Plasma levels of TNF-αFig. 2 shows the plasma levels of TNF-α in the sham-operated and BDL rats with or without ezetimibe treatment (SV vs BV vs BE: n = 6:8:8). The plasma levels of TNF-α significantly increased in the BDL rats compared to the sham-operated rats, and this effect was significantly decreased by ezetimibe treatment (SV vs BV vs BE: 10.0 ± 4.1 vs 18.7 ± 4.4 vs 13.9 ± 4.1 pg/mL; BV vs SV, p = 0.004; BV vs BE, p = 0.031).
 Fig. 2:
Fig. 2: The plasma levels of TNF-α in the sham-operated and BDL rats. The plasma level of TNF-α significantly increased in the BDL rats compared to the sham-operated rats, and this effect was reduced by ezetimibe treatment. BDL = bile duct ligation; TNF-α = tumor necrosis factor α.
3.6. Effects of ezetimibe treatment on systemic oxidative stressFig. 3 shows the oxidative stress markers (TBARS) in the sham-operated and BDL rats treated with vehicle or ezetimibe (SV vs BV vs BE: n = 6:8:8). Upregulation of TBARS activity was noted in the BDL rats compared to the sham-operated rats (SV vs BV: 21.0 ± 7.9 vs 76.5 ± 8.7 nmole MDA eq/mL serum, p < 0.001). Ezetimibe treatment significantly reduced TBARS activity (BV vs BE: 76.5 ± 8.7 vs 58.5 ± 9.5 nmole MDA eq/mL serum, p < 0.001).
 Fig. 3:
Fig. 3: Systemic oxidative stress parameter in the sham-operated and BDL rats treated with vehicle or ezetimibe. Upregulation of the oxidative stress marker TBARS activity was noted in the BDL rats compared to the sham-operated rats. Ezetimibe significantly reduced serum TBARS activity in the BDL rats. BDL = bile duct ligation; TBARS = thiobarbituric acid reactive substances.
3.7. Plasma levels of ox-LDLFig. 4 shows the plasma levels of ox-LDL in the sham-operated and BDL rats treated with vehicle or ezetimibe (SV vs BV vs BE: n = 6:8:8). A higher ox-LDL plasma level was noted in the BDL rats compared to the sham-operated rats, and this effect was reduced by ezetimibe treatment (SV vs BV vs BE: 7.2 ± 4.0 vs 20.4 ± 3.9 vs 15.7 ± 3.4 ng/mL; BV vs SV, p < 0.001; BV vs BE, p = 0.023).
 Fig. 4:
Fig. 4: Plasma levels of ox-LDL in the sham-operated and BDL rats treated with vehicle or ezetimibe. A higher ox-LDL plasma level was noted in the BDL rats compared to the sham rats. Ezetimibe significantly reduced the plasma level of ox-LDL in the BDL rats. BDL = bile duct ligation; ox-LDL = oxidized low-density lipoprotein.
3.8. Hepatic protein expressionsFig. 5 shows the hepatic protein expressions in the sham-operated or BDL rats treated with vehicle or ezetimibe (SV vs BV vs BE: n = 6:8:8). COX-1, LOX-1, and NPC1L1 protein expressions were significantly downregulated and IκBα and COX-2 were significantly upregulated in the BDL rats compared to the sham-operated rats (SV vs BV: COX-1/β-actin = 0.59 ± 0.21 vs 0.39 ± 0.30; LOX-1/β-actin = 0.78 ± 0.17 vs 0.12 ± 0.06; NPC1L1/β-actin = 0.70 ± 0.43 vs 0.37 ± 0.28; IκB/β-actin = 0.44 ± 0.11 vs 0.57 ± 0.16; COX-2/β-actin = 0.26 ± 0.06 vs 0.41 ± 0.25; all p < 0.05). IkBα, COX-1, COX-2, and NPC1L1 protein expressions were not significantly influenced by ezetimibe treatment in the BDL rats (BV vs BE: IκBα/β-actin = 0.57 ± 0.16 vs 0.69 ± 0.13; COX-1/β-actin = 0.39 ± 0.30 vs 0.50 ± 0.17; COX-2/β-actin = 0.41 ± 0.25 vs 0.61 ± 0.25; NPC1L1/β-actin = 0.37 ± 0.28 vs 0.49 ± 0.17; all p > 0.05). However, LOX-1 protein expression was upregulated after ezetimibe treatment in the BDL rats (BV vs BE: LOX-1/β-actin = 0.12 ± 0.06 vs 0.28 ± 0.19; p = 0.009).
 Fig. 5:
Fig. 5: Hepatic protein expressions of the sham-operated and BDL rats treated with vehicle or ezetimibe. COX-1, LOX-1, and NPC1L1 protein expressions were significantly downregulated and IkBα and COX-2 protein expressions were significantly upregulated in the BDL rats compared to the sham-operated rats. Ezetimibe upregulated the LOX-1 protein expression in the BDL rats. IkBα, COX-1, COX-2, and NPC1L1 protein expressions were not significantly influenced by ezetimibe treatment in the BDL rats. BDL = bile duct ligation; COX-1 = Cyclooxygenase 1; IkBα = nuclear factor of kappa light polypeptide gene enhancer in B-cells inhibitor α; NPC1L1 = Niemann-Pick C1-like 1; ox-LDL = oxidized low-density lipoprotein.
4. DISCUSSIONIn the present study, we investigated the effects of ezetimibe on biliary cirrhotic rats. Our data showed that the biliary cirrhotic rats had typical features of liver cirrhosis with portal hypertension and hyperdynamic circulation. The biliary cirrhotic rats also had hyperlipidemia and increased oxidative stress, which is consistent with previous reports.16 We found that 4 weeks of ezetimibe treatment did not ameliorate hyperlipidemia, however, it significantly reduced oxidative stress and ox-LDL levels. In addition, the plasma level of TNF-α was also significantly reduced after treatment, indicating the anti-inflammatory and anti-oxidative effects of ezetimibe in cirrhotic rats. In addition, ezetimibe had an acceptable safety profile with no adverse effects on liver biochemistry or mortality in the cirrhotic rats.
A previous study showed that ezetimibe ameliorated hepatic steatosis in obese and diabetic rats.17 Another report showed that ezetimibe impaired intestinal cholesterol oxidation product intake and reduced intrahepatic fat accumulation through its anti-oxidative effect.18 Despite this evidence regarding the lipid-lowering effect of ezetimibe, a contradictory study reported that ezetimibe did not significantly reduce liver fat as assessed by magnetic resonance imaging in patients with nonalcoholic steatohepatitis.19 Our results showed that ezetimibe treatment did not affect plasma lipid levels; however, it significantly reduced intrahepatic fat accumulation in the cirrhotic rats. Furthermore, ezetimibe reduced systemic and intrahepatic ox-LDL levels and ameliorated systemic oxidative stress and inflammation as evidenced by the reduction in plasma levels of TBARS and TNF-α. Despite the anti-inflammatory and anti-oxidative stress effects, 4 weeks of ezetimibe treatment did not improve hepatic inflammation or liver fibrosis in the cirrhotic rats in the present study.
Our results also showed prominent ox-LDL accumulation in the livers of the BDL rats, which is consistent with a previous report.16 In addition, we also found that the BDL rats had increased oxidative stress compared to the sham-operated rats. The oxidative stress in prolonged cholestasis may have enhanced the oxidative modification of LDL in the livers of the BDL rats.16 On the other hand, the ox-LDL accumulation in the livers of the BDL rats may have been due to the reduced excretion of ox-LDL from bile after BDL.20 In addition, chronic inflammation and intrahepatic fat accumulation also play important roles in the increased levels of ox-LDL in cirrhotic livers.
Ox-LDL is taken up by macrophages in systemic vasculatures through scavenger receptors, such as LOX-1.21 Ox-LDL has been shown to induce tissue factor expression in T-lymphocytes via activation of LOX-1.22 In addition, Kupffer cells have been shown to have specific membrane receptors which act as scavenger receptors for ox-LDL.6 Hypoxia triggers oxidative stress, and LOX-1 mediates reactive oxygen species generation in different cells. In addition, ox-LDL has been shown to have an LOX-1-dependent profibrotic effect in cardiac myofibroblasts, because this effect could be abolished by LOX-1 knockdown.23 LOX-1 knockdown has also been shown to significantly ameliorate cardiac cell hypertrophy through a reduction in reactive oxygen species.24 Increased serum levels of soluble LOX-1 accompanied by elevated ox-LDL levels have been reported in patients with nonalcoholic fatty liver disease, indicating the significant role of LOX-1 in modulating ox-LDL.25 The modulatory roles of LOX-1 on fibrosis, apoptosis, and inflammatory pathways have also been documented.26 Interestingly, although the overexpression of LOX-1 has been shown to mediate portal venous inflammation in patients with nonalcoholic steatohepatitis, the association between ox-LDL and LOX-1 remains uncertain in cirrhotic patients.1 A previous report reported very low LOX-1 expressions in fibrotic livers, in contrast to the obvious ox-LDL accumulation in cirrhotic livers.1 We also found that the BDL-induced cirrhotic rats had prominent hepatic ox-LDL accumulation but decreased LOX-1 protein expression compared to the sham-operated rats. A possible explanation may be that LOX-1 from Kupffer cells plays the major scavenger role for ox-LDL in non-cirrhotic sinusoidal parenchyma, but that this effect is dysfunctional or lacking in a cirrhotic liver. Another possible explanation is that the elimination of ox-LDL in cirrhotic livers may be performed via a non-LOX-1 pathway, such as cluster of differentiation 36 scavenger system.6 Therefore, further investigations are needed to clarify the mechanism of ox-LDL elimination and the contribution of LOX-1 to liver fibrosis in cirrhotic livers. An interesting finding of this study is that the downregulation of LOX-1 protein expression was upregulated by ezetimibe treatment in the cirrhotic rats, which may play a role, at least in part, in eliminating ox-LDL in cirrhotic livers, although it could not reverse liver fibrosis under current experimental conditions.
We also found significantly upregulated IkBα and COX-2 and downregulated COX-1 and NCP1L1 protein expressions in the cirrhotic rats compared to the sham-operated rats. Although ezetimibe reduced plasma levels of TNF-α, it did not influence the hepatic expressions of the inflammatory indicators IkBα and COX-2, which is consistent with the finding that intrahepatic inflammation was not affected by ezetimibe. In addition, NPC1L1 protein expression was not regulated by ezetimibe, indicating that ezetimibe eliminated intrahepatic fat via a non-NPC1L1 pathway. Taken together, our data revealed that intrahepatic inflammation and fibrosis could not be alleviated by ezetimibe. This may be due to the severe liver damage induced by BDL, which was too overwhelming to overcome by ezetimibe.
On the other hand, ezetimibe did not affect systemic or portal hemodynamic data in the cirrhotic rats. Previous studies have reported that ezetimibe lacked obvious pleotropic effects compared to statins.27 In contrast to many experiments confirming the pleiotropic effect of statins, there is still insufficient evidence of the pleiotropic effect of ezetimibe.28 Similarly, our data showed that portal hypertension and hyperdynamic circulation could not be reversed by 4 weeks of ezetimibe treatment. The factors contributing to portal hypertension include portal venous flow and liver stiffness. Because ezetimibe does not appear to affect either portal venous flow or PP, its effect on intrahepatic resistance may be neutral.
In conclusion, 4 weeks of ezetimibe treatment mitigated intrahepatic fat accumulation, oxidative stress, and reduced ox-LDL levels in rats with BDL-induced liver cirrhosis. However, hepatic inflammation and fibrosis were not ameliorated. Because ezetimibe treatment exerts some beneficial effects and is relatively safe in cirrhosis, further clinical investigations may be warranted.
ACKNOWLEDGMENTSThe authors acknowledge the Clinical Research Core Laboratory of Taipei Veterans General Hospital for providing the experimental space and facilities. This work was supported by grants from the Taipei Veterans General Hospital (V111C-060), the National Science and Technology Council (MOST 111-2314-B-A49-059-MY3), and the Szu-Zuan Research Foundation of Internal Medicine (grant nos. 111025), Taipei, Taiwan. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
REFERENCES 1. Ho CM, Ho SL, Jeng YM, Lai YS, Chen YH, Lu SC, et al. Accumulation of free cholesterol and oxidized low-density lipoprotein is associated with portal inflammation and fibrosis in nonalcoholic fatty liver disease. J Inflamm (Lond). 2019;16:7. 2. McGettigan B, McMahan R, Orlicky D, Burchill M, Danhorn T, Francis P, et al. Dietary lipids differentially shape nonalcoholic steatohepatitis progression and the transcriptome of kupffer cells and infiltrating macrophages. Hepatology. 2019;70:67–83. 3. Tomita K, Teratani T, Suzuki T, Shimizu M, Sato H, Narimatsu K, et al. Free cholesterol accumulation in hepatic stellate cells: mechanism of liver fibrosis aggravation in nonalcoholic steatohepatitis in mice. Hepatology. 2014;59:154–69. 4. Van Rooyen DM, Larter CZ, Haigh WG, Yeh MM, Ioannou G, Kuver R, et al. Hepatic free cholesterol accumulates in obese, diabetic mice and causes nonalcoholic steatohepatitis. Gastroenterology. 2011;141:1393–403. 5. Van den Berg VJ, Vroegindewey MM, Kardys I, Boersma E, Haskard D, Hartley A, et al. Anti-oxidized LDL antibodies and coronary artery disease: a systematic review. Antioxidants (Basel). 2019;8:484. 6. Schneiderhan W, Schmid-Kotsas A, Zhao J, Grünert A, Nüssler A, Weidenbach H, et al. Oxidized low-density lipoproteins bind to the scavenger receptor, CD36, of hepatic stellate cells and stimulate extracellular matrix synthesis. Hepatology. 2001;34(4 Pt 1):729–37. 7. Houben T, Oligschlaeger Y, Bitorina AV, Hendrikx T, Walenbergh SMA, Lenders MH, et al. Blood-derived macrophages prone to accumulate lysosomal lipids trigger oxLDL-dependent murine hepatic inflammation. Sci Rep. 2017;7:12550. 8. Nakhjavani M, Mashayekh A, Khalilzadeh O, Asgarani F, Morteza A, Omidi M, et al. Oxidized low-density lipoprotein is associated with viral load and disease activity in patients with chronic hepatitis C. Clin Res Hepatol Gastroenterol. 2011;35:111–6. 9. Miura K, Ohnishi H, Morimoto N, Minami S, Ishioka M, Watanabe S, et al. Ezetimibe suppresses development of liver tumors by inhibiting angiogenesis in mice fed a high-fat diet. Cancer Sci. 2019;110:771–83. 10. Toyoda Y, Takada T, Umezawa M, Tomura F, Yamanashi Y, Takeda K, et al. Identification of hepatic NPC1L1 as an NAFLD risk factor evidenced by ezetimibe-mediated steatosis prevention and recovery. FASEB Bioadv. 2019;1:283–95. 11. Franco F, Gigou M, Szekely AM, Bismuth H. Portal hypertension after bile duct obstruction: effect of bile diversion on portal pressure in the rat. Arch Surg. 1979;114:1064–7. 12. Cameron GR, Muzaffar Hasan S. Disturbances of structure and function in the liver as the result of biliary obstruction. J Pathol Bacteriol. 1958;75:333–49. 13. Albillos A, Colombato LA, Groszmann RJ. Vasodilatation and sodium retention in prehepatic portal hypertension. Gastroenterology. 1992;102:931–5. 14. Abraldes JG, Iwakiri Y, Loureiro-Silva M, Haq O, Sessa WC, Groszmann RJ. Mild increases in portal pressure upregulate vascular endothelial growth factor and endothelial nitric oxide synthase in the intestinal microcirculatory bed, leading to a hyperdynamic state. Am J Physiol Gastrointest Liver Physiol. 2006;290:G980–7. 15. Chang YY, Chou CH, Chiu CH, Yang KT, Lin YL, Weng WL, et al. Preventive effects of taurine on development of hepatic steatosis induced by a high-fat/cholesterol dietary habit. J Agric Food Chem. 2011;59:450–7. 16. Karadeniz G, Acikgoz S, Tekin IO, Tascýlar O, Gun BD, Cömert M. Oxidized low-density-lipoprotein accumulation is associated with liver fibrosis in experimental cholestasis. Clinics (Sao Paulo). 2008;63:531–40. 17. Chang E, Kim L, Park SE, Rhee EJ, Lee WY, Oh KW, et al. Ezetimibe improves hepatic steatosis in relation to autophagy in obese and diabetic rats. World J Gastroenterol. 2015;21:7754–63. 18. Terunuma S, Kumata N, Osada K. Ezetimibe impairs uptake of dietary cholesterol oxidation products and reduces alterations in hepatic cholesterol metabolism and antioxidant function in rats. Lipids. 2013;48:587–95. 19. Loomba R, Sirlin CB, Ang B, Bettencourt R, Jain R, Salotti J, et al.; San Diego Integrated NAFLD Research Consortium (SINC). San Diego Integrated NAFLD Research Consortium (SINC). Ezetimibe for the treatment of nonalcoholic steatohepatitis: assessment by novel magnetic resonance imaging and magnetic resonance elastography in a randomized trial (MOZART trial). Hepatology. 2015;61:1239–50. 20. Cömert M, Tekin IO, Acikgöz S, Ustündağ Y, Uçan BH, Acun Z, et al. Experimental bile-duct ligation resulted in accumulation of oxidized low-density lipoproteins in BALB/c mice liver. J Gastroenterol Hepatol. 2004;19:1052–7. 21. Mitra S, Goyal T, Mehta JL. Oxidized LDL, LOX-1 and atherosclerosis. Cardiovasc Drugs Ther. 2011;25:419–29. 22. Cimmino G, Cirillo P, Conte S, Pellegrino G, Barra G, Maresca L, et al. Oxidized low-density lipoproteins induce tissue factor expression in T-lymphocytes via activation of lectin-like oxidized low-density lipoprotein receptor-1. Cardiovasc Res. 2020;116:1125–35. 23. Villa M, Cerda-Opazo P, Jimenez-Gallegos D, Garrido-Moreno V, Chiong M, Quest AF, et al. Pro-fibrotic effect of oxidized LDL in cardiac myofibroblasts. Biochem Biophys Res Commun. 2020;524:696–701. 24. Zhu TT, Zhang WF, Luo P, Qian ZX, Li F, Zhang Z, et al. LOX-1 promotes right ventricular hypertrophy in hypoxia-exposed rats. Life Sci. 2017;174:35–42. 25. Ozturk O, Colak Y, Senates E, Yilmaz Y, Ulasoglu C, Doganay L, et al. Increased serum soluble lectin-like oxidized low-density lipoprotein receptor-1 levels in patients with biopsy-proven nonalcoholic fatty liver disease. World J Gastroenterol. 2015;21:8096–102. 26. Taye A, El-Sheikh AA. Lectin-like oxidized low-density lipoprotein receptor 1 pathways. Eur J Clin Invest. 2013;43:740–5. 27. Woźniak E, Broncel M, Niedzielski M, Woźniak A, Gorzelak-Pabiś P. The effect of lipid-lowering therapies on the pro-inflammatory and anti-inflammatory properties of vascular endothelial cells. PLoS One. 2023;18:e0280741. 28. Niedzielski M, Broncel M, Gorzelak-Pabiś P, Woźniak E. New possible pharmacological targets for statins and ezetimibe. Biomed Pharmacother. 2020;129:110388.
留言 (0)